Article Text

Abstract
Objective To estimate the incidence of avoidable significant harm in primary care in England; describe and classify the associated patient safety incidents and generate suggestions to mitigate risks of ameliorable factors contributing to the incidents.
Design Retrospective case note review. Patients with significant health problems were identified and clinical judgements were made on avoidability and severity of harm. Factors contributing to avoidable harm were identified and recorded.
Setting Primary care.
Participants Thirteen general practitioners (GPs) undertook a retrospective case note review of a sample of 14 407 primary care patients registered with 12 randomly selected general practices from three regions in England (total list size: 92 255 patients).
Main outcome measures The incidence of significant harm considered at least ‘probably avoidable’ and the nature of the safety incidents.
Results The rate of significant harm considered at least probably avoidable was 35.6 (95% CI 23.3 to 48.0) per 100 000 patient-years (57.9, 95% CI 42.2 to 73.7, per 100 000 based on a sensitivity analysis). Overall, 74 cases of avoidable harm were detected, involving 72 patients. Three types of incident accounted for more than 90% of the problems: problems with diagnosis accounted for 45/74 (60.8%) primary incidents, followed by medication-related problems (n=19, 25.7%) and delayed referrals (n=8, 10.8%). In 59 (79.7%) cases, the significant harm could have been identified sooner (n=48) or prevented (n=11) if the GP had taken actions aligned with evidence-based guidelines.
Conclusion There is likely to be a substantial burden of avoidable significant harm attributable to primary care in England with diagnostic error accounting for most harms. Based on the contributory factors we found, improvements could be made through more effective implementation of existing information technology, enhanced team coordination and communication, and greater personal and informational continuity of care.
- primary care
- general practice
- patient safety
Data availability statement
Data are available upon reasonable request. Anonymised summary data extracted from patient records regarding the avoidable harms detected in this study will be available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Healthcare-associated harm is an internationally recognised threat to public health and well-being. Across all income settings, as many countries aspire towards universal health coverage, attention has focused on the critical role of primary care-led healthcare systems to help achieve this goal.1 2 In countries like the UK, over 90% of clinical encounters are delivered in community settings,3 but a clear understanding of avoidable harm is needed to enable healthcare systems to identify and learn from the most serious incidents and the factors amenable to intervention.
Most patient safety research has focused on hospital-based care settings resulting in a greater awareness of the frequency and causes of health care-associated errors, and the resulting burden to patients.4 Patient safety research in primary care has been slower,2 5 although the profile of patient safety in primary care was provided a platform by the WHO’s Safer Primary Care Expert Group (2012) and catalysed more recently by the US National Patient Safety Foundation’s call to look ‘beyond hospitals to the full care continuum’ and the Organisation for Economic Co-operation and Development’s assessment of the economic burden of unsafe primary and ambulatory care.6–8 The WHO’s Technical Series for Safer Primary Care, where world experts have explored the existing evidence base for primary care safety, highlighted that major evidence gaps exist and robust high-quality epidemiological studies are needed to definitively establish the burden of unsafe primary care.9 While harm from hospital-based care may be more visible, given the volume of patient consultations that occur in primary care, the aggregate burden of harm cannot be ignored.7
Our WHO-commissioned systematic review investigating the frequency and burden of harm in general practice concluded 2%–3% of primary care encounters involved a patient safety incident, and around 1 in 25 of those resulted in a significant harm outcome that has a substantial impact on a patient’s well-being.8 Included studies were notably heterogeneous in study design and definitions of outcome measures. None of the primary care studies in this, or our subsequent systematic review,10 reported the incidence of avoidable harm11 12 based on independent review of medical records, and few distinguished between minor and more significant harms.13 Also, we are aware of only one previous study that was large enough to identify substantial numbers of significant harms but did not report on these in detail.13 This means that based on the literature, it has not been possible to reliably quantify the overall burden of avoidable significant patient harm in primary care.
We have addressed this issue in the current study by undertaking a large retrospective case note review study using independent clinical reviewers to (1) estimate the incidence of avoidable significant harm in primary care in England; (2) quantify, describe and classify the patient safety incidents that result in avoidable significant harm (thus showing the top categories of avoidable harm) and (3) generate suggestions to mitigate risks of ameliorable factors that contributed to the incidents. Our study is different from other primary care studies because of its specific focus on identifying and understanding significant harm, and because it has estimated the incidence (rather than prevalence) of harm on the basis that this provides policy makers with a better idea of the potential burden of the problem. We have used a definition of avoidable harm based on a consensus study panel with general practitioners (GPs)14 using real cases of unsafe general practice from our earlier national-level analysis of patient safety incident reports.15
Methods
Our study protocol describes the methods we employed in detail,16 and an expanded version of our methods is in the online supplemental materials. Box 1 provides the definitions used in the study.
Supplemental material
Definitions used in our study
Significant harm
Our definition of significant harm was informed by the international classification of patient safety definitions of moderate harm, severe harm and death outcomes.44 The definition used was as follows:
‘A patient outcome is symptomatic, which required more intensive intervention than might otherwise have been required (eg, additional operative procedure) and resulted in an escalation of care (eg, hospital admission) or death. This caused a loss of function of at least one bodily organ, which may have been a temporary or permanent loss of its function’.
