Article Text

Abstract
Background This study aimed to involve patients with chronic conditions in generating ideas for improving their care.
Methods We performed a citizen science study. Participants were adult patients with chronic conditions recruited in Community of Patients for Research ‘ComPaRe,’ a French e-cohort of patients with chronic conditions. Participants generated ideas to improve their care in answer to the open-ended question, ‘If you had a magic wand, what would you change in your healthcare?’ Three researchers and two patients independently extracted ideas from open-ended answers by using thematic analysis. Ideas were grouped into areas for improvement at the consultation, hospital/clinic and health system levels. Findings were validated and enriched by a second sample of participants recruited in ComPaRe.
Results Between May 2017 and April 2018, a total of 1636 patients provided 3613 ideas to improve consultations (1701 ideas related to 58 areas for improvement), hospitals/clinics (928 ideas related to 41 areas for improvement) and the health system (984 ideas related to 48 areas for improvement). At the consultation level, most ideas were related to improving physician–patient discussions, informing patients about their own care, and adapting treatment to patient preferences and context. At the hospital/clinic level, most ideas aimed at improving the coordination and collaboration in care. At the health system level, most ideas were related to decreasing the administrative burden imposed on patients, improving access to care and reducing the costs of care.
Conclusion Patients have many ideas to improve their care, from the content of consultations to the organisation of hospitals. Our study provides the proof of concept for a method to leverage patients’ practical knowledge of the care system to improve it.
- chronic disease
- multimorbidity
- quality of healthcare
- citizen science
- patient participation
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Chronic disease is a global epidemic.1 In western countries, 40%–60% of adults have a chronic condition; 50% of these adults have multiple conditions and are considered multimorbid.2 3 This epidemic of chronic conditions challenges disease-centric care models in both European and American settings.4 Despite recent improvements, the care for patients with chronic conditions, in France and in other western countries, remains fragmented and uncoordinated, with a risk of polypharmacy and harmful interactions.5 6 This situation generates an important burden of treatment for patients that can affect their lives as much—or more—than the diseases themselves.7 8 In addition, in France, the care for patients with chronic conditions is affected by the decreasing medical coverage of large parts of the French territory because of a cost containment-driven policy to limit the number of professionals trained in medical schools and the progressive closure of local care structures for the benefit of larger urban medical centres.9 As a result, health professionals are asked to do more in less time and patients are hurried along in their consultations.10–12 Worse, initiatives to improve healthcare may have paradoxically contributed to the emergence of myriad norms, standardised protocols and pay-for-performance regulations, which hinder the importance of human relationships in care and contribute to a feeling of cumulative bureaucracy.13–15
Transforming healthcare is difficult because all parts of the system are intricate and influenced by political, economic and cultural factors and are constrained by value conflicts and resistance to change.16 17 In 2013, an international movement called the ‘Patient Revolution’ was formed to enlist patients, who live and experience the healthcare system every day, to help in designing care services better suited to them.18 The Patient Revolution mirrors initiatives launched in other fields that rely on citizen science methods and the collective intelligence of large groups of people to tackle complex problems. For example, the project Collective Intelligence for Public Transport in European Cities gathered ideas provided by 500 citizens to invent cleaner and better transport in cities19 and the Climate CoLab gathered propositions to tackle climate change from more than 90 000 people all over the world, over 7 years.20
In care improvement, despite multiple studies on patient-reported experiences, expectations and satisfaction in care,21–27 only a few studies have involved patients in identifying which components of the care system needed to be improved and how, and these studies often addressed specific issues, in given conditions or contexts.28 29 In the present study, we aimed to engage patients with chronic conditions, on a large scale, to identify which components of their care require improvement and to generate ideas to do so.
Methods
We performed a citizen science study with two steps. In the first step, patients with chronic conditions provided ideas on aspects of their care they wanted changed by using an online questionnaire with a broad open-ended question. Then, in a second step, another sample of participants reflected on and enriched the ideas identified.
Setting and participants
This study was nested within the Community of Patients for Research (ComPaRe), an ongoing citizen science project based on an e-cohort of patients with chronic conditions (www.compare.aphp.fr). Participants are adults (>18 years old) who report having at least one chronic condition (defined as a condition requiring healthcare for at least 6 months). ComPaRe involves mostly patients in France, although some participants may be from French-speaking countries (Belgium, Switzerland, and so on). Patients join the project to donate time to accelerate research on their conditions. They can do this by answering regular patient-reported outcomes and patient-reported experience instruments, suggesting ideas for new research or participating in the set-up or analysis of research projects. The recruitment started in January 2017 and is still ongoing, with about 18 000 patients included in November 2018. All participants provide electronic consent before participating in the e-cohort.
