Article Text

Abstract
Background Advancing the description and conceptualisation of interventions in complex systems is necessary to support spread, evaluation, attribution and reproducibility. Improvement teams can provide unique insight into how interventions are operationalised in practice. Capturing this ‘insider knowledge’ has the potential to enhance intervention descriptions.
Objectives This exploratory study investigated the spread of a comprehensive medication review (CMR) intervention to (1) describe the work required from the improvement team perspective, (2) identify what stays the same and what changes between the different sites and why, and (3) critically appraise the ‘hard core’ and ‘soft periphery’ (HC/SP) construct as a way of conceptualising interventions.
Design A prospective case study of a CMR initiative across five sites. Data collection included: observations, document analysis and semistructured interviews. A facilitated workshop triangulated findings and measured perceived effort invested in activities. A qualitative database was developed to conduct thematic analysis.
Results Sites identified 16 intervention components. All were considered essential due to their interdependency. The function of components remained the same, but adaptations were made between and within sites. Components were categorised under four ‘spheres of operation’: Accessibility of evidence base; Process of enactment; Dependent processes and Dependent sociocultural issues. Participants reported most effort was invested on ‘dependent sociocultural issues’. None of the existing HC/SP definitions fit well with the empirical data, with inconsistent classifications of components as HC or SP.
Conclusions This study advances the conceptualisation of interventions by explicitly considering how evidence-based practices are operationalised in complex systems. We propose a new conceptualisation of ‘interventions-in-systems’ which describes intervention components in relation to their: proximity to the evidence base; component interdependence; component function; component adaptation and effort.
- complexity
- healthcare quality improvement
- implementation science
- collaborative
- breakthrough groups
- clinical practice guidelines
Data availability statement
All data relevant to the study are included in the article or uploaded as supplemental information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- complexity
- healthcare quality improvement
- implementation science
- collaborative
- breakthrough groups
- clinical practice guidelines
Introduction
The reproduction of successful interventions in new settings is essential for maximising the benefits of treatments and innovations for patients and healthcare systems.1 2 However, it is recognised that spreading interventions is a significant challenge for healthcare teams and managers.2–6 Many promising initiatives fail to spread, remaining isolated within the local context in which they were created.1 7 This results in missed opportunities to improve patient care at scale and can lead to significant variation in care processes and outcomes across healthcare organisations.8 9
The difficulty in spreading interventions is often attributed to a lack of consideration for the complexity and variation among different healthcare settings.5 10–12 Healthcare organisations are increasingly recognised as complex systems (ie, systems that dynamically change overtime, where activities are interdependent and inter-related, and where system actors have agency and are self-organising).1 13–15 Therefore, the role of local variation and context must be understood in order to unpick the processes that lead to spread and optimise intervention functioning in new settings.16 This includes recognition of diverse work processes, organisational structures, people, and cultures which may support or hinder the intervention’s desired effects.17
Several theories, models and frameworks have been designed to conceptualise the spread of healthcare innovations.4 18–27 There is no consensus on optimal ways to spread an intervention, but the importance of defining an intervention and establishing a description of components of an initiative believed to be essential to its effectiveness is widely accepted as an important step.4 19 22 27
However, defining complex interventions is not straightforward. The limited ability of those outside of the system (eg, academics and policymakers) to fully design interventions in advance is recognised.28 29 People in the system have unique ‘insider knowledge’ about how things really work which can help identify facilitators and overcome barriers to success.30 Such knowledge is often tacitly held, and no one person has a comprehensive view of how a system works, nor how an intervention will operate in practice.22 30 Defining interventions therefore requires a complex process of intervention testing, clarification and improvement over time.22 31 32
Quality improvement (QI) approaches tend to focus on building capacity and competencies for people inside the system to understand and intervene in their local settings to achieve improvement goals.33 34 While this builds capacity for improvement within individual sites, historically there has been less emphasis on describing interventions to share learning between improvement sites,35–37 and as such this ‘insider knowledge’ is rarely made explicit or captured in easily shareable forms.30 38
There are limited examples of methodological approaches to describe and conceptualise intervention components from an insider perspective.28–30 Prospectively studying and working in partnership with improvement initiatives could improve our ability to capture the richness of intervention spread and make explicit the tacit knowledge that emerges during this process.39
This study aimed to co-produce a detailed description of an evidence-based intervention and capture how it was spread. The co-production of knowledge was achieved through a partnership: improvement team members brought expert clinical, practice and QI knowledge needed to understand and intervene in their local system; researchers brought expertise in observing, capturing and making sense of what happens, and finding patterns in the busy world of frontline practice.39
The focus of this research was to develop a more in-depth understanding of the intervention, namely, to describe how the intervention was operationalised, and the work required to do this. In particular, we were interested in understanding the extent to which a common or shared view of this work was experienced between sites, and what differences or adaptations emerged, and why.
