Article Text

Abstract
Background Large-scale real-world data to evaluate the impact of chest pain centre (CPC) accreditation on acute coronary syndrome (ACS) emergency care in heavy-burden developing countries like China are rare.
Methods This study is a retrospective study based on data from the Hospital Quality Monitoring System (HQMS) database. This study included emergency patients admitted with ACS to hospitals that uploaded clinical data continuously to the database from 2013 to 2016. Propensity score matching was used to compare hospitals with and without CPC accreditation during this period. A longitudinal self-contrast comparison design with mixed-effects models was used to compare management of ACS before and after accreditation.
Results A total of 798 008 patients with ACS from 746 hospitals were included in the analysis. After matching admission date, hospital levels and types and adjusting for possible covariates, patients with ACS admitted to accredited CPCs had lower in-hospital mortality (OR=0.70, 95% CI 0.53 to 0.93), shorter length of stay (LOS; adjusted multiplicative effect=0.89, 95% CI 0.84 to 0.94) and more percutaneous coronary intervention (PCI) procedures (OR=3.53, 95% CI 2.20 to 5.66) than patients admitted in hospitals without applying for CPC accreditation. Furthermore, when compared with the ‘before accreditation’ group only in accredited CPCs, the in-hospital mortality and LOS decreased and the usage of PCI were increased in both ‘accreditation’ (for in-hospital mortality: OR=0.86, 95% CI 0.79 to 0.93; for LOS: 0.94, 95% CI 0.93 to 0.95; for PCI: OR=1.22, 95% CI 1.18 to 1.26) and ‘after accreditation’ groups (for in-hospital mortality: OR=0.90, 95% CI 0.84 to 0.97; for LOS: 0.89, 95% CI 0.89 to 0.90; for PCI: OR=1.36, 95% CI 1.33 to 1.39). The significant benefits of decreased in-hospital mortality, reduced LOS and increased PCI usage were also observed for patients with acute myocardial infarction.
Conclusions CPC accreditation is associated with better management and in-hospital clinical outcomes of patients with ACS. CPC establishment and accreditation should be promoted and implemented in countries with high levels of ACS.
- healthcare quality improvement
- medical emergency team
- teamwork
- quality improvement
Data availability statement
Data are available upon reasonable request. The data that support the findings of this study are available from China Standard Medical Information Research Center but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors upon reasonable request and with permission of China Standard Medical Information Research Center.
Statistics from Altmetric.com
Introduction
Cardiovascular disease now accounts for approximately one-third of all deaths globally.1 In 2015, the age-standardised mortality rate of cardiovascular disease was 285.5 per 100 000 individuals.2 In China, ischaemic heart disease was the second leading cause of disease death at the national level,3 and age-standardised mortality from ischaemic heart disease increased more than 20% from 1990 to 2017.3
Despite the existence of guideline-recommended diagnostic and therapeutic strategies, there are gaps between best evidence and real-world practices.4 A large number of patients with ST-elevation myocardial infarction (STEMI) do not receive reperfusion therapy, which is the most effective treatment. The percentage of any reperfusion treatment use in European countries varied from 37% to 93% in 2005–20085 and was around 55% during 2001–2011 in China.6 Clinicians face several barriers to the adoption of best practice; the potential barriers to physician guideline adherence include awareness, familiarity, agreement, self-efficacy, outcome expectancy and ability to overcome the inertia of previous practice.7 Organisations also struggle with how best to manage different departments and resources. Organised primary percutaneous coronary intervention (PCI) networks are associated with higher reperfusion therapy rates.8 The purpose of a chest pain centre (CPC) accreditation programme is to monitor and encourage organisations and clinicians to adopt standards for patients with chest pain, by identifying and then resolving real and perceived barriers.4–6 8–10
The USA and Germany have widely adopted national programmes for professional society accreditation as a CPC or chest pain unit and have showed improvements in the management11 or clinical outcomes of patients with acute myocardial infarction (AMI).12–14 Consistently, Fan et al 15 reported that CPC accreditation was associated with a lower incidence of 7-day all-cause death and major cardiovascular events of AMI in China. However, few studies have compared the management and clinical outcomes of patients with acute coronary syndrome (ACS) admitted before and after CPC accreditation using big data from developing countries with a heavy burden of disease. Using a national database, this study was therefore performed to evaluate whether CPC accreditation is associated with better management and lower in-hospital mortality of patients with ACS using different comparison methods in China.