First step: the ‘magic wand’ question
In a first step, we analysed, in January 2018, data from a specific online questionnaire inviting patients to suggest ideas to improve their healthcare. The questionnaire was sent to all participants enrolled in ComPaRe (ie, adults with at least one chronic condition) starting from 9 May 2017. A single open-ended question was used to capture patients’ ideas to improve their care: ‘If you had a magic wand, what would you change in your healthcare?’ This open-ended question was inspired by (1) the ‘Miracle’ question used in solution-focused therapy to encourage participants to focus on possibilities rather than problems,29 and (2) a previous work aimed at identifying the propositions of patients with HIV to reduce their burden of treatment in sub-Saharan Africa.30 The magic wand question was pilot-tested by six patients from ComPaRe to ensure its clarity. Because testing took place before the development of the questionnaire, answers during the pilot phase were not merged with research data.
Open-ended answers were analysed by using thematic analysis with multiple rounds of analysis. In a first step, two investigators (VTT and CR) read the first 180 responses and independently identified ‘ideas’: literal sentences used by participants to describe their ideas to improve healthcare. Coding was limited to explicit statements of potential modifications in healthcare. For example, changes related to patients’ conditions or symptoms (eg, ‘If I had a magic wand, I would like to cough less’) or wishes for more research (eg, ‘I would like more research on my condition so that new effective treatments could be developed’) were dropped from the analysis. Patients’ statements of barriers and burdens in healthcare were extrapolated into wishes for improved care (‘There are too many visits’ was coded as ‘I wish there were fewer visits’). During regular meetings, the two investigators reached consensus on the ideas identified and grouped them into ‘areas for improvement’ according to the context, people and processes involved to implement these ideas. In a second step, this initial set of areas for improvement was used to classify the remaining responses. Each participant’s response was read by the two investigators, who independently assigned data segments to each area for improvement. During frequent meetings, the investigators compared their analyses and reached consensus on coding. This second phase involved more than simply sorting data segments: whenever new ideas emerged, researchers discussed these ideas and refined and enriched the list of areas for improvement.
Second step: enrichment of findings by patients
In April 2018, in a second step, we asked all patients who had answered the ‘magic wand’ question to reflect on and enrich the list of areas for improvement identified in the first step. We invited both people who had participated in the first step (n=1227) and people who had not because they enrolled in ComPaRe after January 2018 (n=741). We invited these participants to answer a second web questionnaire presenting all areas for improvement identified so that they could (1) assess whether they agreed with the list and (2) suggest new ideas that could have come up when reviewing the list. Indeed, reflecting on others’ inputs may enhance creativity and improve the quality of answers.31 32 To ensure that all three levels (consultation, hospital/clinic and health system) would receive similar attention by participants, these levels were presented in a random order to participants.
Open-ended data collected during this second step were analysed by two investigators (VTT and CR) using the same methodology as during the first step. Investigators extracted all novel patients’ ideas to improve their care and during meetings decided how these ideas could be classified under existing areas for improvement or could define new areas for improvement.
Then, another investigator (PR) and two patients (AC and CP) triangulated all findings from both the first and second steps of the study. During recorded meetings with the main investigator (VTT), they went back to the raw data and independently recoded participants’ answers (the whole corpus was recoded by PR and 10% of the corpus was recoded by the two patients) to challenge both the list of areas for improvement and how ideas had been classified. Finally, all investigators reached consensus on the classification of all patients’ ideas in areas of improvement.
Assessment of the point of data saturation
The objective of our study was to identify and list ideas for improvement in the care of patients with chronic conditions, from patients’ perspective. To ascertain that we achieved an exhaustive description of these ideas, we assessed whether data saturation had been reached. Data saturation represents the point in data collection and analysis when new information produces little or no change to the codebook, the codebook representing the collection of codes that link expressions found in text to all abstract constructs identified by the researchers.33 To determine the point of data saturation, we used a mathematical model to predict the potential number of new ideas that could be identified by adding new participants in the study.34 This model involved (1) drawing the ‘observed’ theme accumulation curve (eg, number of different areas for improvement identified during the course of the study); (2) predicting the theoretical number of areas for improvement that could be found with the inclusion of more patients; and (3) estimating the local slope of the expected theme accumulation curve (ie, the number of patients to be included to identify a new theme). Thus, the model did not inform on the nature (‘quality’) of themes identified but rather on the probability to find new themes by recruiting new participants. We examined the number of additional areas of improvement that could have been found by including more participants globally and in different subgroups defined by sex, age (≤50 and>50 years old), multimorbidity and educational level (college vs lower education). Analyses involved use of R V.3.3 (http://www.R-project.org, the R Foundation for Statistical Computing, Vienna, Austria).