To conceptualise the intervention, we examined the popular implementation constructs of ‘hard core’ and ‘soft periphery’ (HC/SP). The innovation diffusion model by Denis et al suggests that each intervention contains a theoretical ‘hard core’ that is ‘well defined and fixed’ and a ‘soft periphery’ that is ‘less clear and more flexible to manipulation by the adopting system’.19 40 In practice, this means aiming for fidelity to an intervention’s HC components, while the SP components could be adapted to fit new settings.
We felt that the HC/SP concept could provide a useful lens to conceptualise the intervention and address the question of ‘what stayed the same, and what changed?’ between sites. However, an exploration of the literature revealed that while HC/SP is commonly used, (including within many popular theoretical frameworks41–43), there is no consistent definition, with several authors proposing various definitions.4 19 44 For example, in contrast to Denis et al’s definition above, Greenhalgh et al define core components as ‘the irreducible elements of the innovation itself’ and peripheral components as ‘the organisational structures and systems required for the full implementation of the innovation’.4 The Medical Research Council (MRC) uses ‘core components’ interchangeably with ‘active ingredients’, defined as ‘essential to achieving good outcomes for consumers at an implementation site’. The peripheral components can then be defined as those that can be adapted without impacting outcomes.44
A small number of studies have attempted to define the HC/SP of complex interventions.45–49 However, these studies have included only high-level descriptions of the HC/SP made in advance or post-hoc and were not based on structured empirical study. With little work done to assess these theoretical constructs or provide guidance on their practical application, we recognised an opportunity to critically appraise the HC/SP construct within our empirical case study.50–53
Our research therefore had three objectives:
To describe the work required to operationalise evidence-based practice from the perspective of improvement team members.
To identify what stayed the same and what changed between the different sites and why.
To critically appraise the ‘HC’ and ‘SP’ construct as a way of conceptualising interventions in complex systems.
Methods
Study setting
This study took place under the National Institute for Health Research Collaboration for Leadership in Applied Health Research and Care Northwest London. The purpose of the programme was to investigate how to support frontline care teams to translate research evidence into practice (eg, evidence-based medicine and clinical guidelines recommendations).45–47 The programme advocated and supported a specific implementation process using an ‘iterative systematic approach to improvement’ which included (QI) tools and methods (eg, model for improvement, plan–do–study–act (PDSA) cycles, process mapping), along with iterative evaluation, to support the implementation process.54–57 The approach also included the development of Action Effect Diagrams for each initiative to build programme theory for evaluation of impact.58–60
Study design
A longitudinal case study approach was taken to prospectively examine an initiative that aimed to spread a comprehensive medication review (CMR) intervention.61 62 For the purposes of this work, it will be referred to as the ‘CMR initiative’.
The case
This study reports on the spread of the CMR initiative between September 2014 and August 2018. The initiative was developed in response to evidence that with increasing polypharmacy there is a greater risk of medication-related harm and poorer patient outcomes.17 40 63 To optimise medication use and reduce harm, the National Institute for Health and Care Excellence (NICE) guidelines recommend conducting CMR for people with an indication for a review.63 A CMR is a medication review done systematically with adequate information about the patient and with the patient’s involvement, often using structured criteria for detecting potentially inappropriate prescribing. NICE recommends that ‘organisations should determine locally the most appropriate health professional to carry out a structured medication review, based on their knowledge and skills’.63 This often includes the prescribing physician, a pharmacist and/or another health professional who is part of a multidisciplinary team.63–65
The initiative began at site A, an acute hospital, and was led by a team with significant medicines optimisation expertise and experience in QI. To support a structured CMR, the initiative adapted evidence-based criteria from the Screening Tool of Older People’s Prescriptions (STOPP)65 and produced an updated tool ‘Screening Tool for Older People’s Inappropriate Treatments’.66 67 CMRs using the STOPP criteria were implemented for anyone aged 70 years or above, who presented acutely and were taking medicines regularly. Following results demonstrating improved patient safety and care at the initial site, the initiative gained interest from other sites across northwest London.67 68 From March 2015, four additional acute hospital sites (sites B–E) sought to implement this initiative, with varying levels of prior QI experience.
All sites reported an improvement in the number of structured medication reviews being conducted (demonstrated by Statistical Process Control rule breaks), and described a culture shift in how clinicians planned and discussed medication reviews as part of their comprehensive assessments.69 70 The evaluation of outcomes across sites will be published separately.
Data collection methods
Data were collected in two phases.
Phase 1 (understanding the intervention)
Observation: non-participant observation of the teams took place (24 hours) at facilitated workshops (about the intervention and its operationalisation) and routine meetings that discussed plans, progress and emergent learning. Observations were recorded in a field notebook.
Documentary analysis: 53 initiative documents were collected and analysed (meeting minutes, presentations, initiative review reports) in addition to QI tool outputs (action effect (programme theory) diagrams, PDSA cycles and a structured sustainability tool) to capture initiative components and activities.57 58 71
Semistructured interviews: key informant sampling was used to recruit interviewees from all sites.72 73 Participants were selected based on their knowledge, expertise and role within the initiative.74 Eight interviews were carried out face-to-face with one interviewer (LL) and elicited information on intervention components, progress and adaptations. An interview guide was used, and all interviews were recorded and professionally transcribed (interviewee details are found in online supplemental file 1).