Avoidability
Our definition of avoidability was informed by our RAND/University of California Los Angeles appropriateness methods study14 to contextualise our definition of significant harm. The definition used was as follows:
‘A patient safety incident could have probably, or totally been avoided by the timely intervention of a health care professional in family practice (eg, investigations, treatment, safety netting) and / or an administrative process (eg, referrals, alerts in electronic health records, procedures for following up results) in accordance with accepted standards of evidence-based practice and / or clinical governance and / or the Bolam test’.45
Participants
We used a stratified random sampling approach to invite general practices to participate from three different areas of England. We undertook a retrospective case note review of an open cohort of all primary care patients registered with participating general practices (between 1 April 2015 and 31 March 2016) to identify cases of avoidable significant harm.
Recruitment and training of data collectors
GPs with at least 5 years’ experience in general practice were recruited to collect data from the participating practices and were provided with training.16
Sampling of patient records
We sampled patient records in three stages. In stage 1, we identified the total patient population of the practices at the start of the retrospective cohort (1 April 2015). In stage 2, we used electronic registry queries to identify patients at increased risk of significant health problems and/or avoidable significant harm (the ‘enhanced sample’). Drawing on suggestions made by the research commissioners, the literature on avoidable harm in primary care8 and our own experience of analysing reports of harm associated with primary care,15 we included patients who had died17 been admitted to secondary care,18 were resident in a care home,19 had multimorbidity15 or polypharmacy,20 21 had undergone an invasive procedure in general practice22 or had been certified unfit for work long term. In stage 3, one of the GP data collectors screened the electronic health record of each patient in the enhanced sample to identify any new significant health problems experienced by patients over the 12 months of the study (1 April 2015–31 March 2016). The GPs then undertook detailed retrospective reviews of the records of this final sample of patients to identify the extent to which errors in primary healthcare provision contributed to these problems.
For the purposes of sensitivity analysis (recognising that cases might have been missed by our sampling approach), the GP data collectors also undertook a detailed records review for the following:
2.5% random sample of the stage 1 population, not including patients identified for the stage 2 enhanced sample; each record was examined by a single GP reviewer.
10% random sample of the stage 2 enhanced sample; each record was examined by a second GP reviewer.
Identification of avoidable significant harm and factors associated with this
For those patients with significant health problems, the GP data collectors recorded whether they found any evidence of avoidable harm. If so, the GPs provided a detailed written account of the principal problem in the patient’s primary care that led to the significant health problem, a narrative describing the manner in which the significant health problem could have potentially been prevented within primary care, and a judgement on the avoidability of the significant health problem using a validated 6-point scale (see table 1).17 23 All cases were considered in detail by the study team, and the GP data collectors were asked to provide additional information if any clarification were needed. To ensure consistency, the study team made the final judgement, through consensus, in terms of the classification of avoidable significant harm.
