Article Text

Abstract
Background Studies in operating rooms (OR) show that minor disruptions tend to group together to result in serious adverse events such as surgical errors. Understanding the characteristics of these minor flow disruptions (FD) that impact major events is important in order to proactively design safer systems
Objective The purpose of this study is to use a systems approach to investigate the aetiology of minor and major FDs in ORs in terms of the people involved, tasks performed and OR traffic, as well as the location of FDs and other environmental characteristics of the OR that may contribute to these disruptions.
Methods Using direct observation and classification of FDs via video recordings of 28 surgical procedures, this study modelled the impact of a range of system factors—location of minor FDs, roles of staff members involved in FDs, type of staff activities as well as OR traffic-related factors—on major FDs in the OR.
Results The rate of major FDs increases as the rate of minor FDs increases, especially in the context of equipment-related FDs, and specific physical locations in the OR. Circulating nurse-related minor FDs and minor FDs that took place in the transitional zone 2, near the foot of the surgical table, were also related to an increase in the rate of major FDs. This study also found that more major and minor FDs took place in the anaesthesia zone compared with all other OR zones. Layout-related disruptions comprised more than half of all observed FDs.
Conclusion Room design and layout issues may create barriers to task performance, potentially contributing to the escalation of FDs in the OR.
- surgery
- healthcare quality improvement
- patient safety
- interruptions
- physical environment
- built environment
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- surgery
- healthcare quality improvement
- patient safety
- interruptions
- physical environment
- built environment
Introduction
The operating room (OR) is a particularly high-risk environment, prone to surgical site infections, surgical accidents and staff injuries.1 Direct observations of ‘work as done’ reveal a range of disruptions in the natural flow of surgical procedures demonstrating mismatches between the demands of tasks required to meet surgical goals, and the configuration of the system to enable that.2–6 High rates of these flow disruptions (FD) contribute to higher stress,7 higher perceived workload for surgical staff,5 increased surgery duration,8 9 surgical errors6 10 and increased patient mortality.11 By diagnosing and addressing the systems design issues that lead to FDs in the OR, it may be possible to improve safety, and thus improve patient outcomes.
These FDs vary in the extent to which they impact the surgery and the surgical staff. Some FDs are barely noticed, while others may lead to distractions, elongated surgical pauses or a change in strategy in order to address the problem.3 One study found that surgical errors increased significantly during cardiac surgery with increases in FDs.6 9 In another study, covering cardiac and orthopaedic surgery, minor problems were observed to ‘group together’ to create more serious, clinically significant, FDs.2 Minor disruptive events that overlap can produce an intensity of interference that likely contributes to major events.3 In an observational study of 173 congenital cardiac surgery cases, de Leval et al found that the number of minor events per case was related to deaths and clinical near misses.11 In isolation they did not make an impact, but there was a multiplicative effect of multiple minor events. These studies highlight the importance of systematically studying the relationship between minor and major FDs in the OR in order to understand the contribution of these minor FDs to patient safety outcomes.
Sources of FD in the OR include equipment malfunction, door openings, case irrelevant conversations, loud noises and alarms, communication breakdowns, environmental clutter and constrained spaces.12 13 The built environment in particular provides the context for the delivery of care but has rarely been studied in any level of detail as a source of FD in the OR. According to Wahr et al,12 small and cluttered ORs, high traffic in and out of the OR and large number of people in the OR contribute to FDs as well as higher infection risk. Inadequate utilisation of space and inefficient equipment placement were identified as key factors contributing to FDs associated with the OR layout.4 Gurses and colleagues14 found that layout and traffic-related OR characteristics such as inadequate room size, lack of organisation for storage of instruments and equipment, cluttered workspaces and lack of proximity between key functional areas in the OR compromised patient safety. Consider a scenario where the circulating nurse (CN) needs to walk around or through a constrained space near the scrub nurse and the instrument tables to reach a particular storage space in the OR. This increased movement may lead to higher physical workload, unnecessary movement, collisions with other staff or equipment, dropped instruments and distraction away from surgical tasks.
The purpose of this study is to use a systems approach to investigate the aetiology of minor and major FDs in ORs in terms of the people involved, tasks performed and OR traffic, as well as the location of FDs and other environmental characteristics of the OR that may contribute to these disruptions. Specifically, a regression model was developed that allowed the exploration of how minor and major FDs were related. By including OR layout and OR traffic characteristics in the models, we seek to better understand how layout and traffic affected the occurrences of both minor and major FDs during surgery.