Supplemental material
Phase 2 (triangulation of findings)
Facilitated workshop: a facilitated workshop (n=10) was conducted to triangulate interpretation of intervention components; assess perceptions of the importance of components and establish the proportion of effort invested in activities. Purposive sampling was used to invite individuals who had played a substantial role within the initiative across the five sites (online supplemental file 1). A discussion was conducted (facilitated by SB) to present the intervention components and remove or adapt any components based on participant views. An activity was then conducted to explore the perceived effort expended across each of the components where each participant was provided with 100 counter chips to distribute between each of the components (represented by printed headings and pots to place the counters). The focus group was audio recorded and professionally transcribed, and field notes were taken.
Data analysis
A qualitative database was developed using NVivo V.10 to conduct thematic analysis.75–77 Interview transcripts, documents and observational fieldnotes were imported into the database. Following familiarisation with each source and modifying (eg, correcting transcription errors) material as necessary, a preliminary coding structure was inductively developed, establishing thematic groupings to understand the spread of the intervention. The coding structure and themes were iteratively developed and refined as further data (ie, the workshop transcript and fieldnotes) were added.78 The data were eventually summarised to highlight overarching ‘spheres of operation’, intervention component functions and adaptations. The ratings from the counter chip ‘effort’ exercise were input into an Excel database and descriptive analysis performed. Findings were then used to examine possible HC/SP configurations of the CMR initiative based on three existing definitions.
Results
Insights from the improvement team members provided a rich picture of how the CMR initiative evolved over time within and across the five sites. Teams addressed many system issues that extended beyond the immediate conduct of the CMR that were required to support the successful operationalisation of the evidence base. Results are presented in five sections: (I) Intervention components; (II) Interdependence of components; (III) Initiative evolution and adaptation; (IV) Effort to operationalise the intervention; (V) Critical appraisal of the ‘HC’ and ‘SP’.
I. Intervention components
In our analysis, the evidence base (NICE recommendation to conduct a CMR with structured criteria for identifying inappropriate medications, here the STOPP criteria49) provided a focal point for understanding the work that was required to operationalise it into practice. Translating this evidence base into practice was the focus of the improvement teams’ work, and this remained consistent across all sites. Analysis revealed a total of 16 components which had essential functions in the operationalisation of the CMR initiative. The components were organised under four ‘spheres of operation’ that represent what needed to be in place in the system (eg, the necessary procedures, processes and behaviours) to support the intervention in practice:
Accessibility of evidence base: the need to interpret the evidence base and make the evidence easily available for clinicians to use in daily clinical practice within their specific context.
Processes of enactment: the clinical activities involved in enacting the evidence-based intervention in local practice, that is, ensuring the right patients are identified and receive the intervention, and that results from the intervention are acted appropriately on.
Dependent processes: the organisational processes and infrastructures that directly or indirectly support the clinical activities of the intervention.
Dependent sociocultural issues: the beliefs, common practices and/or behaviour that are required to support effective operationalisation of the intervention.
The team was required to take action within all spheres to ensure the successful operationalisation of the intervention. table 1 presents the four ‘spheres of operation’ with their respective intervention components. It highlights each component’s function, adaptations made and effort expended on each.
Spheres of operation and intervention components of the CMR initiative
II. Interdependence of components
The cumulative and interdependent roles of the components emerged as critical to successful operationalisation of the intervention. Although the 16 components are represented as distinct activities, the participants described their interactions. For example, portable aide-memoires (Accessibility of the evidence base) were distributed to junior staff to help them identify patients who would benefit from CMR (Process of enactment). Conducting a CMR was dependent on the quality of medical history available for individual patients (Process of enactment). This was dependent on the quality of the processes and practices in place for medicine reconciliation (Dependent processes), which in turn was influenced by the availability of trained staff to perform medicines reconciliation (Dependent processes) and the role expectations of these staff members (Dependent sociocultural issues).
Interdependencies such as these provided insight into how wider systems, processes and practices needed to be considered to support effective and routine application of the evidence base in practice. While some of these interdependencies were anticipated by staff, others emerged throughout the initiative (see section III).
III. Intervention evolution and adaptation
Spread sites developed a shared aim to ‘sustainably improve our delivery of consistent, high quality medicines optimisation to achieve better patient experience and outcomes in northwest London’ (Document_AED). However, participants acknowledged the need for adaptations across sites, to ‘Design your intervention so that it fits with your local practices and processes’ (I9_Pharmacist_Site B). While there was commonality in the components deployed across all sites, adaptations were observed including adaptations between sites, within sites and over time in response to local needs, emerging evidence and site learning (table 1, column 3).