Six-Point Avoidability Scale17 23
Data collection and coding
Each of the participating general practices was visited by an informatician from the study team who collected baseline data on the practice population and ran a computer search to identify patients for the enhanced sample and for the sensitivity analyses. Using encrypted tablet computers and a virtual private network connection, the GP data collectors entered anonymised data directly into a database on a secure server at Cardiff University. The nature of the avoidable harm was recorded by the GP data collectors using the comprehensive patient safety classification system developed in the Primary Care Patient Safety Classification study.24
Analysis
We estimated the incidence of significant harm that was considered at least probably avoidable (our primary outcome—avoidability score of 4 or more) and at least possibly avoidable (avoidability score 3 or more) accompanied by 95% CIs.16 We assessed inter-rater reliability of judgements made using the Cohen’s kappa statistic (with 95% CI).
Members of the study team then undertook a detailed analysis of the information provided on each case of potentially avoidable significant harm and included cases with at least ‘slight to modest’ (score or more) evidence of avoidability, as we judged that even in these cases there were important insights. We analysed the data recorded on the cases and examined the relationships between different types of incident and the factors that contributed to these incidents. As a result, we identified the most important factors contributing to avoidable significant harm.
Results
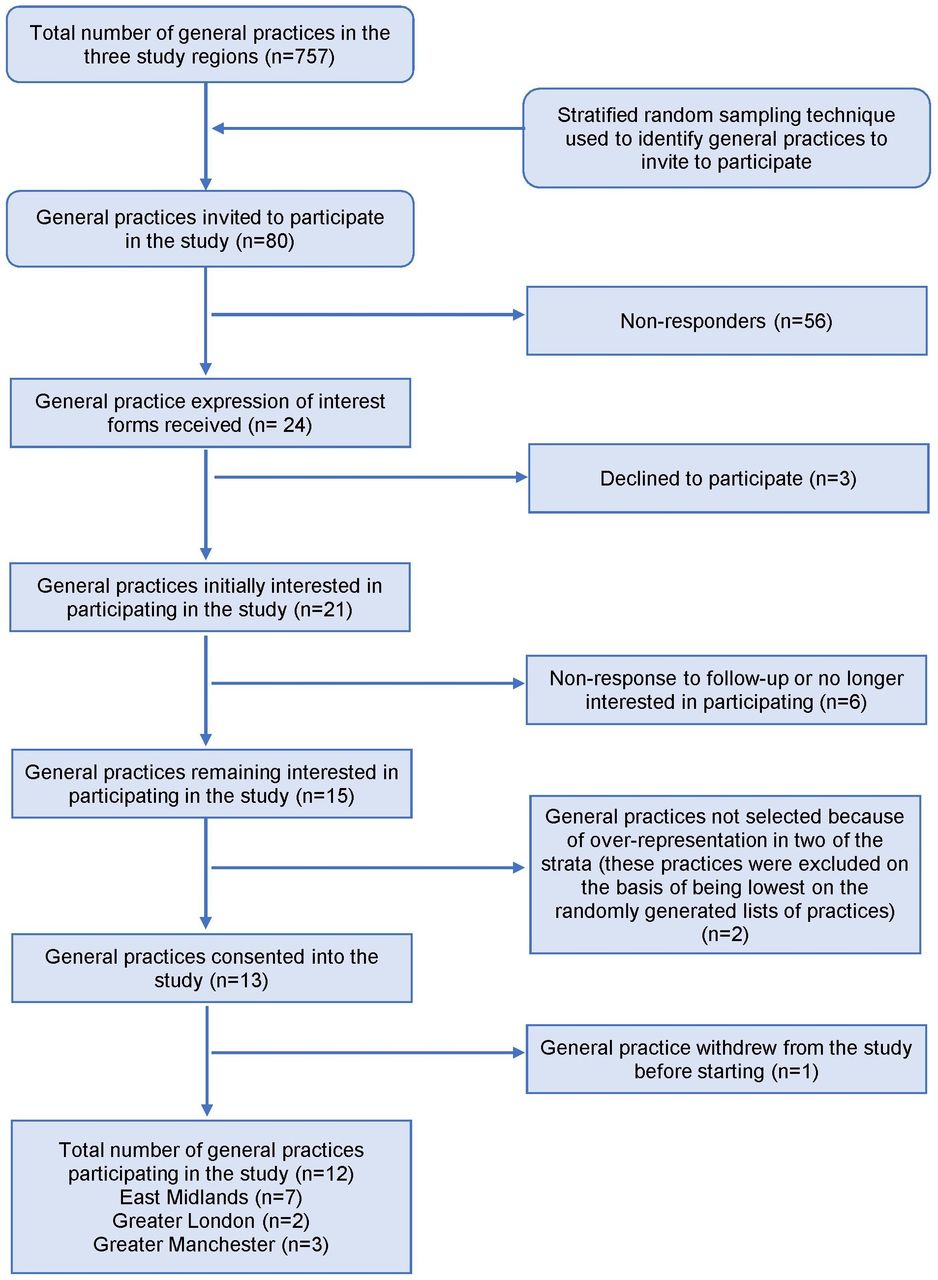
Twelve practices were recruited (as shown in figure 1) and table 2 shows their characteristics compared with national averages for England. The practices were similar to the English average in terms of list size, Index of Multiple Deprivation, and age and gender of patients, but had a higher percentage of non-white patients. Also, all the participating practices were rated overall as ‘good’ or ‘outstanding’ by the Care Quality Commission (CQC), whereas almost 12% of the practices in England received ‘inadequate’ or ‘requires improvement’ scores.

Flowchart showing how practices were recruited.
Characteristics and summary statistics of the 12 participating general practices compared with English averages
The total list size for the 12 general practices at the start date of the study cohort (1 April 2015) was 92 255 (Stage 1). The total number of patient-years of clinical data available for the 92 255 patients over the year of the cohort (1 April 2015–31 March 2016) was 89 779.
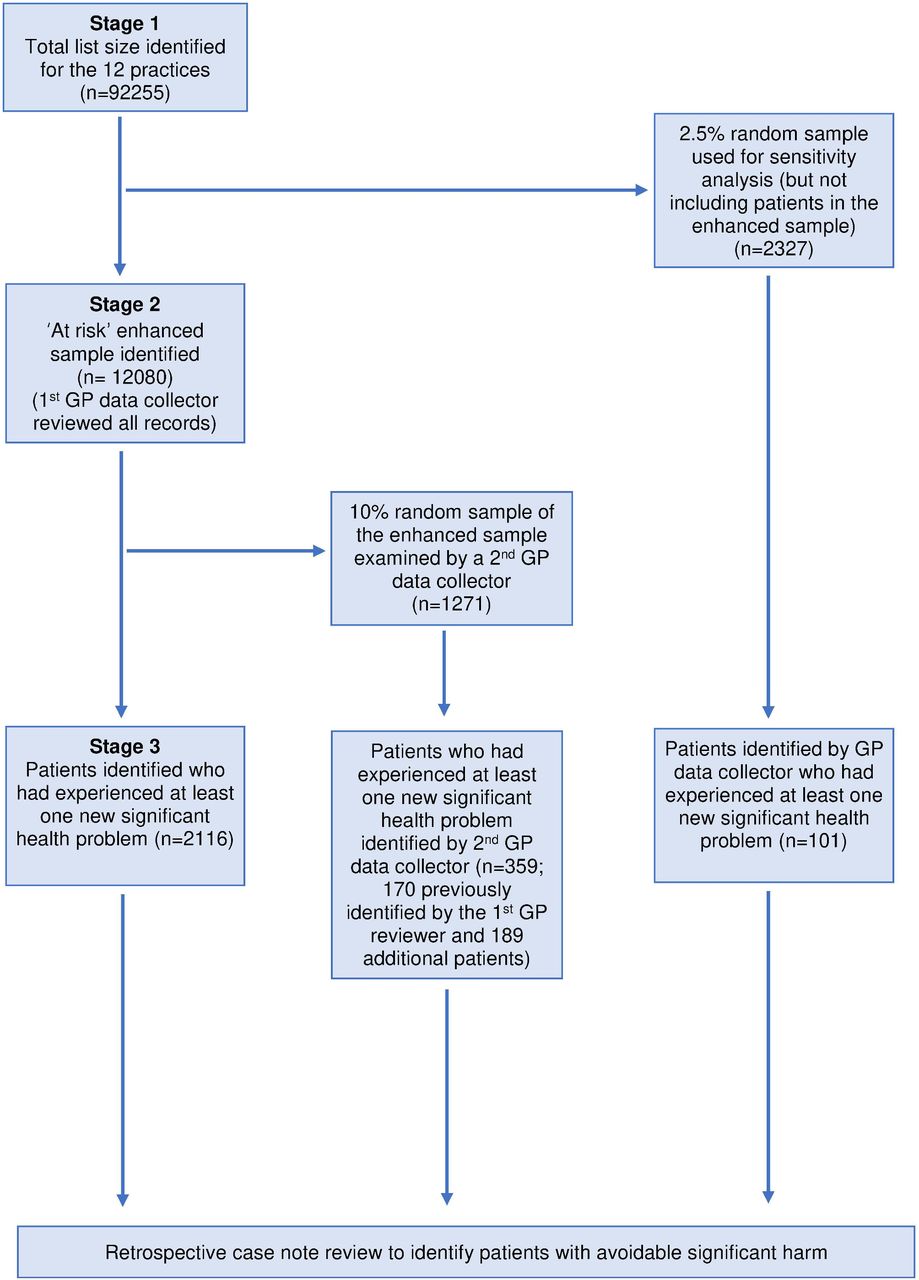
The flow of patient records through the study is shown in figure 2. The computer searches identified 12 080 patients (13.1%) for the enhanced sample (stage 2). Their records were all examined by at least one GP data collector (first GP data collector in figure 2), and 1271 (10.5% random sample) were examined independently by a second GP data collector. From the stage 1 population of 92 255, a random sample of 2327 (2.5%) patients (but not included in the enhanced sample) was examined by one of the GP data collectors.
