Article Text

Abstract
Problem Effective and affordable health systems have good primary care. Access, equity, care of chronic conditions and quality are key priorities in primary care in Australia.
Design A large-scale quality improvement collaborative addressing diabetes, coronary heart disease (CHD), access, chronic obstructive pulmonary disease (COPD), patient self-management, Aboriginal health and diabetes prevention.
Setting General practices and Aboriginal medical services across Australia.
Key Measures for Improvement Sample measures are reported.
Strategy for Change The Improvement Foundation (Australia) adapted collaborative strategies used in the UK. Health service teams attended three workshops, separated by activity periods and followed by 12 months of further work. Teams were supported by local collaborative program managers to make changes and report measures. Services received feedback about improvement compared with their wave.
Effects of Change 1185 health services participated in 13 waves between 2005 and 2011. 83% of Australian divisions of general practice participated, and 262 support staff received quality improvement training. Key measures show improvement in all topics except access. 397 111 patients were on the disease registers of participating health services.
Lessons learnt The collaborative methodology is transferable to primary care in Australia. Results may reflect improved data recording and disease coding, as well as changes in clinical care. Team dynamics and local support are important success factors. Collaboratives are a useful tool in a program of clinical quality improvement. The APCC will work with the new primary healthcare organisations which are part of health reforms in Australia to improve data reporting, improve diabetes care and entrench quality improvement in the emerging environment.
- General practice
- quality improvement
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/3.0/ and http://creativecommons.org/licenses/by-nc/3.0/legalcode
Statistics from Altmetric.com
Introduction
Since 2004, the Australian Primary Care Collaborative (APCC) Program has applied the quality improvement collaborative (QIC) methodology of the Institute for Healthcare Improvement1 to primary care in Australia. The first APCC program waves were adapted from work by the National Primary Care Development Team2 in England and addressed diabetes, coronary heart disease (CHD) and access to care. Later, waves were developed by the Improvement Foundation (Australia) to address chronic obstructive pulmonary disease (COPD), prevention, patient self-management, Aboriginal health and diabetes prevention. The APCC aims to have a systems impact intervening at multiple levels to increase capacity for quality improvement within the primary care sector.
Effective and affordable health systems have strong primary care.3 A recent major government review of primary care in Australia identified access and equity, care of chronic conditions and quality improvement as key priorities.4 ,5 International comparisons indicate that Australia needs to improve primary care services.6 ,7
The common characteristics of QICs have been well described.8–10 While there remain questions about their cost effectiveness9 there is evidence of effectiveness in improving targeted topics10 together with evidence of positive spill-over effects on participating teams in other areas of care and enthusiasm for improvement.11 ,12 Mittman and others note that QICs are arguably the most important response yet to the health quality chasm, and call for rigorous mixed-method evaluation to identify factors which determine their success.8 ,11 ,13–15
This article records the APCC as an example of successful international spread of a large improvement initiative. It describes a methodology for implementing national-level primary care improvement using QICs, gives a snapshot of some of the measures collected, and provides insight into success in engagement with the sector. More detailed analyses of results and lessons in individual topics will be provided in subsequent articles.
Context
The Australian environment
Approximately 20 000 general practitioners (GPs)16 work in 7200 practices17 to serve 22 million Australians.16 On average, an Australian sees a GP 5.3 times per year, and 83% of Australians will attend a GP in a calendar year.16 General practices are usually small businesses, however, an increasing proportion of the sector is owned by large corporations. Australians receive universal health insurance through the national government which reimburses all or part of the fee charged. Practices are supported by a network of regional, mainly government funded, independent organisations called ‘divisions of general practice’.
Alongside mainstream general practices, a network of Aboriginal medical services (AMS)18 have developed which focus on the Aboriginal community. Australian Aboriginal and Torres Strait Islander peoples have a life expectancy 17 years less than non-Indigenous people.19 Closing this gap is a high priority within the health system.
Key measures for improvement
A suite of measures was developed for each topic addressed in the APCC. A selection of these is reported here to provide a sample of the results within the program (table 1).
Sample key measures
Assessment of the problem
The Australian Government Department of Health and Ageing identified the potential value of employing the QIC methodology to improve primary care. The ‘Breakthrough’ collaborative approach was developed in the USA and was used in large-scale application in the UK by the National Primary Care Development Team (NPDT) in the National Primary Care Collaborative. The change principles and ideas for the first three topics of the APCC were adapted from those used by the NPDT.
An expert reference panel (ERP) was convened at the commencement of each topic, and was made up of academic experts to provide best evidence, clinical experts to provide experience with frontline implementation and improvement experts. An aim was determined for each topic (table 2). Under each aim, a series of detailed change principles and change ideas were developed by the ERP based on best evidence and practicalities of implementation.
Aims for each topic in the APCC
Measures
An ERP selected the improvement measures for each topic based on best evidence and practicality of collection of measures in the busy clinical context. Implementation of successive topics has necessitated the development of new measures. Measures need to have face validity for clinicians and reflect actual improvements, while being as easy as possible to collect and report. A wide range of measures are now available to practices.20 As examples, core measures of the first three topics are listed in box 1.