Adaptations made between sites in response to local resources, needs and infrastructure
Each site made adaptations to the scope of the initiative. At site A, the initiative was implemented across the whole hospital, but other sites delivered the initiative on acute care of the elderly wards (sites B, C, E), and an acute assessment unit (site D). The need to adapt scope at sites B–E was attributable to resource availability. ‘(Site B) can’t spread further than the geriatric wards…(Site B) can’t spread because there isn’t the resource. So it comes down to the same thing for every project: we need staff and for the staff we need funding’ (I8_Clinical lead_Sites A and B). Sites decided to target the most vulnerable groups to maximise potential impact from the intervention. Decisions to limit scope caused adaptations to be made between sites including how patients were identified for CMR; which staff were involved with conducting CMR in each setting and which staff received training.
Site digital infrastructure also played a key role in adaptation required across the sites. For example, an initial CMR template was produced by site A to guide clinicians on how, when and why to carry out a medication review. Each site invested significant time in navigating local infrastructure and information governance processes to introduce the CMR templates in their settings. For sites C–E, this was further complicated by pilots and upgrades to new digital infrastructure.
Adaptations made within sites to respond to local variation
The process of delivering the initiative was dependent on resources and preferences of staff. For example, it was agreed by all sites that, in principle, the CMR should be conducted as part of a multidisciplinary team ward round. ‘We’ve basically decided that the only way you were going to get this done in a meaningful way was to have a multidisciplinary review and have everyone going round at the same time…that really helped to build some relationships that weren’t there before’ (I1_Project manager_Site A). However, adaptations were required on a daily and weekly basis within sites in response to staff resource and preferences. This was influenced by many factors including the availability of qualified pharmacists on individual sites, staff shortages, parental leave and competing care priorities. ‘The project was ongoing so we had huge variability in our pharmacy staff during the project period’ (Facilitated workshop_20170803).
Adaptations over time in response to emerging evidence and site learning
All sites made adaptations in response to changing evidence and emergent learning. A major impact for all sites was the update of the STOPP guidance in 2015. The new guidance reflected an updated systematic review of problematic prescriptions.65 This required an update of initiative materials including prompt cards and educational materials.
As well as adapting to new evidence, local learning was a driving force for further adaptation and improvement. For example, the teams had not anticipated the low levels of confidence that junior doctors had in conducting a CMR. They found that although junior doctors received training in how to prescribe medicines, no training was provided on how to deprescribe (stop) medications. This insight led site A to develop a new curriculum to increase competence in this area.65 ‘To improve doctor competency and confidence in deprescribing inappropriate medicines a new module on deprescribing…has been incorporated into junior doctor training’ (Document _Annual Report).
IV. Effort to operationalise the intervention
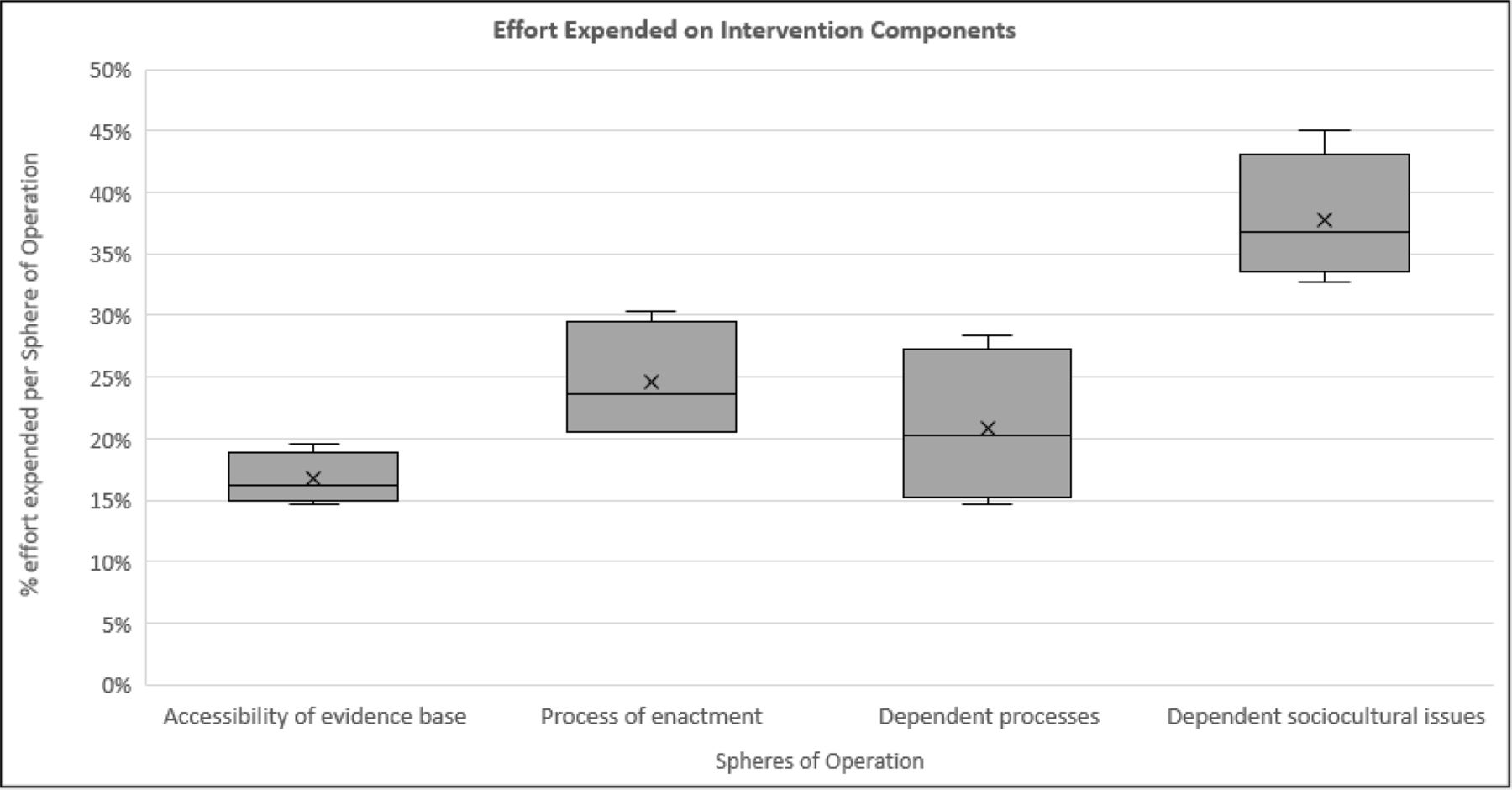
The effort expended to operationalise the intervention components varied across spheres of operation (figure 1 and table 1 (%)). Participants reported that most effort had been dedicated to components categorised within the sphere of ‘Dependent sociocultural issues’ (37.8%). Within this sphere, the specific components, Junior doctor and pharmacist empowerment (13.8%); Staff awareness and competencies (10.1%) were noted as requiring significant effort to ensure continued delivery of the initiative. Components Conducting a comprehensive medication review (CMR) (9.3%) and Documentation infrastructure (7.9%) were also judged to require a large amount of effort, due to the time required to conduct CMRs routinely in addition to normal practice. Participants reported that the least effort was invested in the sphere of ‘Accessibility of evidence base’ (16.7%). This was viewed as requiring less effort as components involved evidence consolidation tasks (eg, Summaries for clinicians (3.7%), Portable aide-memoires (6.1%)) which were completed at designated times (eg, beginning of the initiative and when the evidence was updated), while the other tasks were seen as ongoing activities.