{kind=link}
{kind=link}
Stages of the study and flow of patient records through the study. GP, general practitioner.
Based on the assessment of the GP data collector doing the first assessment on the enhanced sample, there were 2131 new significant health problems for 2116 patients between 1 April 2015 and 31 March 2016 (stage 3; see figure 2). For 2054 (96.4%) of the significant health problems, the GP data collector judged that the patient had received an adequate standard of care and therefore classified these cases as having ‘virtually no evidence of avoidability’.
For the remaining 77 (3.6%) cases, the first GP reviewer formally assessed avoidability and the distribution of avoidability scores, following moderation by the study team, is shown in table 3. A further 10 cases had ‘virtually no evidence of avoidability’, meaning that in total, 2064 (96.9%) of the 2131 significant health problems were considered unavoidable in primary care.
Avoidability of the 2131 new significant health problems identified by the first GP data collector
There were 32 cases (1.5%) of significant harm considered to be at least probably avoidable and 51 (2.4%) considered at least possibly avoidable. This translates into a rate of 35.6 per 100 000 patient-years (95% CI 23.3 to 48.0) for significant harm considered at least probably avoidable and 56.8 per 100 000 patient-years (95% CI 41.2 to 72.4) at least possibly avoidable.
Sensitivity analysis
The examination of the 2.5% sample of the patient population did not identify any additional cases of significant harm considered at least possibly avoidable. The examination of the 10% sample of the enhanced sample by a second GP reviewer identified two further cases of significant harm considered to be at least probably avoidable and four cases considered at least possibly avoidable, based on the final judgement of the study team. This means that had all the patient records in the enhanced sample been assessed independently by two GPs, there could have been an additional 20 cases considered at least probably avoidable, and 40 cases of significant harm considered at least possibly avoidable. In the sensitivity analysis, this translated into rates of 57.9 (95% CI 42.2 to 73.7) per 100 000 patient-years for significant harm considered at least probably avoidable, and 101.4 (95% CI 80.5 to 122.2) per 100 000 patient-years for significant harm considered at least possibly avoidable.
Inter-rater reliability
Where an assessment of avoidability was done, there was 77.0% agreement between GP data collectors and the study team about whether the case was considered at least possibly avoidable (Cohen’s kappa: 0.49, 95% CI 0.29 to 0.69). For the 10% sample of the enhanced sample, there was 71.5% agreement between the first and second GP reviewers that a patient had at least one significant health problem (kappa: 0.33, 95% CI 0.27 to 0.38), and where an avoidability assessment was done independently by two GP data collectors, there was a 67.6% agreement about whether the significant harm was considered at least possibly avoidable (kappa: 0.34, 95% CI: 0.02 to 0.66).
Analysis of the nature and causes of avoidable significant harm
For the detailed analysis of the nature and causes of avoidable significant harm, we included 74 cases involving 72 patients. The distribution of avoidability scores for these cases is shown in table 4.
Summary of cases judged by the study team to have significant harm with at least slight to modest evidence of avoidability
The distribution of different types of primary incidents for the 74 cases is shown in table 5, with problems with diagnosis accounting for 60.8%; medication-related problems for 25.7% and delayed referrals for 10.8% (the latter relating to situations where a clinician had decided that a referral was needed, but there was such a delay in the referral being made that the patient may have been harmed as a result). Examples of these incidents are shown in boxes 2 and 3. In relation to the 74 primary incidents, 114 underlying ‘contributory factors’ were identified, and these are shown in table 6. Patient factors accounted for 71.9%, with comorbidities or multimorbidities being the most important categories (24.6% of all contributory factors), while 17.5% of factors included issues such as not taking medicines as prescribed, problems with eliciting relevant information from patients or caregivers, not following medical advice and presenting with multiple issues in a single consultation. Factors such as multimorbidity and frailty contributed either through offering alternative explanations for symptoms or by presenting clinicians with multiple competing demands. Organisational factors accounted for 21.1% of contributory factors, while staff factors such as inadequate knowledge, skills or mistakes by healthcare professionals accounted for 7.0%. In 59 (79.7%) of the 74 cases, the significant harm could have been identified sooner (48 cases) or prevented (11 cases) if the GP had taken actions aligned with evidence-based guidelines (see examples in box 2).