Monthly measures for access, diabetes and coronary heart disease (Phase 1)
Access
-
Percentage of patients seen by the practice on their day of choice
-
Number of days until GP's third available appointment
-
Number of days until nurse's third available appointment
Diabetes
-
Number of patients on the diabetes register
-
Percentage of patients with measured HbA1c≤7
-
Percentage of patients with measured total cholesterol <4 mmol/litre
-
Percentage of patients with recorded blood pressure ≤130/80
-
Percentage of patients with diabetes service incentive payment claimed
CHD
-
Number of patients on the CHD register
-
Percentage of patients with CHD on a statin
-
Percentage of patients who have had a myocardial infarction in the past 12 months and who are on beta blockers
-
Percentage of patients with CHD with recorded blood pressure <140/90
Improvement measures are collected monthly. Feedback is provided monthly to health services (general practices and AMS) about their improvement measures compared with their wave. Participants in early waves used software to extract or identify clinical measures and manually entered the data via the web. Most clinical measures are now uploaded electronically.
Strategies for improvement
Establishing the APCC
With funding of AU$19 million, the Australian Government commissioned a central organisation, Flinders Consulting, to implement the Collaboratives program in the context of primary care in Australia. Two Australian teams trained in the UK with the NPDT. During early implementation, key staff members from the NPDT travelled to Australia to facilitate implementation. The model established by the NPDT was followed in seeking to engage primary care at practice and regional level. Considerable intellectual property was shared by the NPDT.
Phase 1
Phase 1 involved building the APCC central office team, building knowledge about running collaboratives, event management, training of Collaborative Program Managers (CPMs), constructing support tools to extract data from existing clinical software and identification of exemplars. It was strategic to build links with existing state and national-level primary care organisations which were initially wary. During the first phase, health services began to ask for help with building their teams. A ‘Team Change Principle’ was designed and incorporated into the access topic. The first phase was implemented in three national waves addressing diabetes, coronary heart disease (CHD) and access, and spread through local waves and two virtual waves.
Phase 2
After evaluation, a second phase was funded with approximately AU$23 million. The Improvement Foundation (Australia) Ltd tendered successfully for the second phase. Funding changes required a reduction in scope. The Access topic did not demonstrate the change seen in measures for diabetes and CHD in Phase 1. The review and rewrite of this topic and measures for Phase 2 are discussed elsewhere.21 The topic was renamed ‘Access and Care Redesign’ to reflect the perceived importance of organisational improvement to support chronic disease care improvement.
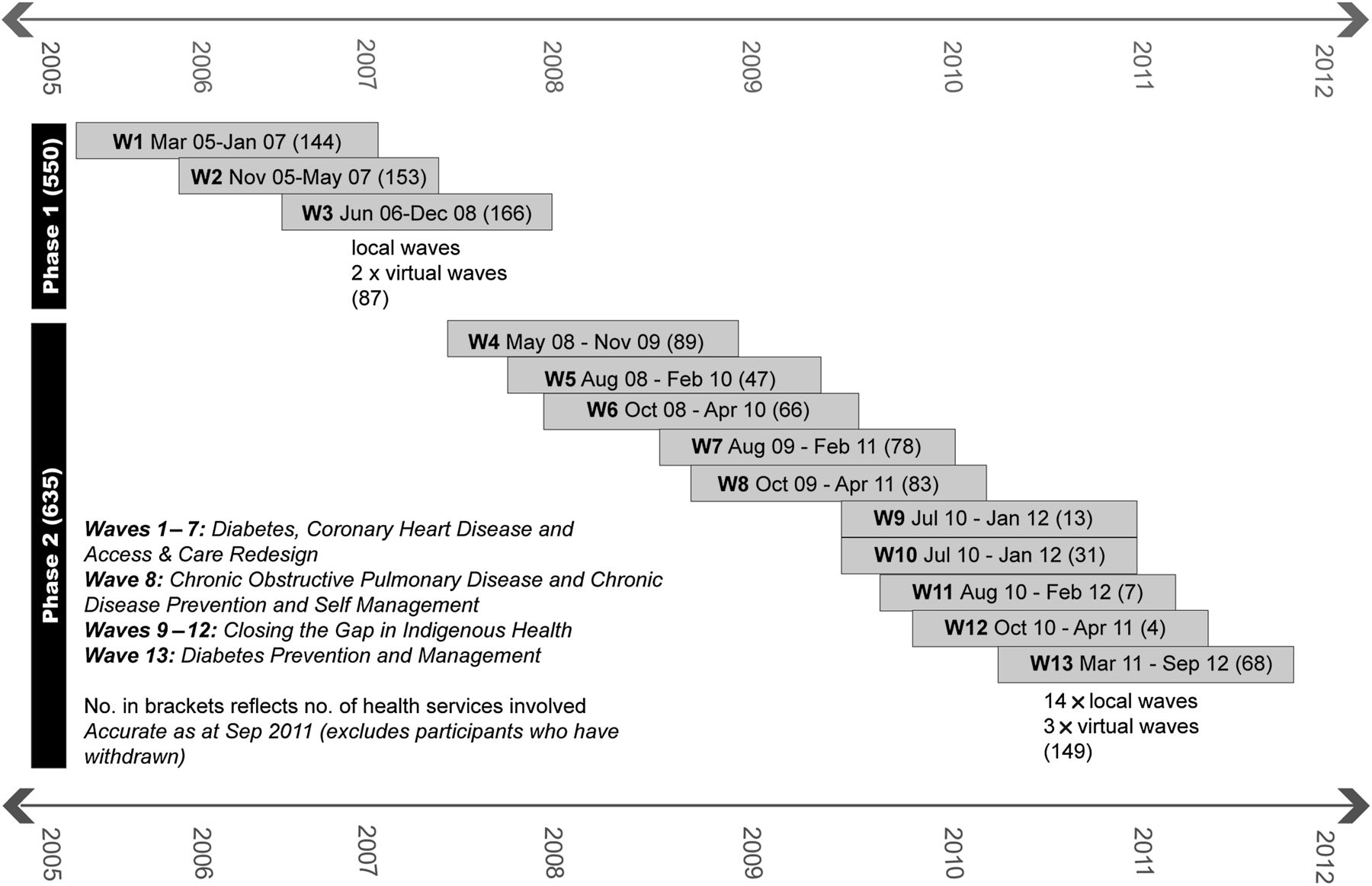
Diabetes, CHD and access topics were delivered in four state-based waves. Later, additional funding allowed waves addressing chronic obstructive pulmonary disease (COPD), prevention and patient self-management to be developed. More recently, waves addressing Aboriginal and Torres Strait Islander health and diabetes prevention have commenced. These topics have been developed in Australia by the Improvement Foundation in response to locally identified problems and funding opportunities using the expertise gained from implementing the first three topics. In response to requests from remote health services and to promote spread, 14 smaller local waves and three virtual waves occurred in phase 2 (see figure 2).