Method
Data collection
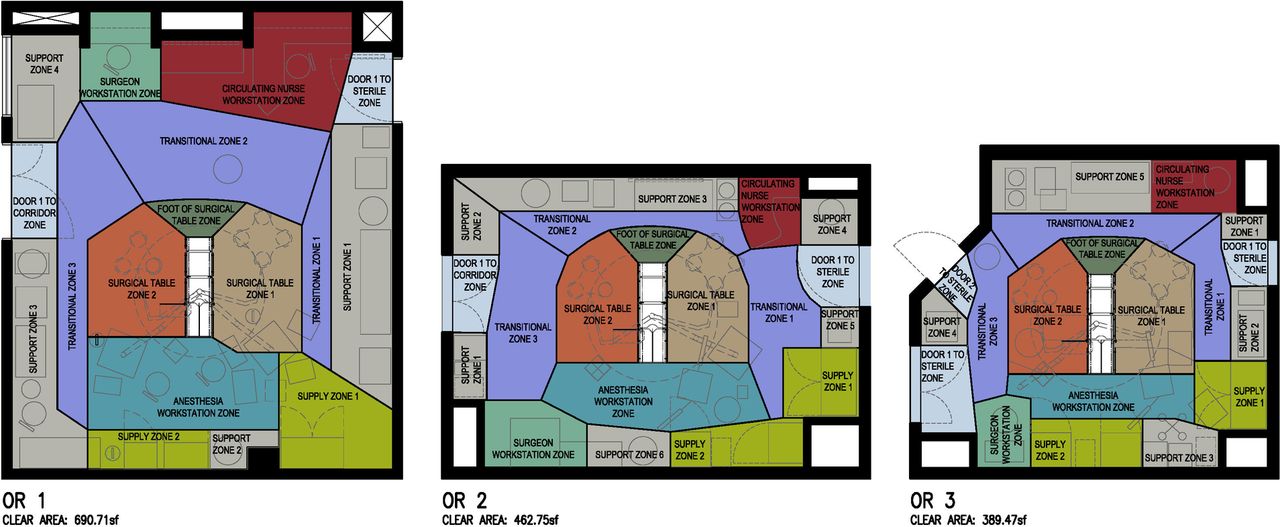
This study used a convenience sample of 28 prerecorded videos from three different ORs (figure 1) in a large academic hospital system. Video recordings of surgeries were captured using four video cameras located in the four corners of the OR to maximise visibility. The recordings were initiated before patient entry and ended after patient exit from the room. For the purpose of this study, observation time was defined as patient-in-room to procedure finish (including both the preoperative and intraoperative phases of the surgery). The videos were then analysed using Noldus Observer XT V.12 software, and the surgical staff members’ locations, activities and FDs were coded. Two graduate students with background in human factors were trained to code the recorded surgeries where each staff member’s location and activity was coded for the duration of the observation. A third graduate student coded FD under the supervision of the first author. All coders participated in 12 in-person observations in the OR and were familiarised with the coding scheme. They also received education on human factor issues in surgical environments from clinical and human factor experts on the research team.
{kind=link}
Disposition of zones in the three operating rooms (OR) observed.
As part of training, pilot coding of three surgeries was conducted by the students to assess the intercoder reliability. The intercoder reliability was measured based on Cohen’s kappa statistic and was obtained through the built-in feature in Noldus Observer XT V.12. Due to the initial low reliability score, a calibration session was held with students and senior researchers to review the disagreements in coding. Codes that were confusing were modified or removed to increase reliability. A second reliability test was done after another round of coding where an acceptable intercoder reliability of K=0.83 was achieved.
Activities performed by core surgical staff members (surgeons, CN, scrub nurse and anaesthesia team) were coded into one of four categories: patient-related tasks (P), equipment-related tasks (E), material and supply-related tasks (M) and information-related tasks (I). Together with a fifth category staff (S) that was accounted for through the other four codes, these tasks are termed as PEMSI tasks. Locations were determined by OR zones, which were bounded and defined according to the type of function conducted in them. Functional zone categories included support, supply, door, surgical table and workstation zones, as depicted in figure 1. Transitional zones connect most of the zones together. All ORs observed as part of this study contained all the functional and circulation zones. However, the ORs varied slightly in terms of their size, the physical location of the zones within the OR and size of the zones.