Distribution of different types of primary incidents
Examples of avoidable significant harm
30-week delay in diagnosing throat cancer (avoidability rating: 5, strong evidence of avoidability)
A middle-aged patient attended the general practitioner (GP) with a hoarse voice and difficulty swallowing. He reported that his mouth felt like the time he had thrush, which required a referral to a gastroenterologist for an endoscopy, and it eventually settled with an antifungal medication. In the medical records, the GP described signs of oral thrush in the mouth and wrote, ‘if does not settle, consider oral treatment or referral back to gastroenterologist’. Over the next 19 weeks, the patient returned, with six visits to the original and different GPs, with on and off ‘red flag’ symptoms that were either improving or worsening or of varying intensity (hoarseness, swallowing issues, odd breathing pattern, difficulty talking and sensation of a lump in throat) and each time was given a course of antifungal medication. From week 12, the medical records describe ‘food getting stuck’. At week 15, a referral for endoscopy was made and the patient was seen 1 week later. At this point, the patient informed the gastroenterologist he was losing weight. No abnormalities were seen on endoscopy, and the patient was told to go back to his GP and have his hoarse voice investigated further (with the same advice in a letter to the GP). Four weeks later, the patient was seen by the GP and a non-urgent referral to ears, nose and throat (ENT) was made. At week 30, the patient was seen by ENT, and a rare type of neck cancer was diagnosed requiring chemotherapy.
Seven-year delay in diagnosis of prostate cancer (avoidability rating: 4; probably avoidable, more than 50:50, but close call)
An elderly patient with type 2 diabetes mellitus attended a nurse appointment stating that he was experiencing nocturnal frequency. It was suspected this was due to poorly controlled diabetes, and amendments to his medication regime were made. Six weeks later, the patient had a telephone consultation with the GP since he was concerned about weight loss, a loss of appetite, increased urinary frequency and night cramps. He was booked with the GP for a face-to-face consultation the following day. It was also noted he had a weight loss of 2–3 kg; he was urinating at least five to six times per night; and he felt nauseous. The GP felt the signs and symptoms were related to poorly controlled diabetes and arranged for the patient to be reviewed by the practice nurse. Over the next week, blood tests (glycosylated haemoglobin and ‘urea and electrolytes’ (U&E)) and urine analysis were undertaken, and his antihyperglycaemic medications were amended. The nurse followed up the patient up a few days later, where a further drop in weight was noted. The patient reported some improvement in symptoms since he was now getting up at night to pass urine four instead of six times. The nurse advised a follow-up appointment with the GP, which did not occur until 4 weeks later. At this time, the GP noted that 7 years previously the patient had a raised prostate-specific antigen (PSA). However, the patient had been unable to tolerate a biopsy for a definitive diagnosis, so 6 monthly PSA testing was advised; however, the patient did not have a follow-up PSA in the subsequent 7-year period. On noting this, the GP advised the patient to have a PSA test which was undertaken 3 weeks later. The PSA measured very high (>100 ng/mL). The patient had a GP appointment 1 week later when he was informed his PSA was raised. An urgent ‘suspected cancer’ referral was made. He was seen by a urologist the following week and diagnosed with localised prostate cancer requiring a transurethral resection of the prostate.
16-month delay in diagnosing non-insulin-dependent diabetes mellitus (avoidability rating: 3; possibly avoidable, less than 50-50, but close call)
An impaired fasting glucose was identified in a middle-aged patient and was followed up with a glucose tolerance test (GTT). The patient was seen by GP (A) soon after and was informed the GTT revealed an impaired glucose tolerance and was given dietary and lifestyle advice. The patient was told to have a repeat test 4 months later. The patient was seen 4 months later by a different GP (B); however, the focus of the consultation was on yellow sclerae and liver function tests (LFTs) were ordered. A test to assess diabetes was not requested. The patient presented 2 months later with weight loss, and GP (B) referred the patient for an endoscopy and a repeat LFT. A follow-up telephone call 1 month later occurred to discuss the LFTs with GP (B). Three months later, the patient presented to GP (B) with tiredness and fatigue. Again, blood tests were requested but did not include tests for diabetes. Six months later, a blood glucose was undertaken as part of an annual review, and following two fasting blood glucose tests 1 week apart, poorly controlled non-insulin-dependent diabetes mellitus was diagnosed.
Four-month delay in referral for an ischaemic limb (avoidability rating: 5, strong evidence of avoidability)
A patient in his early 60s stubbed his big toe 3 weeks prior to attending a nurse appointment at the general practice. The patient was known to have cardiovascular disease, including hypertension (prescribed two antihypertensives) and raised cholesterol (prescribed a statin). The nurse noted the toe was bruised, painful, red and had a foul odour. The patient was prescribed antibiotics for a presumed infection, and a referral was made to podiatry for removal of an associated ingrowing toenail. Four weeks later, a podiatrist was unable to detect a dorsalis pedis or posterior tibial pulse in the affected foot, and the patient was advised to see a GP urgently. The patient was reviewed by the GP, and a referral to a vascular surgeon was discussed but not made. Instead, a further consultation with the same GP in 4 weeks was agreed, with regular nursing reviews of wound healing in the interim. At the first follow-up nurse review 1 week later, the nurse noted that the toe was healing, but there were no pulses with the Doppler scan, and that the patient informed the nurse he needed to sleep with the foot outside the bed because it was so painful. The GP saw him 3 days later and decided to make a non-urgent vascular referral, but the letter was not sent to the vascular surgeons for 6 weeks. The patient was seen in a vascular clinic nearly 4 months after the podiatrist noted absent pulses and was informed that he had critical leg ischaemia and needed surgery. He underwent a right superficial femoral artery and posterior tibial artery (PTA) stent 4 weeks later. Some 9 months later, he required amputation of his big toe and second digit.
