Article Text

Statistics from Altmetric.com
The pace of technological advancements in the intensive care unit (ICU) challenges clinicians’ ability to manage ethical and decision-making challenges near the end of life. Modern medicine has advanced to the point where we can support multiple organ systems simultaneously and sustain life when the benefits of treatments to overall survival and quality of life are not always clear. Physiological and technological limits no longer always tell us when to stop, and clinicians and families are now forced to take over the role that was once played by nature to make decisions as to whether and when life-sustaining therapies should be withdrawn or withheld.
Unfortunately, we often do not do a very good job of making these tough decisions even when patients can participate in the discussion. To add to that challenge, patients often lack decision-making capacity during their ICU stay. Clinicians and families struggle to balance the inherently imperfect practice of substituted judgement with their own views on the best interests of the patient. Advance care planning can facilitate this process, but even with the best advance care planning, it is often a complex and uncertain process.
Recent evidence indicates that we are not negotiating this complex process well.1 2 Life-sustaining therapies are increasingly provided at the end of life in a way that confers no survival benefit and can cause harm. Older Americans with advanced dementia have experienced a doubling in the use of mechanical ventilation and a rise in ICU admission from 17% to 38% of those hospitalised in the last 30 days of life without substantial survival benefit.1 2 A recent cluster-randomised trial suggests that systematically increasing ICU admissions for older adults confers no mortality benefit,3 and other studies have shown a trend towards harm.4 5 Hospitals with higher frequency of ICU use have higher costs and greater use of invasive procedures without improvement in mortality.5 Overly aggressive, non-beneficial treatments are associated with reduced quality of life near death and lower perceptions of quality of care.6–10 Symptoms of post-traumatic stress disorder (PTSD) and depression are more likely among caregivers of patients who experience overly aggressive treatments.10–14 The ethical challenges inherent to considering the burdens and benefits of life-sustaining therapies near the end-of-life care, especially in the ICU, can be highly contentious and challenging.15 16
In the high-stakes environments of the ICU, clinician moral distress, originally defined by Jameton17 as the inability to act according to an individual’s ethical beliefs due to structural or hierarchical constraints, can be particularly prevalent.18 While nurses have recognised the importance of ethical climate and moral distress for decades,19 awareness of physician moral distress is a newer area of enquiry,20 21 perhaps reflecting the growing tensions that have arisen as a result of shifts in societal expectations surrounding autonomy and declines in physician power.22 While moral distress can occur in all areas of healthcare, perceived futile care is a particularly difficult and common ethical challenge in the ICU that frequently leads to clinician moral distress.20 23
Moral distress is an ethical root cause of clinician burnout,24 an urgent problem that affects more than half of US physicians.25 Clinician burnout is linked to poor clinician well-being, job dissatisfaction and job turnover.26–28 Burnout among medical students contributes to unprofessional behaviour and declines in empathy.29–31 Clinician burnout has negative effects on patient care, including reduced patient satisfaction, quality of care, patient rapport and patient safety, with higher rates of medical errors.32–34
Interventions to mitigate clinician moral distress and burnout tend to focus on the individual clinicians.35–38 Cultivating mindfulness and resilience is important and is a necessary step to alleviate moral distress, but must be integrated with interventions that target broader cultural norms that influence clinician behaviour and integrity. Although some have described the need to consider organisational and systems factors, little is known about the precise systemic inflection points and levers that influence moral distress and burnout.39 In particular, ethical climate, defined as ‘individual perceptions of the organization that influences attitudes and behavior and serves as a reference for employee behavior’,40 should be recognised as an important contributor that either alleviates or exacerbates moral distress.
In BMJ Quality & Safety, Van den Bulcke and colleagues41 report the development and validation of the Ethical Decision-Making Climate Questionnaire (EDMCQ). This is an important step in allowing us to understand and subsequently design and evaluate interventions that modify an ICU’s ethical climate to alleviate clinician moral distress and burnout and improve the patients' and families’ experience. The authors developed this 35-question self-assessment instrument through a modified Delphi method that created a theoretical framework for ethical decision-making. The instrument was subsequently validated in 68 ICUs in 13 European countries and the USA. The ethical decision-making domains included within the EDMCQ are interdisciplinary collaboration and communication, leadership by physicians, and ethical climate. Although moral distress can manifest in many different ways, the EDMCQ allows us to specifically measure aspects of ethical climate as they relate to moral distress due to decision-making surrounding intensity of ICU care.