Engaging with health services
Divisions of general practice were invited to participate in the APCC and were asked to recruit and support participating health services. Health services were offered partial expenses and contracted to dedicate a clinician and administrator to attend all workshops. They were supported by a CPM placed in the local division of general practice. The CPM is trained and funded by the APCC and is a pivotal role, reinforcing learning from workshops, helping health services report data and supporting them in quality improvement initiatives.
Initially, there was some resistance to participation in the APCC in some states, and from some stakeholders in the health system. Support of key clinical leaders, positive results and a track record of good faith appear to have increased acceptance of the role of the APCC in the seven years since it began.
The intervention
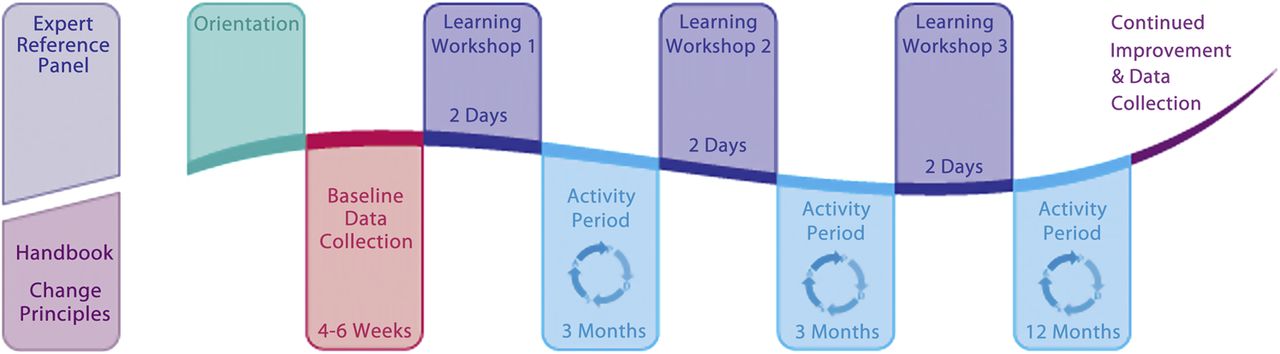
Small teams from each health service attended three learning workshops at which they learnt the change principles for the topic, the measures and the Langley and Nolan model for improvement.22 The workshops generated enthusiasm and a shared purpose, and provided a context for exchanging ideas.
During activity periods between workshops, health services submitted the monthly improvement measures, Plan/Do/Study/Act (PDSA) cycles and implemented the change principles with the support of their CPM. After the third learning workshop, supported improvement work continued for 12 months (see figure 1).

Diagram of APCC wave.
Health services received regular reports of their change measure progress compared against their ‘wave’. They shared their ideas and strategies in local groups, through list servers and at the learning workshops, often building a sense of shared commitment to the project. Emerging clinical leaders contributed to subsequent workshops and waves.
In an effort to reduce costs and increase effectiveness, wave 13 (diabetes prevention) is trialling a new collaborative format involving two central face-to-face workshops separated by a series of virtual workshops.
Effects of change
Participation
One thousand three hundred and eight health services commenced the APCC and 123 withdrew (9%). One thousand one hundred and thirty-two general practices (16% of 7119 practices) and 53 AMSs have completed, or continue to participate in the APCC, giving a total of 1185 participating health services. Of the 111 divisions of general practice in Australia, 93 (83%) have been involved. Two hundred and sixty-two division staff members have received training in quality improvement and the collaborative methodology.
Health services that failed to submit data or PDSA cycles were offered support and were eventually withdrawn from the program if they were unable to meet minimum standards of participation.
The APCC has been implemented in 13 national/state waves of health services (figure 2). Some health services have participated in more than one topic, but in general, each wave comprised a new cohort of health services.