Long-term nephrotoxic medications in older adults
We observed two cases where patients with known reduced kidney function were receiving long-term potentially nephrotoxic drugs. One of the patients was prescribed naproxen ‘as required’ for gout but received a two times per day monthly supply for >12 months while concurrently receiving long-term nitrofurantoin. A hospital admission for acute-on-chronic kidney injury was required (avoidability rating: 5, strong evidence of avoidability).
Another patient was taking lithium and should have had 3 monthly U&E blood tests to monitor their kidney function. This did not happen for 15 months, and the patient was admitted with acute kidney injury (avoidability rating: 4; probably avoidable, more than 50:50, but close call).
Underlying incidents resulting in delayed diagnoses (history taking, examination, investigation, communication and referral)
Incomplete history taking (one case), for example, not enquiring about red flags and not documenting salient negatives, inaccurate medical records (two cases), and inadequate documentation of care delivered (one case).
Absent or delayed physical examination (five cases), for example, advising patient to book another visit to undertake a pelvic examination.
Not ordering correct investigations (three cases), for example, no follow-up or investigations ordered for an older adult with a 3-week history of diarrhoea with blood and mucus; the patient eventually required an emergency admission, and Crohn’s disease was diagnosed.
Failing to order a necessary investigation (one case), for example, not testing for diabetes mellitus when presenting with lower urinary tract symptoms.
Inappropriate responses to laboratory (three cases) or imaging (one case) investigations, for example, (1) not recognising the cut-off for diagnosing type 2 diabetes, (2) not arranging a follow-up chest X-ray (that had been advised by a radiologist) in a patient with an opacity seen on serial radiographs (this resulted in a delay in referral to respiratory medicine for an eventual diagnosis of lung cancer).
Transfer of information about the patient, which included delays in the communication being sent (two cases) or not sent at all by secondary care (one case), or a communication received but not actioned in primary care (three cases).
Incorrect advice being given to the patient (one case), for example, patient with insulin-dependent diabetes not given information about how to prepare for an endoscopy and the general practitioner did not inform secondary care the patient was diabetic.
Delayed referral (seven cases), referral not made (one case) or referral sent to the wrong location.
Distribution of contributory factors
These 74 cases involved 115 healthcare professionals (81 (70.4%) GPs and 10 (8.7%) practice nurses), and only 4 of these (3.5%) were clearly identifiable as being from outside the participating general practices (community nurse, community optometrist, community physiotherapist and community psychiatric nurse).
Discussion
Principal findings
The estimated incidence of significant harm in English primary care considered at least ‘probably’ avoidable is between 35.6 and 57.9 per 100 000 patient-years (the latter figure being based on sensitivity analysis). Extrapolating our findings to the English population of 55.6 million (mid-year 2017), we found that there are likely to be between 19 800 and 32 200 cases of ‘probably avoidable’ significant harm to patients each year.
The three major sources of significant avoidable harm in general practice were diagnostic error (60.8% of the avoidable incidents), medication incidents (25.7%) and delayed referrals (10.8%). In 79.7% of cases, the significant harm could have been identified sooner or prevented if the GP had taken actions aligned with evidence-based guidelines. The study identified a mix of organisational, clinician and patient contributory factors associated with the avoidable incidents. The majority of these were patient factors (71.9% of the total contributory factors identified), including multimorbidity, old age and complexity arising from pathophysiological factors such as frailty. Most of these factors are not ameliorable but highlight the challenges that healthcare professionals face when trying to avoid patients coming to harm. Of the organisational factors, problems relating to continuity and coordination of care (between providers and within primary care) were most important (14.1% of the total). For example, the patient did not experience a ‘seamless service’ due to failures in coordination and sharing of information between different providers across the health and social care system, disconnect between multiple members of the primary care in the same practice and lack of care coordination as a patient transitions from secondary back to primary care. Mitigating risk for future patients could be achieved through targeting the organisational structures and processes underpinning the most frequent contributing factors.
Strengths and limitations of the study
This is one of the most comprehensive studies of avoidable harm in primary care,8 10 and one of only two records review studies we are aware of that is large enough to report on substantial numbers of significant harms.13 It is the only study of which we are aware that has reported the incidence of avoidable harm based on independent review of primary care clinical records. In terms of other potential methods of investigation, independent retrospective case note review has significant advantages over incident reports, which are more at risk of selection bias and are not well suited to accurately estimating the incidence of avoidable harm. It also has advantages over database studies because detailed examination is required of the healthcare records (including hospital correspondence), which is not possible through clinical databases. One major limitation of case note review is the onerous task of searching for and identifying important information to build a narrative, based on what is explicitly stated or from what is absent based on the clinician’s knowledge of the relevant evidence-based guidelines.
We used a stratified random sampling approach to recruit 12 general practices from three geographically different regions of England, and the independent GPs involved in data collection were experienced and were given thorough training. We used a validated method for judging the avoidability of harm14 and a comprehensive validated system for classifying the underlying causes of patient harm.15 Our methodological approach used the recursive model of incident analysis and permitted us to capture the series of ‘contributing incidents’ that led to the final ‘principal incident’ prior to the patient experiencing a harmful outcome.25 This meant we could provide the most robust and comprehensive assessment of the patient safety incidents implicated in significant avoidable harm outcomes, as well as consider the apparent underlying events when formulating our recommendations to mitigate future risk to patients.