A clinician’s decisions do not occur in a vacuum, but are instead embedded in a cultural milieu influenced by national policy, financial incentives, resource pressures, patient and family factors, and institutional leadership. Policy changes and systemic interventions can have unintended consequences that further disrupt this interconnected ecosystem.42 In a recent qualitative study, one of us (ED) found that an institution’s ethical priority influenced the way physicians conceptualised autonomy and beneficence, which consequently influenced communication practices surrounding resuscitation decision-making near the end of life.43 The study also revealed the importance of systemic factors such as institutional cultural norms that contributed to inappropriately aggressive care at the end of life in the USA.44 This study and others highlight the importance of understanding and intervening on these institutional and ethical norms to mitigate overly aggressive care.45 46 We have previously hypothesised that interventions may be more effective if they target the attitudes, beliefs and culture that underlie communication practices rather than only the practices themselves.44
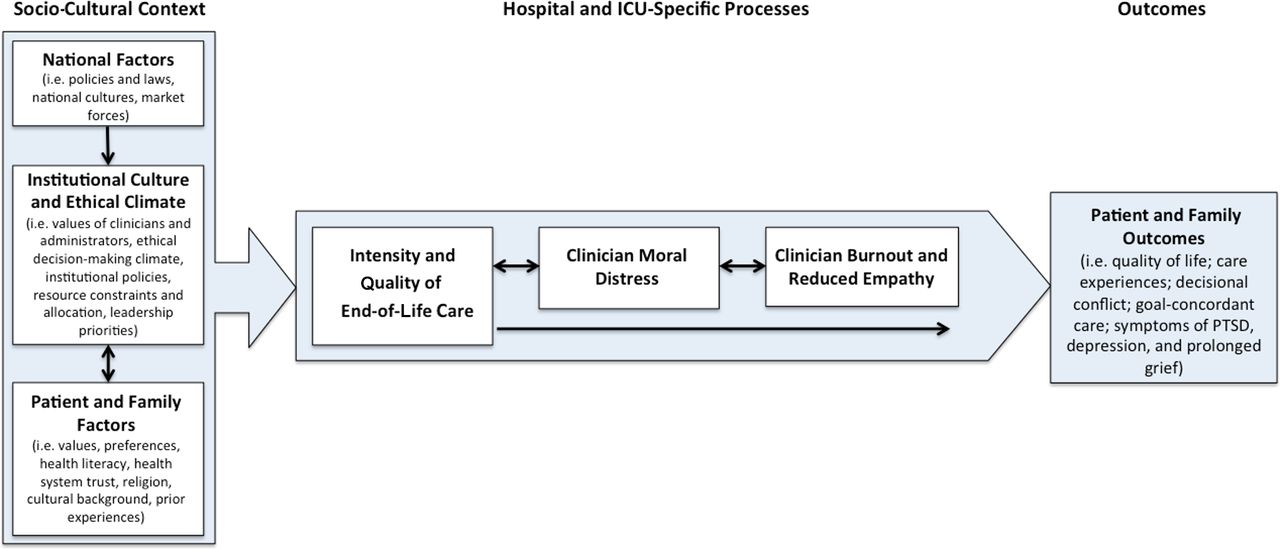
We propose a conceptual framework (figure 1) highlighting the importance of institutional culture and, in particular, of institutional ethical climate, which influences intensity of end-of-life care in the ICU and hospital setting, and subsequently contributes to clinician moral distress and burnout. We hypothesise that this causal pathway from ethical climate, to intensity of care, and subsequent moral distress and burnout result in substantive effects on patient and family outcomes including quality of life, experience of care, and presence of symptoms of PTSD, depression and prolonged bereavement. As such, the importance of the EDMCQ is its ability to measure, guide and evaluate interventions on the ethical decision-making climate, providing the potential to improve patient, family and clinician outcomes.