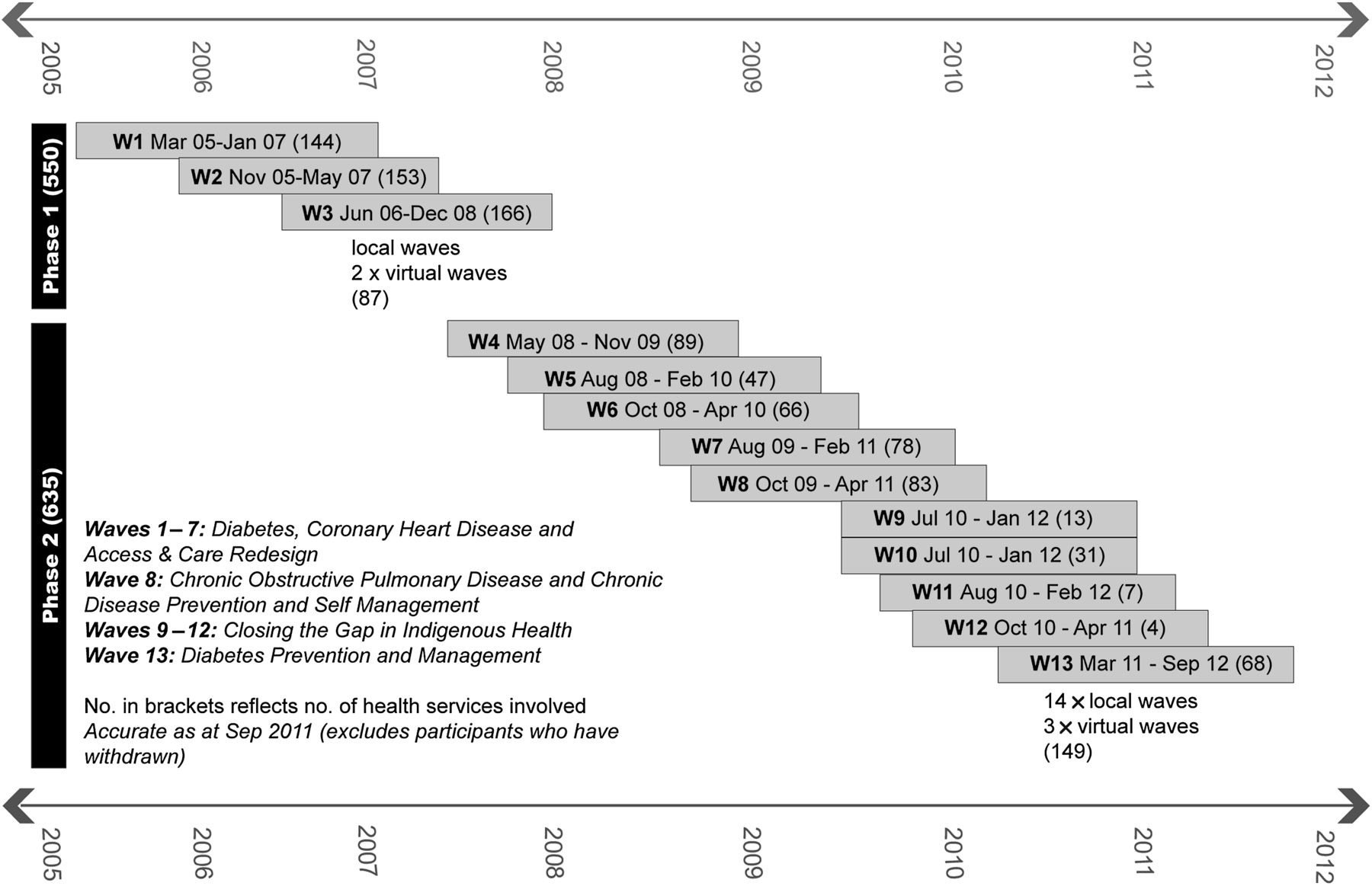
Timeline of waves and phases.