An existing taxonomy developed by Palmer and colleagues was adapted and used as the basis for categorising FDs.4 In terms of type, disruptions were classified into five categories: layout, environmental hazards (EH), usability, interruption and equipment failure (EF). Layout disruptions were defined as events where surgical staff had to adapt to inadequate space; impeded visibility; and the positioning of connectors, equipment, furniture and fixed structures in the OR. EH disruptions were defined as events where surgical staff actively interacted with the environment, such as slipping, falling, tripping; interacting with sharp objects and contaminated needles; colliding with staff, equipment or furniture; and excessively reaching to access patient, objects or equipment. Usability disruptions were defined as disruptions associated with the operation of physical elements (such as computers, equipment, surfaces, sterile field barriers such as surgical drapes, and packaging materials containing supplies and instruments) within the OR environment. Interruption disruptions were events where surgical staff was diverted from their task due to phone calls or pagers; looking at personal phones; non-essential personnel in the room; spilling or dropping equipment; shift changes; door openings; missing supplies or instruments; and searching for missing surgical items. Finally, EF disruptions were defined as events related to missing, broken or malfunctioning equipment during surgery.
All disruptions were classified as individual events with a range of associated characteristics such as FD type, location, roles of staff involved, number of staff involved and activities of all staff during the FD. Additionally, the severity of each disruption was classified into one of six categories (1—no impact/minor disruption-no response; 2—momentary disruption (acknowledgement of disruption, no pause in task); 3—momentary distraction (short pause <10 s); 4—primary task interrupted (task cessation >10 s); 5—primary task disruption (secondary task engaged); 6—repeat task) developed by Parker et al.15 For the purposes of further analysis, in this study, we define any FD that results in a pause or break in the primary activity as a ‘major flow disruption’ (categories 3–6). All other FDs are termed as ‘minor flow disruptions’ (categories 1 and 2).
This study also focuses on how traffic in the OR may contribute to FDs. Transitions between OR zones, the number of staff in the OR and the density in the OR were used to measure traffic in the OR. The number of transitions in the OR is measured by the total number of transitions that occurred across the observation time for each procedure, where a transition was counted as the movement of a staff member from one zone to another. The number of staff in the OR is measured as the average of the number of staff members present inside the OR across the entire observation time. The density of a zone is defined as the area occupied by staff and equipment divided by the available area of that zone. The average density of the OR is defined as the average of the densities of all zones recorded during the observation time.
Statistical analyses
The event-based data around FDs were converted into time-based data with 1 s intervals to facilitate statistical analysis. In order to control for differences in the observation times across surgeries, all linear regression analyses were based on event rates per hour. The most widely used diagnostic for multicollinearity, the variance inflation factor (VIF), was used to control high correlations among variables. In developing the regression models, it was necessary to remove correlated predictors, and to remove certain variables where there was insufficient sample size. For all regression analyses, a p value less than the critical level 0.05 was considered statistically significant. All logistic regression models were built on the original data in 1 s intervals.
A series of linear regression models was constructed to investigate how major FDs are affected by minor FDs defined by different characteristics. A second phase of the analysis explored the potential relationships between specific traffic factors and FDs of any type (major or minor). Both linear and logistic regression models were introduced to test the significance of the three traffic-related variables—the number of transitions in the OR, the average density of the OR and the number of staff in the OR. Finally, a combined regression model was developed that included all variables found to be significant in the preceding analyses. For the final regression model, VIFs were in the range (1.2, 6.2) with mean 2.8, where the standard interpretation is that only moderate correlation exists. Based on this result, a regression approach was determined. The Shapiro-Wilk test was used to check the normality of residuals (errors), implying that the residuals were approximately normally distributed with neither significant outliers nor high leverage points.
Results
Twenty-eight surgeries conducted in three different ORs were video recorded (table 1). The observation times varied from 14.2 to 216.2 min with an average length of 78.6 min and SD of 53.68. Multiple surgery types were observed including band removal (n=2), cholecystectomy (n=5), gastric bypass (n=3), paediatric (n=12) and other operations (n=6). Table 1 shows the average number of minor and major disruptions per hour and per observation for different types of surgeries as well as the three different ORs.
Average number of minor and major flow disruptions per hour and per case for different types of surgeries as well as the three different ORs
A total of 2504 FDs were observed across the 28 surgeries in this sample. Of this, 658 (26%) were major disruptions and 1846 (74%) were minor disruptions. Approximately 73% of minor FDs were classified as ‘Momentary with no pause’, implying that it resulted in no discussion or change in behaviour or action, at least in terms of how that minor FD was handled. In 98% of major FDs, a surgical staff member(s) either was momentarily distracted or had a pause or interruption in her/his task. In only 2% of all disruptions categorised as major FDs did the surgical staff member(s) actually engage in a secondary activity or repeat the surgical task. At the time of happening of these types of major FDs, surgical team members were involved in performing tasks related to material, instrument, supplies (31%), information (27%), equipment (21%) and the patient (21%).