Methods
CPC accreditation process in China
To mainly improve the management of patients with ACS and achieve early reperfusion in patients with AMI, a CPC accreditation programme was officially initiated in China in 2013, using Chinese standards. The Headquarters of China CPCs was established in 2016 for systematic accreditation management.
The China CPC accreditation programme tries to promote the management of patients with acute chest pain by establishing a regional emergency care network. Five main elements are included in China CPC accreditation: the basic framework, diagnosis and treatment of acute chest pain, cooperation between emergency medical services and the in-hospital emergency system, education and training, and continuous improvement. Hospitals at different levels and regional emergency medical systems are involved in a continuous accreditation process to establish regional emergency care networks under the regulation of the Headquarters of China CPCs. To receive accreditation, hospitals applying for accreditation must develop an in-hospital process, start network construction, and then register on the official website of the Headquarters of China CPCs (www.chinacpc.org). Besides, hospitals must submit documentation, upload data for evaluation and receive the investigation for both online and onsite methods by three experts from the Headquarters of China CPCs.16 Hospitals must also upload data about acute chest pain care for at least 6 months and show continuous improvement evaluated by a series of key performance indexes before formal accreditation.17 The Headquarters of China CPCs will help them to identify and resolve any barriers by providing training.
Data source
This retrospective analysis was based on the Hospital Quality Monitoring System (HQMS), a national administrative database authorised by the National Health Commission of the People’s Republic of China.18 The HQMS, an official online data collection system covering all tertiary hospitals, is a mandatory patient-level national database for hospital accreditation. This study was authorised by the HQMS Committee Board and approved by the ethics committee of Peking University First Hospital.
Identification of patients with AMI and ACS and definitions of comorbidities
The present analysis included adult patients with ACS admitted on an emergency/urgent basis to hospitals whose front-page medical record data were continuously uploaded to the HQMS database from 2013 to 2016. ACS includes STEMI, non-STEMI and unstable angina, and AMI includes both STEMI and non-STEMI. The International Statistical Classification of Diseases (ICD) used was shown in online supplemental table 1). Similar to previous studies,18 ACS and AMI were identified using discharge diagnosis codes from the 10th revision of the International Statistical Classification of Diseases (ICD-10). The validity of this approach to define AMI in administrative data has been previously documented.19 For patients with more than one ACS record, only the first hospitalisation with ACS was included in this study. Records with missing information about sex, age and death status at discharge were excluded. Comorbidities including hypertension, diabetes, old myocardial infarction, percutaneous coronary intervention (PCI) during hospitalisation and heart failure were also defined using discharge ICD codes. Three sets containing the most detailed ICD codes (Beijing RC020-ICD-10 version, National Clinical Edition 1.1 and National RC020-ICD-10 version) and two sets containing operation codes (National Clinical Edition 1.1 and Beijing RC022-ICD-9 version) were used from different editions of the ICD dictionary accordingly. All code sets and rules were reviewed separately by at least two experienced cardiologists.
Supplemental material
Definition of CPC accreditation status
Hospitals’ accreditation status was provided by Headquarters of China CPC in April 2018. For patients admitted to hospitals that had passed CPC accreditation, the CPC accreditation statuses were grouped as ‘before accreditation’, ‘undergoing accreditation’ and ‘after accreditation’. Patients who were admitted to hospitals 6 months or more before the corresponding date of accreditation were classified into the ‘before accreditation’ group, those who were admitted to hospitals between 6 months before the corresponding date of accreditation and the date of accreditation were classified into the ‘undergoing accreditation’ group and those who were admitted to hospitals after the corresponding date of accreditation were classified into the ‘after accreditation’ group.