Patient and public involvement
Two patients (CP, AC) who expressed interest in contributing ‘more’ than just answering questionnaires independently recoded 10% of all answers and contributed to the elaboration of the list of areas for improvement resulting from participants’ answers. They were also invited to be authors of the manuscript and critically revised it before submission.
Results
In the first step of the study, 1227 participants provided ideas to improve their care (2195 patients had been invited to answer the ‘magic wand’ question; response rate: 56%). In the second step, 752 participants, of whom 409 (54%) had not previously proposed ideas, reflected on the findings from the first step and suggested at least one new idea to improve their care (1968 patients were invited in the second step; response rate: 38%). As a result, 1636 patients (1210 (74%) female) proposed ideas to improve their care (online supplementary appendix 1). The mean age was 49 years (SD=14.4). Participants living in France (n=1600, 98%) were geographically dispersed among large cities, smaller cities and rural areas (online supplementary appendix 2). About 50% of our participants had multimorbidity (mean number of conditions 2.4 (SD=2.3)). Patients’ conditions included diabetes (n=146), asthma (n=105), rheumatological conditions (n=488), neurological disorders (n=331) and cancer (n=133). Patients’ characteristics are detailed in table 1.
Supplemental material
Characteristics of participants (n=1636)
During the first step of the study, we gathered 2941 patients’ ideas (51 140 words), grouped into 138 areas for improvement. In the second step, patients’ feedback on ideas previously discovered resulted in the identification of 672 new ideas (27 729 words) and nine additional areas for improvement. Therefore, patients proposed a total of 3613 ideas during the study. These ideas covered 147 areas for improvement: 58 (39.5 %), 41 (27.8 %) and 48 (32.6 %) at consultation, hospital/clinic and health system levels, respectively (online supplementary appendices 3, 4 and 5).