Changes in sample key improvement measures in each topic
-
Diabetes see figure 3
-
CHD see figure 4
-
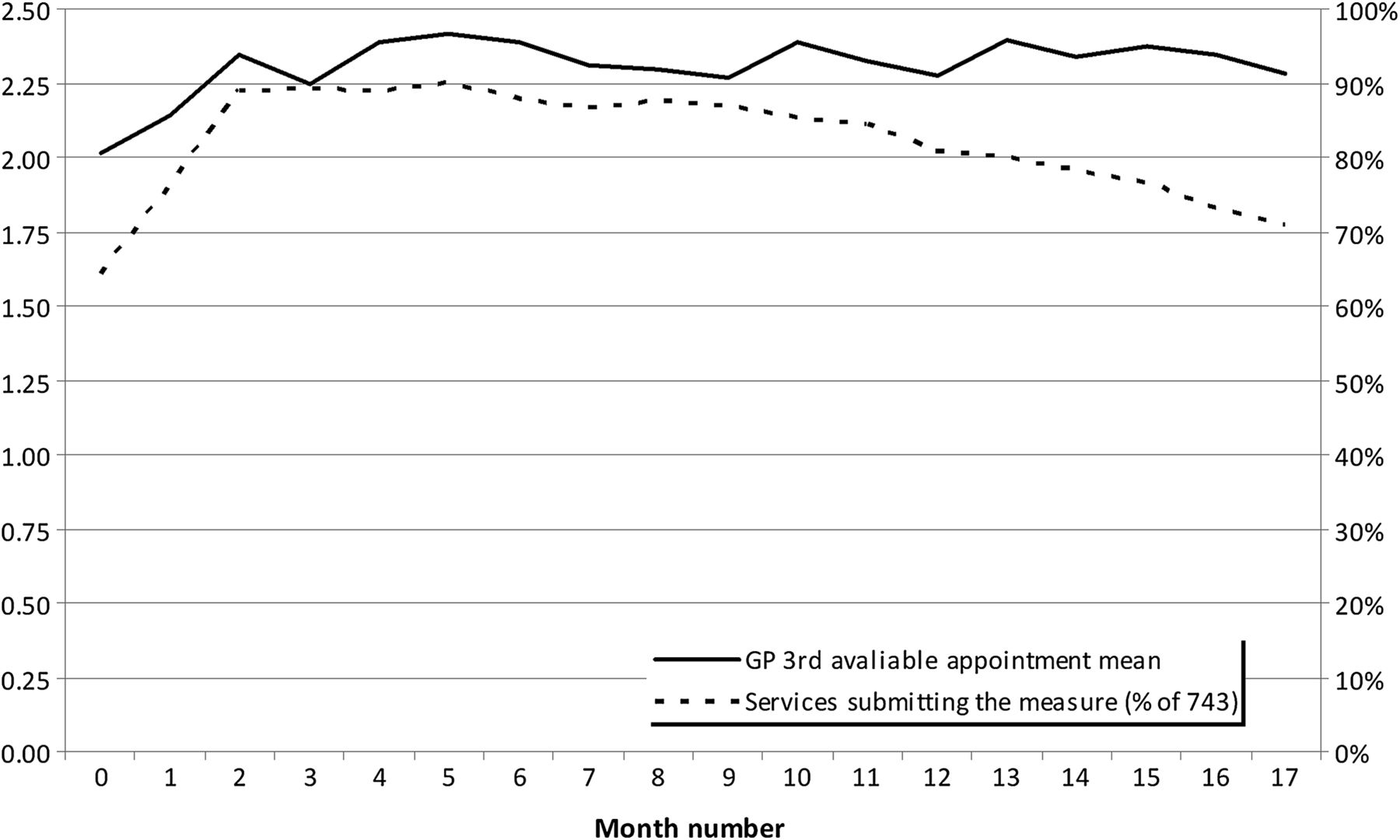
Access see figure 5
-
COPD see figure 6
-
Chronic Disease Patient Self-Management see figure 7
-
Closing the Gap see figure 8.
Patients served by the APCC
Table 3 records the number of patients with heart disease and diabetes appearing on disease registers of health services participating in the APCC. The number of patients with diabetes on the registers is approximately 6% of the estimated total number of patients with diabetes in Australia.23
Number of patients on disease registers of participating health services
Improvement cycles reported by participating health services
Participating health services were required to submit written reports of PDSA cycles undertaken within their organisations. Table 4 reports figures for reported cycles from participating health services.
PDSA cycle reports submitted by participating health services
Data quality and reporting
Health services reported single points of baseline data which, for practical purposes, were collected before patient lists were cleansed or disease registers validated. The access measures required manual calculation and input onto the APCC data collection web portal. De-identified aggregated clinical measures are now collected by direct upload from third-party software that interrogates data from within health service clinical information systems.
Data reporting was mandatory for the 18 months of wave involvement. Some health services have continued to report data since their wave finished.
System changes associated with the APCC
The clinical software data extraction tools which the APCC initiated are now in widespread use across Australia in many health services that have not participated in the APCC. This process has begun to drive software development as health services become increasingly sophisticated in their expectations. The tools are being used by health services and divisions to collect national performance indicators, some of which are based on the improvement measures developed for the APCC. The web portal designed for use within the APCC has provided significant lessons that have contributed to the development of a new web portal for reporting and feedback of quality improvement indicators for the Aboriginal Community Controlled Health Service sector. Many divisions of general practice are using the QIC approach to implement other improvements as part of their respective missions.
Lessons and next steps
The APCC has demonstrated that the QIC methodology can be implemented in primary care in Australia for multiple topics, and over an extended period of time. It is the largest continuous, primary care collaborative program yet published. The program exceeds the Vermont Oxford Network, the Veterans Health Administration program and the Health Resources and Services Administration Health Disparities series in the number of health services participating. In 8 years, the APCC has engaged with 400 000 patients. The largest continuous specialist collaborative, the Vermont Oxford Network program, has engaged with 1 million neonates in 22 years.
The results show engagement with a large proportion of the sector. We have reported a sample of results which demonstrate some of the changes that have been measured. Most topics have shown improvement in the measures. In an uncontrolled implementation project such as this, it is not possible to determine to what extent this reflects change in clinical care or changes in data quality. There may have been background environmental changes which affected the measures collected.
Improvement in APCC measures may in part be due to improved skills in disease register formation, cleaning and data collection, rather than changes in clinical care. Health services concentrated on these processes early in their improvement journey. As time progressed, they turned their attention to focus more on redesigning clinical care. It is not possible to determine which part of the intervention resulted in the changes in measures. Increased evaluation of QICs as they are being implemented, may help improve understanding of which parts of the intervention are most important for improvement, and which topics are most appropriate for QICs.