Other variables
In addition to the original variables in the database, other hospital characteristics were obtained from the National Health Commission of the People’s Republic of China (https://www.hqms.org.cn). These data included the rank and type (specialised or general) of each hospital. In China, hospitals levels are divided into grade IIIA, B and C, grade IIA, B and C, and grade I levels, according to the scale, facilities and ability of the hospital, with grade IIIA being the highest level. In addition, hospital type is divided into specialised and general hospitals based on the medical specialty.
Statistical analysis
The statistical analysis was performed using R V.3.4.3 (http://www.R-project.org). Age is presented as mean±SD, and length of stay (LOS) and total charge are presented as median (IQR). Categorical variables are presented as number (percentage), and differences between CPC accreditation statuses were examined using the χ2 test.
We carried out the study in two parts. First, we used a cross-sectional design to compare the management and in-hospital clinical outcomes of patients with AMI and ACS admitted to CPCs against patients admitted to hospitals that had not applied for CPC accreditation. Propensity score matching was used to balance admission dates, hospital types and hospital levels. Patients admitted to CPCs were matched 1:2 with patients randomly selected from hospitals that had not applied for CPC accreditation based on the nearest neighbour in terms of the Mahalanobis distance with a calliper of 0.05. Mixed-effect models were then used in the matched data to control for hospital-related random effects, a logistic regression model was used for in-hospital mortality, a negative binomial model was used for the LOS and a generalised linear model with a log link and γ distribution was used for the charges. For in-hospital mortality and LOS, adjustments were made for sex, age, comorbidities (hypertension, diabetes, heart failure and old myocardial infarction), hospital type, hospital rank and geographical region. For total charge, adjustments were also made for PCI.
Second, we used a self-contrasted design that only included hospitals that had acquired CPC accreditation and had all three accreditation statuses: ‘before accreditation’, ‘undergoing accreditation’ and ‘after accreditation’. This design was used to evaluate the management and in-hospital clinical outcomes in these hospitals before and after CPC accreditation. Mixed-effect models were used: a logistic regression model for in-hospital mortality, a negative binomial model for the LOS and a generalised linear model with a log link and γ distribution for the charges. For in-hospital mortality and LOS, adjustments were made for sex, age, comorbidities (hypertension, diabetes, heart failure and old myocardial infarction), hospital type, hospital rank and geographical region. For total charge, adjustments were also made for PCI. All comparisons were two sided, with statistical significance defined as p<0.05.