Around 80% of all FDs occurred in the anaesthesia workstation zone, transitional zones and surgical table zones (table 2). The anaesthesia workstation zone accounts for approximately 30% of minor and major FDs, most of which were layout related, while the footprint of this zone in the OR accounts for only 10% of the total OR area. Furthermore, transitional zones 2 and 3 contain more FDs compared with transitional zone 1. The support zones accommodated FDs twice as often as the supply zones. More than 80% of FDs involved a single staff member, with the anaesthesia team and the CN accounting for more major and minor FDs than any other category.
Frequency of major and minor flow disruptions by their type, location, number and role of staff involved
As table 2 shows, more than half of all FDs originated from layout-related issues. Further, layout-related disruptions were dominant in all OR locations and for all staff roles. In addition to the layout-related FDs, around one-third of minor FDs were EH-related FDs. However, a significant number of major FDs (30%) occurred due to interruptions such as non-essential staff entering the OR, spilling or dropping of equipment and searching activities because of missing items in the OR.
We tested several potential variables to represent the occurrences of minor disruptions by disruption type, disruption location, OR type, number/role of staff and other traffic-related measures, and only those variables with significant association to major FDs are reported below.
Relationship between minor and major FDs
The rate of major FDs increased linearly with increases in the rate of minor FDs (r=0.61, p≈0). A multiple linear regression model was developed to explore the relationship between major FDs and specific characteristics of minor FDs. The results reveal that increases in layout-related minor FDs significantly increase the rate of major FDs. Further, there was a significant association between minor FDs related to equipment/furniture positioning and the rate of major FDs. Moreover, increases in minor FDs that occur in transitional zone 2 significantly increased the rate of major FDs. The results also indicate a significant relationship between minor FDs, in which the anaesthesia team members are involved, and the rate of major FDs. Furthermore, there was a significant association between minor FDs in which the CN is involved and the rate of major FDs. Also, higher rate of minor FDs during equipment-related activities significantly increases the rate of major FDs (see online supplementary appendix for more details).
Supplementary file 1
Impact of transitions, density and number of staff on FDs
There was no significant association between the traffic-related factors and the rate of major FDs. However, increases in the average density of transitional zone 2 slightly increase the rate of major FDs. Further, the result shows that the rate of major FDs increases significantly with increases in the number of transitions to and from transitional zone 3 and surgical table zone 1. Also, there was a significant association between the number of transitions in the OR as well as the average density of the OR and the occurrence of FDs (see online supplementary tables A1 and A2 for more details).
Major FDs explained through a single, combined regression model
The purpose of the combined regression model (table 3) was to analyse which factor(s) significantly contribute to the overall model, when all variables found to be significant in the individual models were entered into the model simultaneously. The result shows a significant association between minor FDs that occurred during equipment-related activities and the rate of major FDs in the presence of all potentially significant predictors. Equipment-related activities included monitoring, preparing, moving and organising equipment in the OR. Additionally, increases in minor FDs involving the CN also significantly increased the rate of major FDs. Furthermore, a higher rate of minor FDs in transitional zone 2 slightly affects the rate of major FDs.
Multiple regression analysis—relating minor flow disruptions and traffic-related factors to major flow disruptions
Discussion
Using direct observation and classification of FDs via video recordings of surgical procedures, this study looked at a range of factors—location of minor FDs, roles of staff members involved in FDs, type of staff activities as well as OR traffic-related factors—in order to understand the relationship of these system factors to major FDs in the OR. We found that the rate of major FDs increases as the rate of minor FDs increases, especially in the context of equipment-related FDs, equipment positioning and specific physical locations in the OR. CN-related minor FDs and minor FDs that took place in the transitional zone 2, near the foot of the surgical table, were also related to an increase in the rate of major FDs. This study also found that more major and minor FDs took place in the anaesthesia zone compared with all other OR zones.