Perception of effort expended on intervention components of the quality improvement initiative by site participants.
V. Critical appraisal of the ‘HC and ‘SP’
To identify and reflect on possible HC/SP configurations for the CMR initiative, three definitions were examined (table 2).4 19 44 In critically assessing the HC/SP construct, we found the different construct definitions challenging to interpret and apply to the CMR case study. Due to the ambiguity and lack of specificity of the given definitions, the intervention components were often unable to exclusively meet the requirements for either HC or SP. Therefore, results show contradictory configurations of the HC/SP for the initiative.
Applying hard core/soft periphery (HC/SP) definitions to the CMR case study
Denis et al’s19 definition of HC components as ‘fixed’ meant that none of the CMR intervention components were considered core as none were completely fixed: even the evidence base informing the intervention was updated during the course of the initiative. Craig et al’s44 definition also implies that the ‘active’ core components are not adapted, and the components that are adapted (periphery) are not important to outcomes. In our case study all components were adapted, and yet all were deemed necessary to achieving the desired outcomes.
Conversely, Greenhalgh et al’s4 definition fit more closely with our empirical findings, as it does not associate the HC or SP with adaptation and similarly recognised the importance of supporting structures and process components within intervention description. However, some ambiguity around this definition remains as it draws a distinction between the core ‘irreducible elements of the intervention’ and the peripheral ‘supporting systems and structures’, which makes the implicit assumption that systems and structures are not essential components of an intervention. Our study demonstrated that participants considered all components to be ‘irreducible elements’, including those within the organisational structure and processes, due to their interdependent nature. This made the differentiation between HC and SP ambiguous in this case.
Discussion
The ability to accurately describe interventions and understand how evidence can be translated into routine practice is critical to reproduce improvements in different settings.22 27 30 This study provides rich insight into the work conducted from the perspective of improvement teams to appraise and advance the description and conceptualisation of interventions in complex systems.
An insider’s view: interventions-in-systems
Analysing the improvement initiative from the perspective of the improvement teams revealed a rich understanding of ‘interventions-in-systems’, recognising that the CMR was not an isolated activity, but dependent on its interaction with established processes and practices. Team actions were not limited by any predefined notion of what the intervention ‘should’ entail, and instead they actively sought to ensure the system was operating in a way that supported the intervention. These findings resonate with previous research which suggests interventions can be seen as ‘events in systems’ with importance placed on understanding how the intervention interacts with and disrupts the system it is deployed in.51 Findings also demonstrate that evidence operationalisation is not a one-off or time-bounded activity that disrupts the system, but instead an ongoing effort to address and maintain system performance aligning to the idea of ‘intervening in systems’.54
Consistency of function, adaptation of form
The improvement teams described intervention components and functions that were common across sites. Due to their interdependency, all component functions were seen as critical, and from this perspective a shared view of how to operationalise the CMR evidence base in practice was held between the five sites. However, while all components were perceived as necessary, all were adapted.