Results
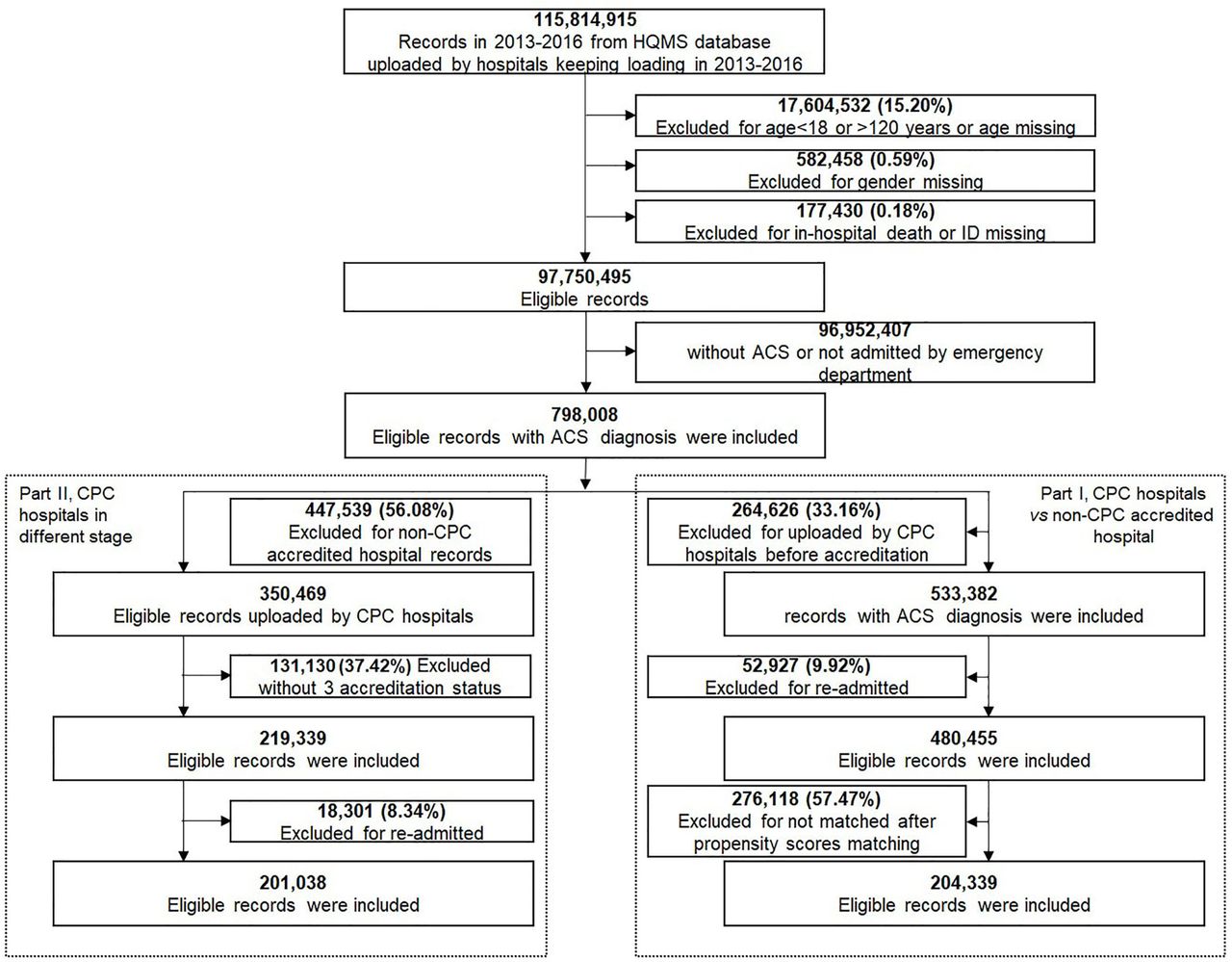
During the study period (1 January 2013–31 December 2016), 996 hospitals were covered in the HQMS database, and 746 of them continued to upload data during these 4 years. Of these 746 hospitals, 82 were accredited as CPCs and had all three accreditation statuses in the database. As shown in figure 1, 126 038 670 records were included in the HQMS database during the study period, and 115 814 915 of them were uploaded by hospitals that had continued to upload data during the study period. After excluding those with missing information for age and age <18 years (15.20%), missing information for sex (0.59%) or in-hospital death (0.18%), we included 97 887 921 eligible records, of which 798 008 were records of patients with ACS admitted on an emergency/urgent basis.
In the first part of the analysis, management and in-hospital clinical outcomes were compared between patients admitted to CPCs and patients admitted to hospitals that had not applied for CPC accreditation during the same period. Of the 798 008 records, 264 626 were excluded because they were uploaded by CPCs before they had passed accreditation, and another 52 927 were excluded because of readmission. For the remaining 480 455 patients, 1:2 propensity score matching was used to match the admission data, hospital levels and hospital types, and 204 339 of these patients were included in the matched database (figure 1). The characteristics of the 204 339 patients are summarised in tables 1 and 2. For patients with ACS, the in-hospital mortality rate, LOS and percentage of PCI procedures were 3.5%, 8 (5–11) days, and 35.3%, respectively. For patients with AMI, the in-hospital mortality rate, LOS and percentage of PCI procedures were 5.9%, 8 (6–12) days, and 50.4%, respectively. After matching for the admission date, hospital level and hospital type and adjusting for covariates, patients with ACS admitted to accredited CPCs had lower in-hospital mortality (OR 0.70; 95% CI 0.53 to 0.93), shorter LOS (adjusted multiplicative effect 0.89; 95% CI 0.84 to 0.94) and more PCI procedures (OR 3.53; 95% CI 2.20 to 5.66) than patients admitted to hospitals that had not applied for CPC accreditation. When adjustment for PCI was not made, patients admitted to CPCs had a higher total charge; however, when adjustment for PCI was made, CPC accreditation did not result in a higher total charge. Similar results were found for patients with AMI: those admitted to accredited CPCs had lower in-hospital mortality (OR 0.67; 95% CI 0.51 to 0.88), shorter LOS (adjusted multiplicative effect 0.91; 95% CI 0.86 to 0.96) and more PCI procedures (OR 3.54; 95% CI 2.15 to 5.85) than those admitted to hospitals that had not applied for CPC accreditation (table 3).