Only a quarter of the general practices in the stratified random sample agreed to participate, and this is a limitation from an epidemiological perspective. The most common reason cited for not participating was lack of time. Although the characteristics of the practices recruited were similar to those in England in most respects, none of the study practices received an overall CQC rating of ‘inadequate’ or ‘requires improvement’, whereas 2.6% and 9.1% (respectively) of all English practices received these ratings. If CQC ratings are associated with patient safety, then our study may underestimate the overall incidence of avoidable significant harm in English general practices. Our inter-rater reliability assessments showed that there was moderate agreement between the GPs in their identification of patients with significant health problems, and their judgements as to whether a patient had experienced avoidable significant harm. Even with our sensitivity analysis, the upper limit of our estimates of the incidence of avoidable significant harm may be an underestimate. This highlights the uncertainties of estimates of frequency of harm originating from case note reviews that rely on clinical judgement. It suggests that our study could have missed some cases of avoidable significant harm but could also have included cases that others might not consider to be ‘significant’ or ‘avoidable’.
Through our enhanced sample, we successfully identified patients most likely to have avoidable significant harm, but the criteria we used might be difficult to replicate in other countries. We did, however, manage to identify these patients through electronic medical records, and so a similar approach should be possible in countries with comprehensive primary care electronic records. Our study was not designed to detect near misses.
Comparison with other studies
We recognise from our previous systematic reviews8 10 that comparing studies of avoidable harm is difficult because of different study designs and different ways of applying definitions of avoidable harm. One key difference between our study and almost all previous studies is that we report the incidence of avoidable harm rather than the prevalence (per consultation). Our approach allows for a clearer estimate of the public health burden of avoidable harm while also recognising that some harms, especially in a primary care setting, may occur over several consultations (eg, delayed diagnosis). Also, we have focused specifically on significant harm (such as a clinically important delay in cancer diagnosis) to ensure that our findings reflect a health burden that is unquestionably of importance to patients, the public, clinicians and policy makers.
The only study we are aware of that was of a similar large size to ours, while also reporting on severity, was from a convenience sample of 48 health centres in Spain with health professionals reporting any incidents causing harm.13 From 96 047 consultations, 773 harms were detected with 46 of these considered ‘severe’. Of all the harms, 64.3% were considered preventable, and applying this percentage to the severe harms suggests a prevalence of 30.8 severe harms per 100 000 consultations. It is not possible to directly compare this with the incidence figures from our study (where the same harm may have been apparent across several consultations over the course of the 12 months), but the overall rates of significant harm are probably not widely dissimilar.
There is considerable variation in studies reporting categories of avoidable harm as well as contributory factors. Nevertheless, our findings are in keeping with a systematic review that found that diagnostic errors were among the most important causes of avoidable harm,10 and a review of the global burden of diagnostic errors in primary care,26 while the systematic review10 (and other studies) has highlighted the importance of prescribing errors.13 In relation to diagnostic delay in cancer, a recent study has highlighted that in almost half of the cases, this is attributable to primary care,27 with problems with clinical appraisal of the patient and referral being particularly important. Our study has specifically highlighted the importance of delays in making a referral,15 23 and this has been highlighted as an important problem by the Institute for Healthcare Improvement.28 In comparison with other studies, ours is unusual in reporting such a high level of patient factors contributing to patient harm. While many of these cannot be considered the reason for the harm being avoidable, the findings suggest that factors such as multimorbidity, frailty and complex presentations may make it more difficult for clinicians to make timely and accurate diagnosis and avoid medication errors. In relation to contributory factors that are avoidable, our findings are in keeping with other studies that have highlighted organisational issues and communication problems.8 12 29
Implications for clinicians and policy makers
This study has estimated the incidence of significant harm in English primary care considered at least probably avoidable, which translates to three to four cases per year for an average general practice of 8000 patients. Efforts to make improvements should focus on addressing the structures and processes underpinning the identified patient, clinician and organisational contributing factors. For example, better organisation of key systems (eg, referrals, test result management, identifying non-adherence) and related administration could have prevented most incidents. Some of the earliest patient safety studies carried out in primary care over two decades ago pointed to administrative failures, such as the mismanagement of test results, as the root cause of the the most common incidents concerning diagnosis and medication,30–32 and an Australian study concluded about 70% of incidents were related to processes of providing healthcare, rather than gaps in the knowledge and skills of health professionals.11 The current study provides considerable insights into the ameliorable contributory factors associated with avoidable significant harm in primary care, which in turn have generated the following suggestions for improvement.
More effective implementation of existing information technology solutions could ensure that planned action such as referrals take place in a timely way.26 Enhanced team coordination and communication could ensure that patients are seen (or have necessary investigations) or that they are recalled for follow-up investigations or assessment when needed. Currently, it is largely down to individual primary care teams and individual healthcare practitioners to develop their own strategies. Without stifling innovation, however, it might be helpful to model ‘what best practice looks like’ in relation to preventing patients from coming to harm. Interventions like the ‘QRISK3–2018’ algorithm to calculate a person’s risk of developing a ‘heart attack’ or stroke are now commonly integrated into electronic health record systems and used by clinicians to explain and manage risk and support patient decision-making.33 In a similar way, the factors implicated in patient safety incidents that we have identified might be considered as signals for future algorithms for development and validation, either to flag up patients for timely clinical review to mitigate current risk levels or to proactively detect risks of future unsafe care.