There has been variability in data reporting across and within topics. The cholesterol and the Aboriginal health measures reported are examples of relatively low reporting levels. Other evaluations of QICs have noted that achieving high rates of measure reporting can be challenging. Where measures are collected electronically from clinical health records and electronically uploaded, the APCC has achieved very high rates of data reporting (eg, HbA1C, GP management plans measures). Those contemplating implementing QICs should seek ways to make data collection as easy as possible for busy clinical teams.
Ovretveit et al 8 identify 10 recommendations for increasing the effectiveness of improvement through QICs of which six relate to health service team dynamics (see box 2). Feedback from participating teams supported the findings of previous evaluations of QICs that the functioning of clinical teams is very important for success in improvement. The APCC response to requests from teams was to produce resources and provide training to guide them in improving their team health. Workshops were designed to give teams time to plan, and CPMs were trained to provide further support.
Recommendations for increasing the chances of achieving successful spread of quality improvement through QICs. Ovretveit et al8
Recommendations for preparation and defining purpose
-
Choose the right type of subject.
-
Ensure participants define objectives for taking part, and assess their capacity to benefit from the collaborative.
-
Define roles and make clear what is expected.
-
Ensure team building and preparation by teams for the collaborative.
Recommendations for organising and running meetings
-
Emphasise mutual learning rather than teaching.
-
Pay attention to motivating and empowering teams.
-
Ensure teams have measurable and achievable targets.
-
Equip and support teams to deal with data and change challenges.
Recommendations for post-collaborative transition
-
Learn and plan for sustaining improvements, involving managers in this work.
-
Plan and learn for ‘spread’.
As well as improving clinical care, the APCC was designed to increase knowledge and skills in the sector about quality improvement. The spread of some APCC measures to be used as national key performance indicators, and the use of APCC tools, more widely suggest that the APCC has had a significant effect on primary care culture. In particular, software solutions for quality indicator collection developed for the APCC are now in widespread use providing a capability which did not previously exist.