{kind=link}
Conceptual model describing the relationship between ethical climate, clinician moral distress and burnout, and patient and family outcomes. The Ethical Decision-Making Climate Questionnaire focuses on institutional culture and ethical climate and its influence on institutional norms, which influence the intensity of end-of-life care. ICU, intensive care unit; PTSD, post-traumatic stress disorder.
Multiple qualitative and quantitative studies in the nursing literature have found that a positive ethical climate facilitated less moral distress among nurses.47–49 Given that in the ICU clinical decision-making is at the nexus of ethical challenges surrounding life-sustaining therapies near the end of life and a crucial moment for shifts in care trajectory, ethical decision-making climate is a key aspect of ICU ethical climate. The EDMCQ homes in on this critical facet of ethical climate that specifically links ethical climate with ICU treatment decisions at the end of life.
The EDMCQ scale is a valuable addition and update to existing ethical climate scales, the most prominent being the Olsen Hospital Ethical Climate Survey (HECS), which was designed and validated in the nursing literature.40 The HECS is a measure of ethical climate among nurses and focuses on factors related to nurses’ relationships with actors within the hospital system, such as nurse peers, patients, managers, hospital administrators, and physicians. The EDMCQ focuses on physicians and nurses, as well as unit physician leadership, which all have profound effects on both ethical climate and ethical decision-making climate.
Given that physicians are often in positions of power in the hospital, involvement of and measurements that include physicians are important to an assessment of ethical culture. Studies using the HECS in physicians and nurses have shown that physicians generally rated ethical climate more positively than nurses,50 highlighting the power differential and affirming the importance of the EDMCQ’s focus on interprofessional (particularly nurse–physician) trust, collaboration, and communication. In particular, the EDMCQ’s emphasis on hearing the voices of all members of the team highlights the importance of the moral agency to speak up as being an important part of fostering positive ethical climates and alleviate moral distress.51 52 Furthermore, the EDMCQ’s emphasis on interdisciplinary collaboration and communication is important as unit dysfunction and intrateam discordance exacerbate moral distress among members of the ICU team.18
The paper by Van den Bulcke and colleagues has some important strengths and weaknesses. In terms of strengths, this is a large and well-conducted study that included 3610 nurses and 1137 physicians working in 68 adult ICUs across Europe and the USA. The authors used a careful modified Delphi approach to develop a survey with strong face validity and they used rigorous and state-of-the-art exploratory and confirmatory factor analyses to determine the structure of the ethical decision-making climate concept. This report also has some important weaknesses. First, the 68 ICUs represent a convenience sample of ICUs that were willing to participate, although it is difficult to know how this might affect the findings. Second, the reports of ICU clinicians on their own ethical decision-making climate will undoubtedly be influenced by some degree of reporting bias, as well as by the fact that ICU clinicians may have limitations in their ability to observe the ethical norms in which they practise. Given these strengths and weaknesses, the EDMCQ is an important new measurement tool that should undergo additional validation as well as be compared with other methods to understand and assess the ethical decision-making climates in our ICUs.
We believe there has been insufficient recognition of moral distress as a key contributor to clinician burnout and poor well-being. Clinician burnout is a topic that has garnered significant interest and attention over the past several years.33 53 54 In light of this crisis of clinician burnout, there is an urgent need to look to systemic and cultural root causes of burnout. One of the barriers to focusing on institutional culture and systems change is that it is difficult to measure culture. The EDMCQ helps advance the field by providing ways to measure ethical decision-making climate, thus facilitating future descriptive and intervention studies focusing on institutional and ethical culture to improve patient and family outcomes. Another benefit of the EDMCQ and other instruments that focus on the more humanistic aspects of medicine55 is that it draws attention to an institutional prioritisation of ethics and ethical climate among clinicians and administrators.56 The EDMCQ is an important step in improving the ethical decision-making climate of ICUs around intensity of end-of-life care and understanding its subsequent impact on the patient and family experience.
References
Footnotes
Contributor ED contributed to the conception of the paper. ED and JRC critically read and modified subsequent drafts and approved the final version.
Funding Research reported in this publication was supported by the National Center for Advancing Translational Sciences of the NIH under Award Number KL2TR001870. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Commissioned; internally peer reviewed.