Our study suggests that lack of continuity of care may contribute to avoidable significant harm in some cases.34 Recent systematic reviews suggest that low continuity of care is associated with a higher risk of mortality across different healthcare settings35 and specifically in general practice.36 In some cases in our study, follow-up by the same primary healthcare practitioner could have been helpful to enable earlier recognition of the progression of a serious health problem. In other cases, better ‘informational continuity’37 could have helped to ensure that the assessment and suggested follow-up plans from a previous consultation better informed the next consultation. This should be facilitated by electronic health records, but we found several examples where recommendations from one consultation were not acted on in a subsequent consultation involving a different healthcare practitioner. Nevertheless, high levels of personal continuity may not always be best for patients. A recent qualitative study showed a mixed picture in terms of patients’ perceptions of whether personal continuity improved safety, or not,38 while a cross-sectional ecological study found that general practices that appeared to have high levels of personal continuity did fewer urgent referrals39; this does not necessary mean they were less safe, but it is a potential cause for concern.
Some of the cases of avoidable significant harm in our study were associated with GPs having too many problems to deal with adequately in a single consultation, with significant health problems not detected early enough because of lack of effective and timely clinical history taking, examination or investigation. Some of the contributory factors associated with patient behaviours may have resulted from their concerns being unrecognised or unresolved, as highlighted in a study of missed opportunities in cancer diagnosis.40 When such incidents occur in general practice, it is essential that practice teams know how to generate learning from the incident, including how to identify vulnerabilities in their existing structures and processes, and feel confident to plan and test changes that could achieve improved outcomes for future patients.41 The introduction of quality improvement domains into 2019/2020 Quality and Outcomes Framework by NHS England represents a promising commitment for supporting practices to learn about and develop their approach to systems improvement42 as does the 2019 NHS Patient Safety Strategy.43
Conclusion
There is likely to be a substantial burden of avoidable significant harm attributable to primary care in England with diagnostic error accounting for most harms, followed by medication error and delays in making a referral once a referral decision had been made. Based on the contributory factors we found, improvements could be made through more effective implementation of existing information technology, enhanced team coordination and communication, and greater personal and informational continuity of care.
Data availability statement
Data are available upon reasonable request. Anonymised summary data extracted from patient records regarding the avoidable harms detected in this study will be available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The study had NHS research ethics committee approval and was granted a favourable opinion by the East Midlands Nottingham 2 Research Ethics Committee on 15 January 2016 (reference: 15/EM/0411) and Confidentiality Advisory Group approval for access to medical records without consent under section 251 of the NHS Act 2006 on 11 April 2016 (reference: 15/CAG/0182). Research and development approval was obtained for the Clinical Commissioning Groups, where the study occurred.
Acknowledgments
We thank Dr Christine Johnson and others who helped us to recruit the general practitioners (GPs) for the retrospective case note review. We also thank all of the practices that willingly took part in the retrospective case note review study; they were all very welcoming to the GPs who undertook the data collection, and provided space, access to computers and support to allow them to undertake their work. We are particularly indebted to the GPs who did the data collection as they were highly committed to the study, and many of them went the extra mile in terms of fitting in extra data collection sessions to enable us to complete the study within the time frame agreed. In particular, we thank Dr Richard Thomas for providing most of the training for the GPs. We thank Ed Longridge for running most of the baseline computer searches in the practices and for collecting data to allow us to calculate ‘patient-years’ (the denominator for our study). We thank Dr Sukhmeet Panesar for advice at the development stage of the project, particularly concerning literature on avoidable harm. We are extremely grateful to the members of our external advisory group (chaired by Professor Charles Vincent and including Professor Susan Dovey, Dr Frances Healey (funder representative) and Professor Gordon Schiff), who gave very helpful advice throughout the study and were particularly helpful in terms of the interpretation of our findings. We also thank members of the East Midlands Academic Health Science Network PPI Senate and the Greater Manchester Patient Safety Translational Research Centre and Health Innovation Manchester Patient Experience Group for reviewing the findings and providing helpful comments from the perspective of members of the public.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @tonyavery1
Contributors All authors made a substantial contribution to the conception or design of the work; or the acquisition, analysis or interpretation of data for the work. Specifically, AJA, ACh, AC-S, AD, AE, AS, DMA, HPE, MJB, SMC, SA and SR conceived the study; AJA, ACh, AC-S, AD, AE, AS, DMA, HPE, JL, MJB, PS, RM, SMC, SA and SR designed the study; AJA, AC-S, CS, DMA, SMC and SR recruited the general practitioner (GP) reviewers and practices; AJA, AC-S, AE, CS and HPE trained the GP reviewers; AJA, ACh, ACo, AC-S, AD, AE, CS, DMA, HPE, JL, MJB, SMC, SH and SR designed the data collection process; AJA, ACo, AC-S, AE, BB, HW and SH processed the data; AJA, ACo, AC-S, AE, HW, and SH contributed to team judgements of avoidability of harm; AJA, ACo, AC-S, AE, BB and HW analysed the data, and all authors were involved in interpretation of the data; AJA, AC-S, AE, AS, BB, CS, DMA and SMC drafted the paper and all authors revised it critically for important intellectual content; all authors gave the final approval of the version to be published and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. AJA is the guarantor for the paper and accepts full responsibility for the work and/or the conduct of the study, had access to the data and controlled the decision to publish.
Funding This paper is based on independent research commissioned and funded by the National Institute for Health Research (NIHR) Policy Research Programme (‘Understanding the Nature and Frequency of Avoidable Harm in Primary Care’, Ref: PR-R11-0914-11001). General practitioner time was funded by the NIHR Greater Manchester Patient Safety Translational Research Centre (NIHR Greater Manchester PSTRC).
Disclaimer The views expressed in the publication are those of the authors and not necessarily those of the National Institute for Health Research or the Department of Health and Social Care.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.