Characteristics of patients with ACS stratified by hospitals accredited and not accredited as CPCs

{kind=link}
Flow chart of data processing and record inclusion criteria. ACS, acute coronary syndrome; CPC, chest pain centre; HQMS, Hospital Quality Monitoring System.
In-hospital mortality and management of ACS stratified by hospitals accredited and not accredited as CPCs
The associations between in-hospital mortality, case management and chest pain centre accreditation in all hospitals
In the second part of the analysis, only records uploaded by hospitals with all three accreditation statuses (‘before accreditation’, ‘undergoing accreditation’ and ‘after accreditation’) were included. A self-contrasted design was used to evaluate the management and in-hospital clinical outcomes in these hospitals before and after CPC accreditation. Of the 798 008 ACS records, those not uploaded by hospitals with all three accreditation statuses were excluded, as were all readmission records. Ultimately, 201 038 patients with ACS were included in the analysis (figure 1S 1and online supplemental table 2). The average age was 63.6 years, and 36.2% of patients (n=72 718) were women. For patients with ACS, the in-hospital mortality rate, LOS and percentage of PCI procedures were 3.2%, 7 (5–11) days, and 38.2%, respectively (table 4). For patients with AMI, the in-hospital mortality rate, LOS and percentage of PCI procedures were 5.5%, 8 (6–11) days, and 55.6%, respectively. Patients with hypertension, diabetes, old myocardial infarction and heart failure accounted for 56.9% (n=1 14 437), 25.4% (n=50 969), 7.7% (n=15 467) and 24.1% (n=48 527), respectively.
In-hospital mortality and management stratified by chest pain centre accreditation status in accredited hospitals*
Table 5 shows the effect of CPC accreditation status on in-hospital mortality, LOS, use of PCI and total charge after adjusting for possible covariates in patients with ACS and AMI. Compared with the ‘before accreditation’ group, the in-hospital mortality rate was lower in both the ‘undergoing accreditation’ group (for patients with ACS: OR 0.86; 95% CI 0.79 to 0.93; for patients with AMI: OR 0.84; 95% CI 0.77 to 0.93) and ‘after accreditation’ group (for patients with ACS: OR 0.90; 95% CI 0.84 to 0.97; for patients with AMI: OR 0.90; 95% CI 0.83 to 0.97). Additionally, LOS was shorter in both the ‘undergoing accreditation’ group (for patients with ACS: adjusted multiplicative effect 0.94; 95% CI 0.93 to 0.95; for patients with AMI: adjusted multiplicative effect 0.94; 95% CI 0.93 to 0.95) and ‘after accreditation’ group (for patients with ACS: adjusted multiplicative effect 0.89; 95% CI 0.89 to 0.90; for patients with AMI: adjusted multiplicative effect 0.88; 95% CI 0.87 to 0.89). Furthermore, compared with the ‘before accreditation’ group, more PCI procedures were performed in both the ‘undergoing accreditation’ group (for patients with ACS: OR 1.22; 95% CI 1.18 to 1.26; for patients with AMI: OR 1.32; 95% CI 1.26 to 1.38) and ‘after accreditation’ group (for patients with ACS: OR 1.36; 95% CI 1.33 to 1.39; for patients with AMI: OR 1.49; 95% CI 1.43 to 1.54). When adjustment for PCI was not made, patients admitted ‘after accreditation’ had a higher total charge; however, when adjustment for PCI was made, CPC accreditation did not increase the total charge. We considered that patients with multiple ACS admissions would have a different risk at each admission, so we also performed a validation study using the last admission. The results remained the same (online supplemental tables 3–4).