According to the mathematical model to predict data saturation, more than 99% of the potential areas for improvement were identified. Thus, our study represents a comprehensive mapping of the aspects of consultations, hospitals/clinics and the health system that require change, according to patients (online supplementary appendix 6).
Patients’ ideas to change consultations
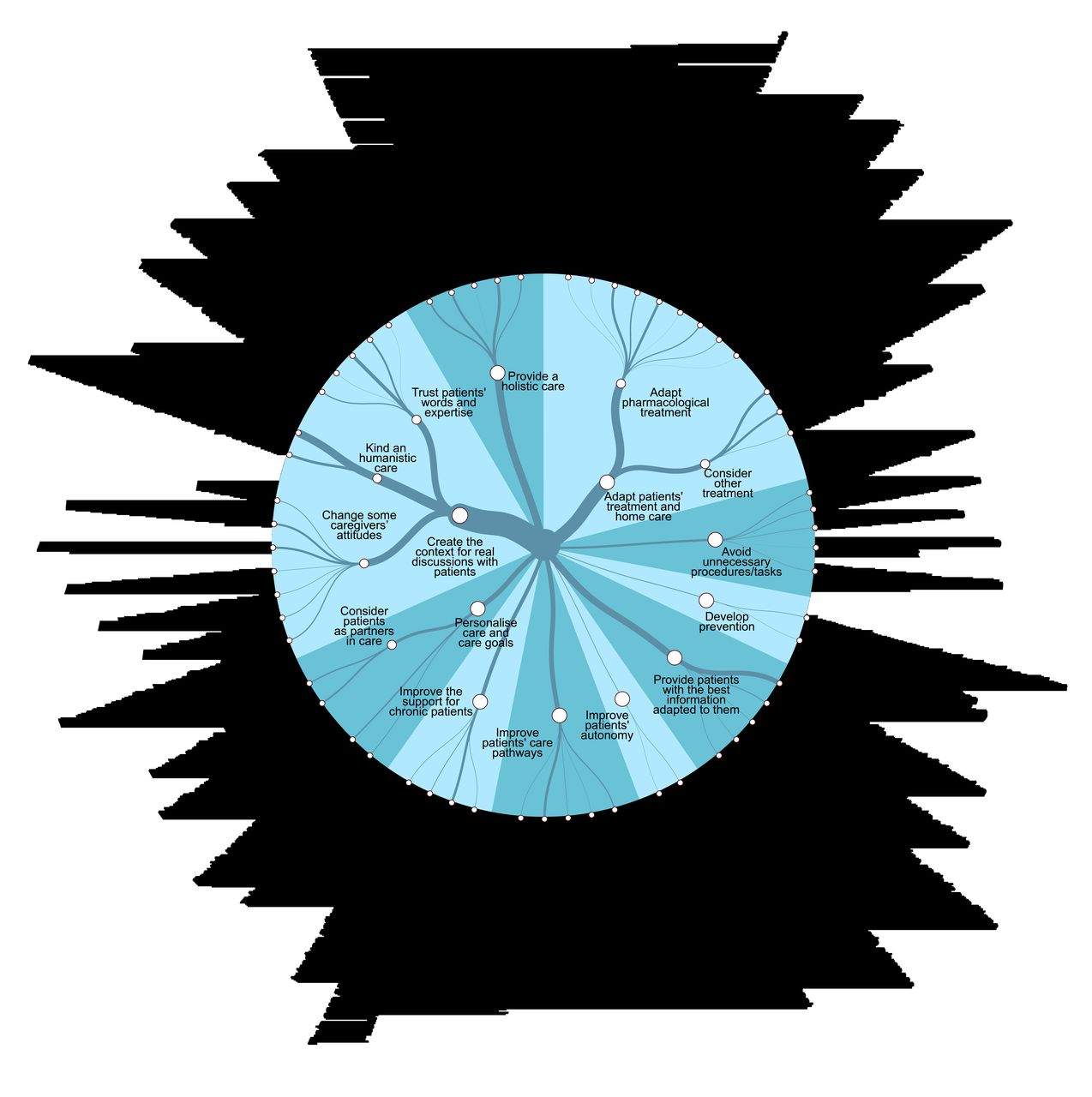
A total of 838 participants proposed at least one idea to change consultations, for a total of 1701 ideas. Examples of patients’ ideas to change consultations are in table 2, figure 1 and online supplementary appendix 3. We gathered fewer practical ideas to change care at the consultation level than the hospital/clinic or health system level. Rather, patients called for changing entrenched medical paradigms, behaviours and cultures. For example, a large number of patients called for creating the right context for discussions with their caregivers.
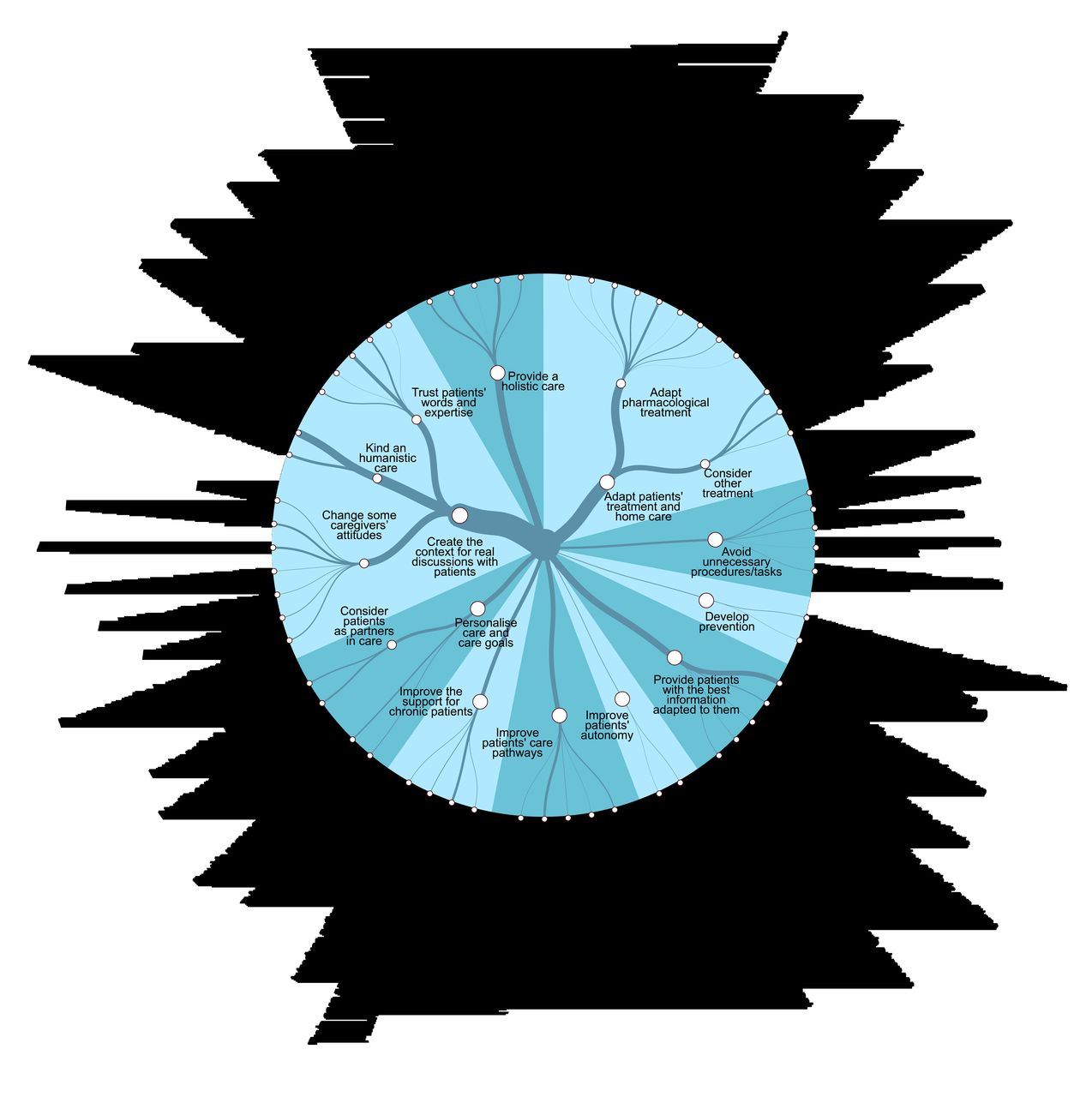
Areas for improvement at the consultation level. Line thickness represents the number of participants who elicited the idea.
Examples of patients’ ideas to change consultations (1701 ideas)*
If I had a magic wand, I would like to be listened to and understood. Do not question my observations and what I may have experienced before. Physicians should consider me as a partner. We should reflect together about the most appropriate treatment and management. They should help me be sincere by avoiding judging me. They should accept that I can make decisions by myself. (Female with endometriosis)
Ways to achieve this goal involved moving from standardised ‘mechanical’ and organ-centred care to personalised (n=121) and holistic care (n=187), and from paternalistic care to shared decisions to set common care goals (n=41) and major care decisions (n=32).
It is not acceptable to endure life-changing decisions without having at least a slight control on some aspects. Treating a disease is good, but if it means that patients will have no control over their lives, it’s not. Some decisions used to cure a patient can destroy him if he’s not the person who made it. Doctors should enlighten the patient but not decide for him. (Female with breast cancer)