To our knowledge, this was the most comprehensive attempt to observe and model FDs and their systemic causes. Previous observational studies of OR environments have shown that minor disruptive events tend to group together to result in serious adverse events such as surgical errors, which impact patient safety.2 6 11 Understanding the characteristics of these minor FDs that may be related to major events is important in order to proactively design safer systems. This study found that minor FDs that occurred while performing equipment-related activities were related to increases in major FDs. Our findings are in keeping with other studies that have found equipment-related problems to be the source of FDs in the OR.6 16 17
The transitional zone in the OR might be an important location to consider from a design perspective, as an increase in minor disruptions in this part of the OR was slightly related to an increase in the rate of major FDs. In particular, the transitional zone connects the CN workstation zone with the foot of the surgical table, where instrument tables and the scrub nurse are located and where the CN frequently visits during the surgery. Moreover, the CN is a potential subject in contributing to major FDs, as he/she plays a key role in supporting the progress of the procedure and the surgical team. If the transitional zone is cramped or overcrowded with equipment and people, it could well contribute to multiple minor FDs as the CN moves back and forth to his/her workstation. This zone should be optimally sized while designing ORs.
While the traffic-related factors were not significantly related to major FDs in the overall model, the number of transitions between OR zones and the overall density or crowdedness in the OR significantly impacted the occurrence of any type of FD. Previous studies have identified the high number of door openings and people moving in and out of the OR as key factors impacting disruptions.18 19 However, the contribution of movements within the OR to disruptions has not been empirically studied. A larger number of movements between zones in the OR could potentially be an indicator of a suboptimal OR layout that requires staff members to make frequent trips to different parts of the OR to retrieve items. Placing functional zones such as supplies and storage close to staff members who need to access these areas will help reduce the number of trips (and associated movements) within the OR.
It has been noted that crowded and cluttered ORs contribute to FDs but no quantitative metrics have been put forth to measure crowding in these studies. Some studies have shown that the number of people in the OR may be an important consideration, related to OR traffic and higher infection risk.17 20 One solution to reducing crowding in the OR has been to design larger ORs. However, some zones within the OR, such as the anaesthesia zone, still end up being crowded with equipment and people, while other parts of the OR remain underused. By developing a measure for both overall OR density and perhaps more meaningfully, the density of individual zones within the OR, this study puts forth metrics that could be used by future studies to quantify crowding in different parts of the OR. Evaluation of zone density of different zones in proposed OR designs may also help in identifying potential problem areas and trigger discussions around the design of the spaces to support the tasks, equipment and people using the space. Another area for future research is to identify temporal relationships between minor and major FDs. This line of inquiry may be useful in developing predictive models that help signal major disruptions before they occur.
This study is arguably the most detailed analysis of the relationship between FDs, surgical tasks and the OR workspace ever conducted. However, it has some limitations. While the video observation approach allowed for in-depth and thorough coding of FDs and surgical staff behaviours at the macro scale of the OR, the surgical site was not videotaped. As such, the impacts of FDs in the OR on the surgeon’s performance could not be evaluated. A future study may include a fifth video camera focused on the surgical site. The audio quality obtained from the recordings was poor due to noise from equipment and alarms. As such, communication-related disruptions were hard to observe and record. While the type of team member (anaesthesiologist, nurse) involved in the FD was coded, the data could not be linked to a specific individual since there were often multiple people of the same job type in the OR. As such, it is difficult to obtain a deep contextual understanding of a FD from these data such as, how the FD may have affected the task at hand (either positively or negatively) without further coding. The type of data obtained from the 28 surgeries in this study is very extensive. However, a relatively small sample of surgeries was studied in multiple ORs. Further, different types of surgeries were included in the sample and variations among procedures could potentially confound findings.
FDs demonstrate mismatches between surgical task demands and the configuration of the system of work. In essence, they demonstrate design issues that, if addressed, provide opportunities for efficiency and safety improvements. This developing area of patient safety science has demonstrated both downstream impacts on efficiency and outcomes through the escalation of small problems to bigger, more dangerous situations, and upstream causes in terms of technology design, training, and patient and procedural complexity.5–7 In this study, we have demonstrated that room design and layout can also contribute to these critical escalation patterns. Our future studies will use this knowledge to inform improved designs of ORs.
References
Footnotes
Contributors The authors are the sole contributors of all text, images and tables included in the manuscript.
Funding The study was funded by the Agency for Healthcare Research and Quality (P30HS024380, 2015).
Competing interests None declared.
Patient consent Not required.
Ethics approval Medical University of South Carolina.
Provenance and peer review Not commissioned; externally peer reviewed.
Collaborators Scott Reeves, David Allison, Sara Riggs, James Abernathy, Dee San, David Neyens, Larry Fredendall, Yann Ferrand, Deborah Wingler, Katie Jurawicz, Scott Betza, Brandon Lee, Roxana Jafarifirozabadi, Zahra Zamani