This finding resonates with what has previously been defined as the ‘function and form’ of interventions: the ‘function’ represents a high-level statement of what an intervention is aiming to achieve (eg, increase competency), and the ‘form’ represents the specific form in which that intervention is delivered (eg, an educational workshop). Hawe et al 51 observe d that when working in complex systems, the ‘function’ is likely to be what can be standardised, whereas the ‘form’ will be likely to be adapted to meet the different needs of local systems. Our findings support this proposal: the component ‘functions’ were common across all sites, whereas the component ‘form’ always required adaptation.
Advancing the conceptualisation of interventions in complex systems
Based on our analysis, we conclude that the HC/SP construct is not well suited to conceptualising interventions in complex systems. We found the notion of core and periphery and the consideration of adaptation helpful but not conflation of the two. Previous HC/SP definitions tend to adopt a more reductionist view, focusing attention on the HC as the ‘fixed’, ‘essential’ or ‘active’ part of an intervention, and as such potentially trivialise the SP as ‘adaptable’, ‘supporting’, ‘inactive’ or ‘implementation activities’. This distinction risks minimising the attention paid to adaptable components as they are seen as non-active elements of the intervention. Our case and many others have shown that adaptations to interventions are not only common but often necessary for success.17 36 43 79–86 This suggests that the previous HC/SP perspectives have inappropriately conflated the concepts of effectiveness and adaptability by assuming if components can be adapted, they are not essential to the effectiveness of the intervention.44
These findings suggest the need to advance conceptualisation of interventions to more explicitly consider how an intervention is operationalised in complex systems. Drawing on insights from the improvement teams, we propose an updated intervention conceptualisation that builds on the HC/SP construct and proposes a more nuanced approach to intervention conceptualisation. The revised conceptualisation is summarised in box 1 and figure 2.
Advancing intervention conceptualisation in complex systems
Revised intervention conceptualisation: ‘interventions-in-systems’
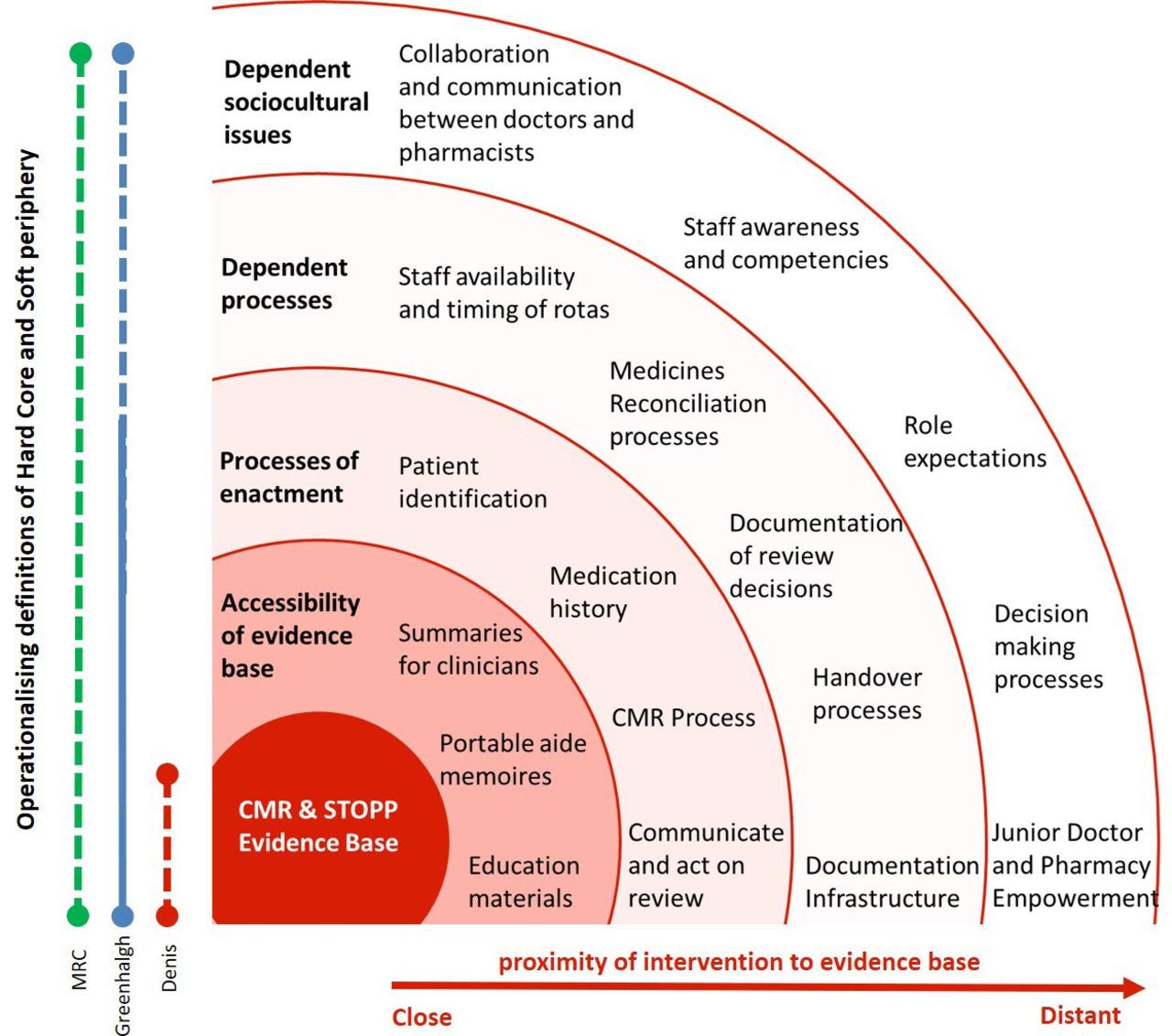
Proximity to the evidence base: the ‘core’ and ‘periphery’ of an intervention can be conceptualised in relation to the proximity of the intervention components to a focal point of the initiative (eg, evidence base). This can be represented as ‘spheres of operation’ close to the core (Accessibility of evidence base, Process of enactment) as well as those more peripheral (Dependent processes and Dependent sociocultural issues). All contribute to successful outcomes.