Patients’ ideas to change hospitals/clinics
A total of 506 participants proposed at least one idea to change hospitals/clinics, for a total of 928 ideas. Examples of patients’ ideas to change hospitals/clinics are in table 3, figure 2 and online supplementary appendix 4. Examples of areas for improvement identified were to develop tools and processes to smooth the journey of patients with chronic conditions within the care system (n=368) and to improve the coordination and collaboration between the different actors involved (n=300). For example, patients suggested simplifying patients’ burden for managing appointments (n=135).

Areas for improvement at the hospital/clinic level. Line thickness represents the number of participants who elicited the idea.
Examples of patients’ ideas to change hospitals/clinics (928 ideas)*
Systematically schedule the next appointment at the end of the consultation. Do not wait for the patient to make the appointment himself from his home. (Female with diabetes)
Another idea to improve care coordination was to define, for each patient, an identifiable and accessible member of the care team they could rely on as their entry point in the care system (n=36).
I would create some sort of ‘care conductor’ who would assess the patient's needs and guide him [in the system] as well as possible. This would alleviate a lot of hardships to a patient already frail due to his disease. (Female with multiple sclerosis)
Examples of patients’ ideas to change the health system (984 ideas)*
Patients’ ideas to change the health system
A total of 604 participants proposed at least one idea to change the health system, for a total of 984 ideas. Examples of patients’ ideas to change the health system are shown in table 4, figure 3 and online supplementary appendix 5. According to patients, the main areas of health systems that should be transformed were to decrease the administrative burden imposed on patients with chronic conditions (n=179), improve access to care (n=155) and reduce the costs of care (n=166).