In many of the topics, the APCC saw strong improvements in measures supporting previous findings that QICs are effective interventions. Even with strong improvements, there remain gaps which demonstrate that QICs are a partial solution to improving patient care. QICs appear to be effective for the right topic and for rapid change. Additional policy levers are required if patients are to receive the right care on all occasions.
By creating a small team and a decentralised structure that delivers a series of collaborative waves nationally, expertise in quality improvement, logistics and engagement with clinical teams and their supports has been built. The APCC demonstrates a possible strategy for improving primary healthcare that other health systems may consider.
While there has been some attempt to institutionalise the behaviours learnt in the APCC, there remains room for more effort in building systems and processes to ensure that the behaviours in clinical performance, improvement methodologies and sharing of experiences become entrenched in the Australian primary care sector, as recommended by Ovretveit et al 8 (box 2).
The APCC has had a significant impact on the Australian primary care sector. It has demonstrated success in engagement of health services and support structures, in promoting knowledge and in providing tools to increase capacity for quality improvement. Further phases of the APCC will provide an opportunity for more comprehensive quantitative and qualitative evaluation to further understand the component strategies and optimum use of QICs.
Next steps
Australia is currently undergoing health reforms. In this context, the Improvement Foundation will implement a third phase of the APCC. Current plans are for another national wave of diabetes improvement, and a wave working with the new regional primary healthcare organisations to support a quality improvement culture. Other work will use the QIC approach with primary healthcare services to pilot implementation of the new patient-controlled electronic health record in Australia.
Acknowledgments
The authors acknowledge the hard work and creativity of the many primary care health services that made the APCC possible.
References
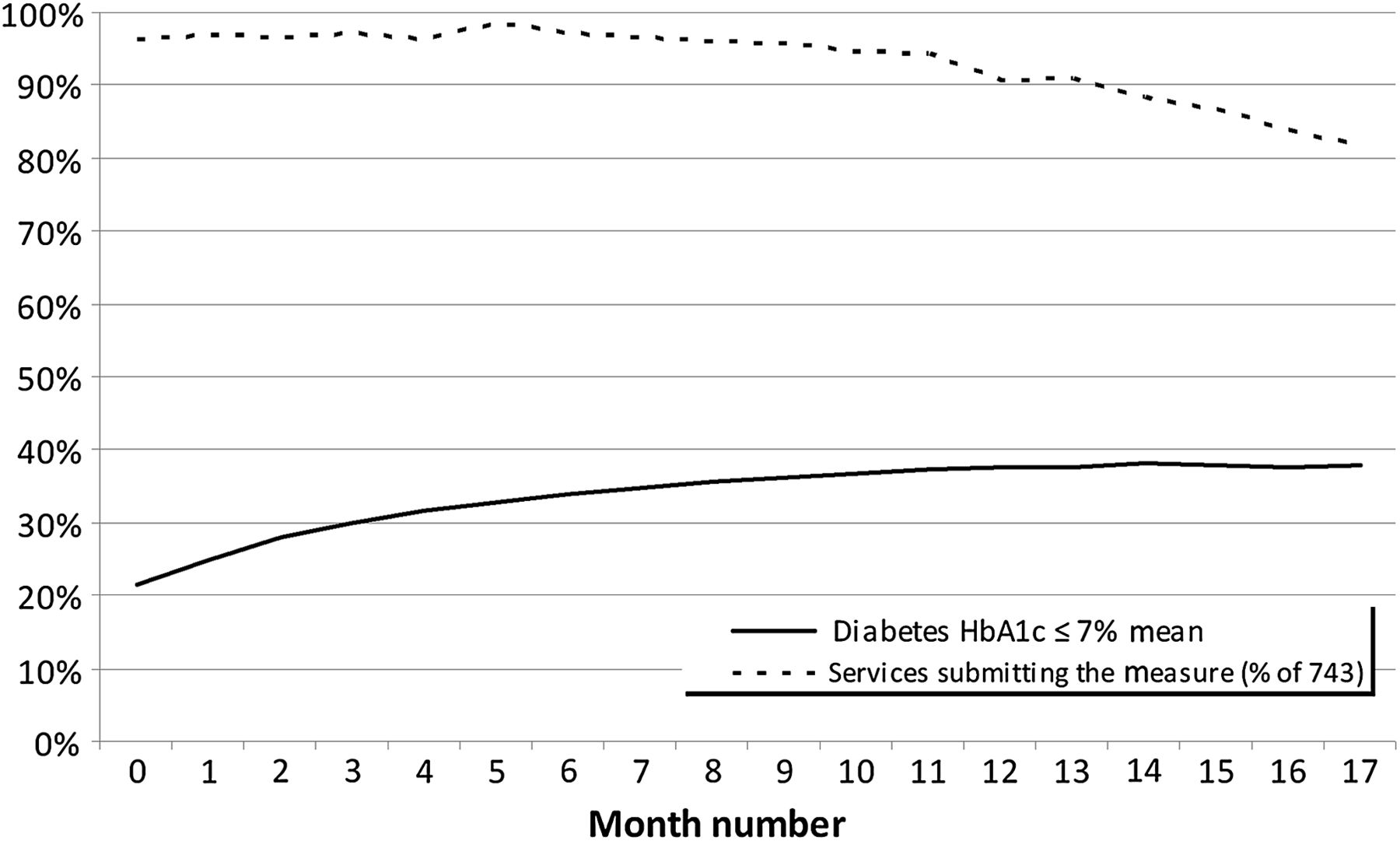
Mean percentage of patients in each health service achieving target HbA1C level (≤7 mmol/l).

Mean percentage of patients in each health service diagnosed with CHD achieving target cholesterol level (total cholesterol <4 mmol/l).
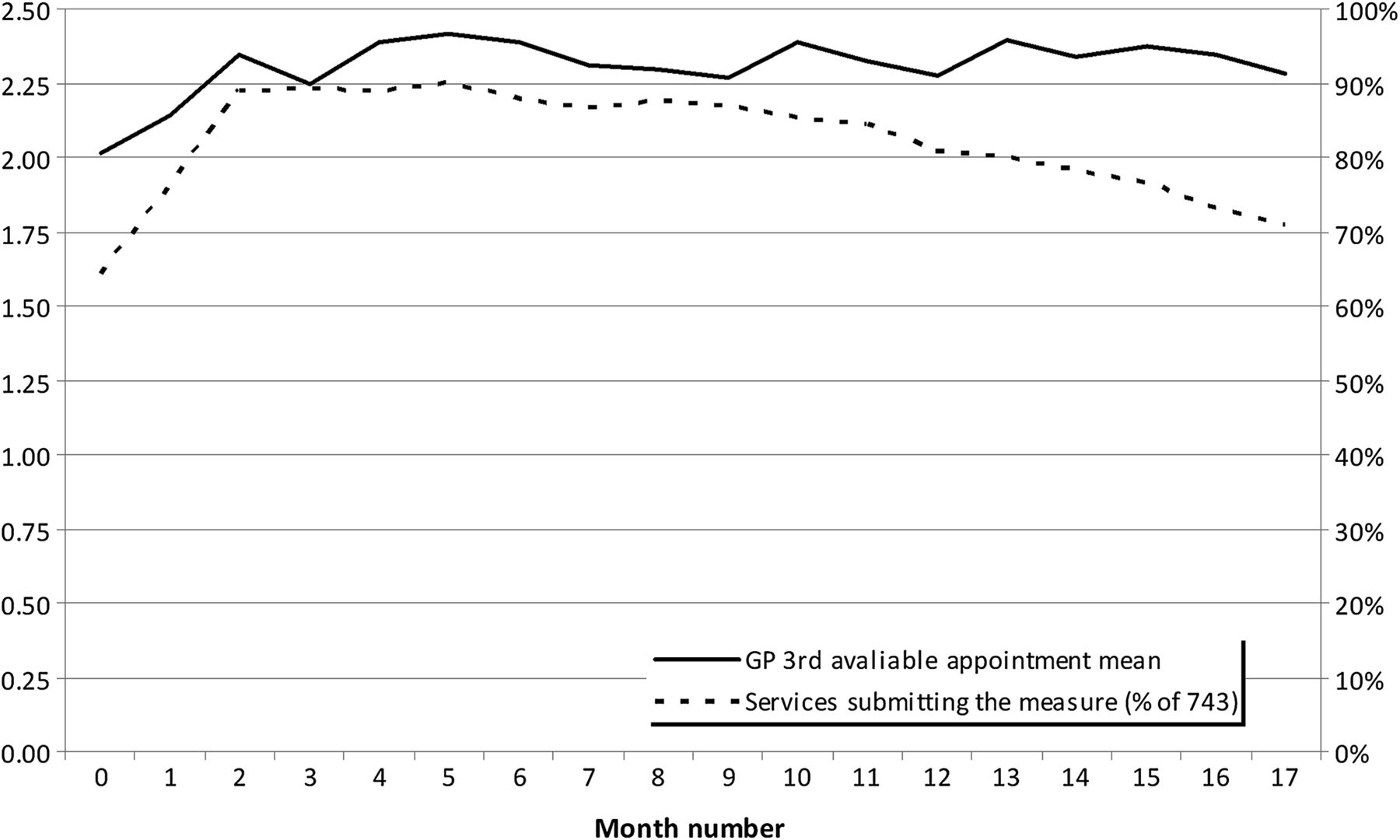
Days to third available GP appointment.