The association between in-hospital mortality, case management and chest pain centre accreditation status in accredited hospitals*
Discussion
The current study revealed that CPC accreditation is associated with significant improvement in the management and clinical outcomes of patients with ACS admitted on an emergency/urgent basis using two comparison methods. First, a propensity score matching method combined mixed-effects models was used to control for pre-existing differences between CPC and non-CPC hospitals; compared with patients admitted to hospitals that have not applied for CPC accreditation, patients admitted to CPCs within the same period had lower in-hospital mortality, shorter LOS and more PCI procedures. Second, a self-contrast comparison with evaluate preimprovements/postimprovements was also conducted to further eliminate interhospital differences; compared with the ‘before accreditation’ group, the in-hospital mortality rate and LOS were significantly lower in both the ‘undergoing accreditation’ and ‘after accreditation’ groups among both patients with ACS and those with AMI. Likewise, the numbers of PCI procedures were higher in both the ‘undergoing accreditation’ and ‘after accreditation’ groups. The results of these two comparisons are consistent, which makes our results more robust.
In-hospital mortality is an important measure of quality of care in hospitals. The in-hospital mortality rate of AMI in our study was slightly higher than in Korea20 but lower than in Japan.21 In 2015, Kim et al 20 reported an in-hospital mortality rate of 3.9% among Korean patients with AMI. In a 2014 study by Ishihara et al,21 the in-hospital mortality rate among Japanese patients with AMI was 6.5%. In our study, the in-hospital mortality rate in non-CPC hospitals was 3.7% and 6.2% for patients with ACS and AMI. In CPC hospitals, it was 3.0% and 5.3%. Keller et al 22 reported that in a German chest pain unit, event-free 1-year survival for patients with ACS was improved. In accordance with Keller’s study, CPC accreditation in China also improved the quality of treatment in patients with ACS. The decreased in-hospital mortality in the present study can be explained by the following factors. (1) The in-hospital process of diagnosis and treatment was optimised with accreditation resulting in better guidance and arrangements such as timely reperfusion for patients with STEMI and risk stratification for patients with non-STEMI ACS. (2) Close cooperation between the hospital and emergency medical service was ensured, so the time before reperfusion was shortened. A study by Canto et al 23 revealed that patients with AMI transported to hospital by ambulance had greater and significantly faster receipt of initial reperfusion therapies. The use of prehospital ECGs was also showed to be associated with greater use of timely reperfusion therapy.24 (3) Another possible reason is hierarchical education for both physicians and patients in accordance with the criteria for CPC accreditation in China.
Previous studies have proven that timely primary PCI can reduce mortality in patients with STEMI.25 In a study by Ross et al, 12 in a US population, CPC accreditation was associated with greater use of PCI within 120 min of arrival at hospital. The accreditation standard for CPCs in China also emphasises the use of primary PCI for the rescue of patients with STEMI.26 However, we cannot differentiate PCI into primary and elective in this study. Alternatively, CPC accreditation was found to be associated with more widespread use of PCI for patients with ACS and AMI admitted on an emergency/urgent basis. In our study, after accreditation, about 60% of the patients with AMI admitted on an emergency/urgent basis received all kinds of PCI procedures. In another study, the rate of PCI at any time during hospitalisation increased from 23% to 78% over the period from 1999 to 2016 in an Australian population of patients with STEMI.27 Puymirat et al 28 reported that the rate of using any PCI in European Society of Cardiology member countries was 55% in 2009, which is similar to the rate in the ‘after accreditation’ group in our study. The certification standards in CPC accreditation in China may therefore be the reasons for the more widespread use of PCI during and after accreditation.