{kind=link}
{kind=link}
{kind=link}
Areas for improvement at the health system level. Line thickness represents the number of participants who elicited the idea.
Create a one-stop-shop for administrative tasks. These places would propose and explain patients how to obtain ALL possible state help for which they would be eligible: CAF [family allowance], help for housing or to adapt the patient’s home (adapt kitchens or bathrooms etc.), recognition of disability etc. It would allow patients to avoid going to multiple places, filling in multiple files and missing help that they ignore. (Female with rheumatoid arthritis)
In line with their demands to change caregivers’ attitudes, patients proposed ideas to transform caregivers’ training (n=128). As an example, a patient suggested that all people interacting with patients should be ‘put in patients’ shoes’ to improve their interpersonal skills.
Train professionals to talk correctly to patients and to show empathy. (…) Teach them to listen to patients without systematically questioning their words. Personnel from MDPH [Departmental Structures for people with disability], CAF [Structures for family allowances] and the National Health Insurance system should live one week or more of the life of a sick, diminished or disabled person. This should be a mandatory internship ‘Live my Life.’ (Female with breast cancer and multiple sclerosis)
Discussion
Statement of principal findings
In this large citizen science study, we engaged 1636 participants in generating and reflecting on ideas to improve their care. This led to the identification of 3613 ideas from patients to improve 147 areas of care at consultation, hospital/clinic and health system levels. To our knowledge, this is the first study to provide a comprehensive and patient-defined list of areas of improvement in our care system and practical ideas to enact these changes. Patients’ ‘ideal’ care was not very different from the models advocated in the medical literature.35 Care for patients with chronic condition should be effective but minimally disruptive.36 Professionals should work as teams and coordinate their efforts.37 Care should be patient centred and have a holistic approach rather than be disease focused and fragmented.4 38–40 Low-value exams and treatments should be avoided.41 Our collective intelligence study generated practical ideas to get closer to this ideal.
Strengths and weaknesses of the study
This study has several strengths. First, we used an innovative data collection method involving both an initial consultation and an enrichment step. Besides significantly augmenting our data, this collective intelligence approach reinforced patients’ participation in research: patients were informed about the progress of the analysis and were involved in its finalisation.31 Second, the impact of investigators’ preconceptions on the analysis was reduced by (1) the independent analysis of data by multiple researchers, each supplementing and/or contesting others’ statements, and (2) the triangulation of our findings by patients themselves.42 Finally, our study included a large sample of participants with diverse diseases, education level and place of residence. This diverse sample enabled the collection of a comprehensive list of areas for improvement and an abundant number of patients’ ideas.
This study has several limitations. First, because we used open-ended questions, the number of times an idea appeared in our data depended on its elicitation. Frequently elicited ideas are not necessarily those most ‘desired’ by participants but those that were the most evident to them. However, this problem may have been mitigated by our two-step method in that participants were able to react to and reflect on others’ ideas. Second, we made the methodological choice to use online surveys with open-ended questions as an alternative to face-to-face data collection methods such as interviews or focus groups in order to gather ideas from a larger and more diverse population. Using an online questionnaire prevented any adaptation to participants’ responses and in-depth probing for more specific information. This choice was a deliberate trade-off between richer answers and more diverse participants, in line with our objective to identify a large amount of different ideas on how to improve the care for patients with chronic conditions. Similarly, the classification of ideas in areas of improvement was driven by their similarity in the contexts, people and processes involved to implement them. Other analysis frameworks could have yielded different results, focused on different aspects of the data. Third, our population is not representative of the general population of patients with chronic conditions. Similar to other online studies, our results reflect a large proportion of younger and more educated women.43 44 Regardless, we were able to include a large number of older and less educated patients. In the same way, the use of an online questionnaire may have favoured the participation of patients with striking experiences, with a message to convey, or those who were more invested in their care. Finally, the transferability of our findings is cautioned. Most (98%) of our participants lived in France. Thus, the pitfalls of the system and ideas for improvement were closely tied to the specificities of the French healthcare model (eg, universal health coverage, institutional polycentrism).45 As an example, most patients in France benefit from free-of-charge care for their chronic conditions; hence, our participants desired simpler administrative tasks to obtain reimbursement for health expenditures (n=142, 9%) rather than asking for lower health expenses (n=27, 2%).