Mean percentage of patients diagnosed with COPD in each health service, who have spirometry recorded.
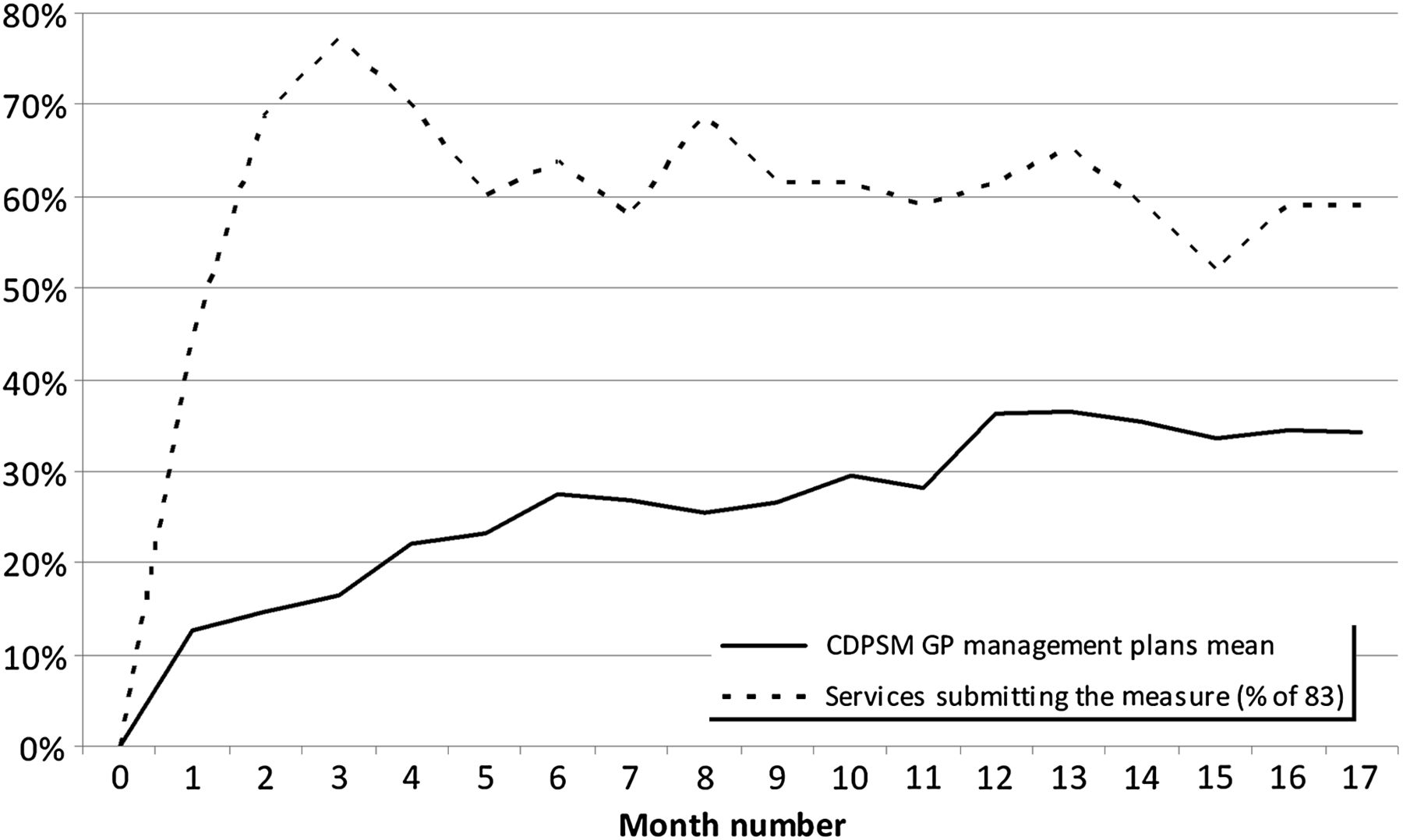
Mean percentage of patients with chronic disease in each health service, who have a GP management plan established.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Mean number of Aboriginal and Torres Strait Islander Health Checks per health service.
Footnotes
-
Funding The Australian Primary Care Collaboratives Program is funded by the Australian Government Department of Health and Ageing and delivered by the Improvement Foundation (Australia) Ltd.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement This article publishes a small indicative subset of the data collected by the APCC Program in the course of its improvement work. The complete dataset is held by the Improvement Foundation and is subject to agreements with participating health services which restrict its use. Researchers wishing to access the data may make direct contact with the Improvement Foundation (Australia).