Component interdependence: the activities of the ‘core’ and the ‘periphery’ are interconnected, and understanding and articulating the interdependence of intervention components is critical for successful implementation. All components including those in the periphery are considered important to effective implementation and successful outcomes.
Component function: identifying the ‘function’ of intervention components provides clarity on what each component is intending to achieve. Each function should describe how the component supports the operationalisation of evidence in routine practice. This function should be irreducible and generalisable across diverse settings. Collectively the component functions represent the requirements to operationalise evidence into practice.
Component adaptation: assessing the degree and nature of adaptation is important in understanding how intervention components are effectively applied in local settings. Adaptation can take place between sites, within sites and over time in both the core and peripheral elements based on local resources, needs, constraints and infrastructure, as well as emerging evidence and site learning.
Effort: significant effort is required to operationalise and adapt intervention components. There is a need to acknowledge the often neglected and undervalued labour required to enact change in practice including solving local problems, adapting interventions and motivating staff to engage in new ways of working. This effort is crucial to the success of intervention spread, and only by being explicit about the nature and amount of this effort can we manage expectations for the planning, conduct and evaluation of change efforts.
{kind=link}
{kind=link}
CMR intervention components by ’spheres of operation’. Each sphere represents the proximity of each component to the evidence base. Y-axis: hard core and soft periphery configurations based on the Medical Research Council (MRC) definition (green line), Greenhalgh et al definition (blue line) and Denis et al definition (red line). A solid line represents intervention components meeting the definition of hard core. A dotted line represents intervention components that could be classified as hard core or soft periphery. No line represents intervention components meeting the definition for soft periphery. CMR, comprehensive medication review; STOPP, Screening Tool of Older People’s Prescriptions.
Box 1 presents the revised conceptualisation of ‘interventions-in-systems’ and describes intervention components in relation to their: proximity to the evidence base; component interdependence; component function; component adaptation and effort. This conceptualisation maintains the notion of ‘core’ and ‘periphery’ as defined by the proximity of the intervention components to the evidence base. For example, ‘Accessibility of evidence base’ is directly related to the CMR and STOPP criteria, communicating the evidence to increase practitioner understanding and application. Whereas ‘Dependent sociocultural issues’ (the most distal category) had an indirect link to the evidence base yet were required to effectively deliver the CMR. The revised conceptualisation replaces the simplistic notion of ‘hard’ or ‘soft’ by recognising the interdependence and potential adaptation of all components, and the importance of defining component functions as the irreducible and generalisable aspects of an intervention (which collectively should describe the requirements to operationalise the evidence base into practice). We also emphasise the need to understand the effort required to adapt and embed intervention components in each spread site.
Figure 2 presents this conceptualisation visually, picturing the evidence base as the core of the CMR intervention, surrounded by ‘spheres of operation’ and associated intervention components based on their proximity to the evidence base. Figure 2 also visually represents the challenge of applying the existing HC/SP definitions due to the ambiguity of each definition in categorising the ‘core’ or ‘peripheral’ components as either ‘hard’ or ‘soft’ (represented by solid and dotted lines). The inconsistency between the three definitions is represented by separate red, green and blue lines.
Strengths, limitations and future work
This study makes an empirical contribution by taking a systems view and drawing on ‘insider’ knowledge to provide a richer account of how interventions are spread across multiple sites. The findings from this work are complementary to building programme theory for evaluation of impact as they enable more detail description of intervention components and mechanisms of action that can support evaluation design.
However, this study also has several limitations. A known weakness of prospective case study design is limited external validity. This means we cannot ascertain whether our findings are applicable and generalisable to other contexts and initiatives.62 87 For example, components might not fit within our ‘sphere’ classification, or different sites may have different views on which components are irreducible. We also recognise the sites we were working with had significant clinical expertise, QI experience and support, and dedicated time and resource for the initiative, which will have influenced the study findings. This is, however, inherent to the iterative process of theory building; future studies are needed to test and refine proposed theoretical contributions.