Comparison with other studies
The literature on satisfaction/experience of care of patients with chronic condition is very rich.24 46 47 Our study complements it by asking a conceptually different question: ‘What if our care was designed by patients?’ Indeed, only a handful of studies involved patients in pointing out precise areas of care that should be transformed and how, and the studies were often limited to specific settings or topics.22 48 For example, a recent initiative involved patients, families and professionals in the USA in finding ‘health rules’ that should be broken for a better experience of patients or staff.27 Obviously, patients’ answers were driven by their experience and may overlap with problems already identified. However, our approach also led to the identification of proposals that have, to our knowledge, not been explored before.
In addition, ours is the first study to systematically gather, on a large scale, patients’ ideas to improve the healthcare system. Our results are not limited to a single topic, type of change or context; rather, they outline the major care paradigms that should be addressed to improve care, independent of patients’ conditions or management place. In that sense, our findings have more in common with patients’ feedback on medical practices that are systematically collected by health organisations or institutions via discharge surveys, patients’ feedback on online platforms or complaint procedures.49–51 Unfortunately, this routinely collected feedback is often underused by health organisations that collect them and thus only rarely lead to quality improvement.49 52
Implications for clinicians and policymakers
The sharp contrast between the number of patient feedback procedures in health organisations and the reality of care, as experienced by patients, leads us to question the impact of these procedures. Evidence shows, for example, that most physicians mistrust results from patient feedback surveys and question their design, the framing of questions and the fact that they collect numerical data that do not account for the answer’s context.53 As stated by Coulter, ‘Stories trump data.’54 Stories are more powerful than numerical feedback for capturing the interest of staff and changing minds.49 55 Our work aims at embodying a collection of such stories focused on ‘informing, infecting, irritating, and igniting a chain reaction that makes the status quo unsustainable (…) in a push for healthcare that is careful and kind to each patient and community.’56 Our work is also an original repertoire of ideas that can be used by researchers, translated into patient-relevant interventions or organisational changes and evaluated in rigorous research.
Beyond our findings, this study is the proof of concept of a method to leverage the untapped resource of patients’ knowledge and experience to improve care. This process may be replicated locally, in departments or hospitals, as a new way to generate patients’ feedback for identifying bottlenecks in the system and ideas to improve it. It may also be implemented on a larger scale to guide healthcare policies, although new tools to analyse larger and ever-growing amounts of qualitative data will be required. Although our results were at the small scale, they have already been taken into account by the French government in its consultations in preparation for elaborating the national strategy to transform the healthcare system.57 Future steps may involve exploring how patients’ ideas identified in this study would be prioritised or valued by different groups.
Finally, our results must remind those who work every day with patients—whether at patient reception or in the doctor’s office—that top-down strategies (eg, policies, regulations, rules and restructuration) are not the only proponents to improve the quality of care. Professionals should not wait for their institutions or organisations to act. By simply engaging in discussions with patients, they and their patients can already identify key areas of their work that they can improve and move things by themselves—the first steps to a Patient Revolution.
Conclusion
In this study, we engaged patients with chronic conditions, on a large scale, to identify which components of the care system require improvement and to generate ideas to do so. Patients proposed many ideas to improve their care, from the content of consultations to the organisation of hospitals. Our study provides the proof of concept for a method to leverage patients’ practical knowledge of the care system to improve it.
References
Footnotes
Contributors Generated the idea: VTT and PR. Conceived and designed the experiments: VTT and PR. Collected data: VTT and PR. Analysed data: VTT, CR, CP, AC and PR. Wrote the first draft of the manuscript: VTT. Contributed to the writing of the manuscript: VTT, CR, CP, AC and PR. Agree with manuscript results and conclusions: VTT, CR, AC and PR. VTT is the guarantor, had full access to the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Funding ComPaRe was funded by the Assistance Publique-Hôpitaux de Paris (APHP) and Paris Descartes University.
Disclaimer The authors have no association with commercial entities that could be viewed as having an interest in the general area of the submitted manuscript.
Competing interests None declared.
Patient consent for publication Obtained.
Ethics approval ComPaRe was approved by the Institutional Review Board of Hôtel-Dieu Hospital, Paris (IRB: 0008367).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.