The LOS of both patients with ACS and AMI were longer for patients admitted to non-CPC hospitals comparing with those admitted to CPCs in our study. A recent study showed that the average hospital LOS for German patients with AMI was 8.66 in 2009.29 In the current study, the average LOS was longer than in the German study in the ‘before accreditation’ group but comparable in the ‘after accreditation’ group. In Germany, the LOS in patients with ACS was also reduced by establishing a chest pain unit.30 With respect to the total charge, CPC accreditation was associated with a higher total charge for both patients with ACS and those with AMI in the crude model; however, when adjustment was made for the use of PCI, CPC accreditation did not increase the total charge. This is reasonable because the fee for use of PCI is a non-negligible part of treatment of both AMI and ACS.
As a continuous process, hospitals applying for accreditation should upload their data on emergency care for acute chest pain to the Headquarters of China CPCs for at least 6 months. Final accreditation will be received only when improvements are observed. Thus, we used the 6 months prior to receiving accreditation as the ‘undergoing’ phase in our analysis. Similar with our results, Fan et al 15 found a slight decrease in the effect of CPC accreditation over time. This caused China to establish a reaccreditation project, with CPC accreditation lasting for 3 years. This helps to explain why improvements appear to occur from the ‘undergoing’ phase and emphasises the importance of continuous improvement.
This study has several limitations that must be considered when interpreting its results. First, the ICD classification cannot completely differentiate AMI into STEMI and non-STEMI. The separate effects of CPC accreditation on STEMI and non-STEMI are unknown. Second, the total ischaemic time of STEMI, defined as duration from symptom onset to target vessel open, was not available; thus, the process optimisation of STEMI care cannot be estimated in this study. Third, one of the goals of CPCs is to streamline the differential diagnosis of acute chest pain with different risks; in the present study, however, only in-hospital patients with ACS admitted through the emergency department were included. Whether CPCs can improve the quality of care for patients with low-risk ACS, such as those discharged by the emergency department, remains unclear and requires further study. However, using a database with a large sample size, this study was able to evaluate the effect of CPC accreditation using both a corresponding period and self-contrast design. It shows that there were significant improvements in both the management and in-hospital outcomes of patients with ACS in China.
In conclusion, CPC accreditation is associated with better management and in-hospital clinical outcomes of patients with ACS and AMI admitted on an emergency/urgent basis, including lower in-hospital mortality, shorter LOS and more widespread use of PCI. CPC establishment and accreditation need to be further promoted and implemented in countries with high levels of ACS.
Data availability statement
Data are available upon reasonable request. The data that support the findings of this study are available from China Standard Medical Information Research Center but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors upon reasonable request and with permission of China Standard Medical Information Research Center.
Ethics statements
Patient consent for publication
Ethics approval
This study was authorised by the Hospital Quality Monitoring System Committee Board and approved by the ethics committee of Peking University First Hospital.
Acknowledgments
The authors thank Headquarters of China Chest Pain Centres and the China Standard Medical Information Research Centre for their help and support throughout the study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors All authors meet the ICMJE recommendations for authorship and agree to be accountable for all aspects All authors meet the ICMJE recommendations for authorship and agree to be accountable for all aspects of the work. Yong Huo, Yan Zhang and Jianping Li contributed to the design and revising of the work; Pengfei Sun contributed to the acquisition, analysis, or interpretation of data for the work and drafting of the work. Haibo Wang, Hu Chen, Dingcheng Xiang, Weiyi Fang, Xi Su, Bo Yu, Yan Wang, Chunjie Li and Ying Shi contributed to the final approval of the version to be published. Xingang Wang, Bin Zhang, Yuxi Li and Min Mo contributed to acquisition of data.The authors thank Headquarters of China Chest Pain Centres and the China Standard Medical Information Research Centre for their help and support throughout the study.
Funding This study was funded by China-WHO Biennial Collaborative Projects 2016-2017 (design and collection parts).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.