The impact of ‘groupthink’ may have also been a limitation to our findings.88 Although there was strong consensus on the intervention components and functions proposed, groupthink may have led to fewer dissentions or identification of alternative options. Through the triangulation of multiple data sources, we aimed to mitigate this limitation.
Future research is needed to assess how intervention adaptations, based on component function, impact intervention effectiveness. While intervention fidelity has been associated with positive outcomes,89 in line with others, our study suggests this might not be feasible or desirable in practice.51 The components’ functions described by this study provide a strong foundation to design and conduct more analytically rigorous studies to explore the attribution of adaptations to the overall success of the initiative. Indeed, such work would not be possible without this prior work to prepare a detailed understanding of the intervention components and their interactions.
Implications for research and practice
The approach taken in this research can provide guidance to support practitioners and researchers to study and describe interventions, to support spread and reproducibility of improvement initiatives. We propose a generic template for conceptualising interventions based on the methodology used in this study (online supplemental file 2).
Supplemental material
From a practical perspective, this template can support implementation teams to list intervention components, describe the component functions and the rationale for adaptation. This will help new sites avoid narrow artificially bounded intervention descriptions.90 91 From a research perspective, this will provide an opportunity to systematically build knowledge, test theories, and increase the scale, sophistication, rigour of evaluation approaches as interventions are spread to a greater number of sites.
Conclusion
The study makes theoretical and practical contributions towards the comprehensive conceptualisation of healthcare interventions. We demonstrate the value of co-producing knowledge of interventions between improvement teams and researchers through prospective study. This ‘insider’ knowledge revealed that interventions cannot be viewed as isolated activities, and their effective operation can only be achieved through understanding their interaction with established processes and practices. We conclude that to understand and describe interventions, we need to conceptualise them as ‘interventions-in-systems’. Adopting this view identifies the range of actions required to ensure interventions are ‘fit for purpose’ and that the surrounding systems are capable of supporting them.
In applying HC/SP constructs in the context of the multisite CMR initiative, we encountered challenges in the binary conceptualisation of intervention components as either HC or SP. Therefore, we propose a more nuanced approach to intervention conceptualisation where components are described in respect to their: proximity to the evidence base (whether component parts are closer or further away from the core evidence base); component interdependence (how the components interact with and influence each other); component function (the purpose of each component which should be generalisable across sites); component adaptation (the degree and nature of adaptation in local settings) and effort (the amount of effort required to enact change in practice). Collectively, such a description should represent the work needed to operationalise evidence into practice in diverse settings, facilitating knowledge-sharing between sites, and reproducibility of successful improvement initiatives. Further work is needed to test and refine our proposed theoretical contributions to assess and strengthen their practical relevance.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplemental information.
Ethics statements
Patient consent for publication
Ethics approval
This study has been approved by the NHS Health Research Authority (IRAS 188851). Although the potential for distress or risk for participants in this study was low, ethical considerations for consent, confidentiality and data protection were made. Participants were given information sheets about the study and consent forms prior to interviews and the focus group. All participants provided written consent prior to participation. Participants were also given the option to withdraw from the study at any time prior to write up. To ensure confidentiality, names of participants were not audio recorded during the interviews and each participant was assigned a unique identifier. All recorded and transcribed information as well as names and contact details was kept in separate, password-protected files stored on secure servers. Access was only permitted to approved researchers. All data remained fully confidential and findings are reported in an aggregated manner without reference to individuals’ names. To maximise confidentiality of individual participants, generic job titles instead of specific grades or specialty titles have been used.
Acknowledgments
The authors would like to thank the participants of this research for agreeing to be involved and allowing access to their workplaces and daily activities. Their participation made these findings possible, and their time, support and feedback were greatly appreciated.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @lauralennox3, @julie4clahrc
LL and JER contributed equally.
Contributors LL and JER contributed equally to the paper. JER and LL conceived of the study. LL and JER developed the research protocol with contributions from NS and SB. VM and EW led the CMR initiative. LL undertook the interviews. JER, LL and SB conducted the observations. SB conducted the focus group. NS performed the initial analysis of the data. LL and JER refined and developed the emerging themes and findings and conducted further analysis. SS, VM, EW and SB reviewed and commented on themes and findings. LL drafted the first version of the paper and JER made contributions to interpret results and develop the conceptual findings of the paper. All authors contributed to the development of the manuscript content. All authors read and approved the final manuscript.
Funding This research was funded by the National Institute for Health Research (NIHR) Collaboration for Leadership in Applied Health Research and Care Northwest London (CLAHRC NWL), now recommissioned as NIHR Applied Research Collaboration NWL (ARC NWL). The research team also acknowledges the support of the NIHR Clinical Research Network (CRN). JR was also funded by a Health Foundation Improvement Science Fellowship.
Disclaimer The views expressed in this publication are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.