Article Text

Abstract
Background: Tachycardia during anaesthesia is a common event. In most cases the cause is easily identified and the problem promptly resolved. However, in some the cause may be rare or obscure. Under such circumstances, attempting to initiate appropriate supportive therapy and to consider a large differential diagnosis in a comprehensive manner may lead to delays which can put a patient at risk.
Objectives: To examine the role of a previously described core algorithm “COVER ABCD–A SWIFT CHECK”, supplemented by a specific sub-algorithm for tachycardia, in the management of tachycardia developing in association with anaesthesia.
Methods: The potential performance of this structured approach for each of the relevant incidents among the first 4000 reported to the Australian Incident Monitoring Study (AIMS) was compared with the actual management as reported by the anaesthetists involved.
Results: There were 145 causative events identified in 123 reports of tachycardia during anaesthesia which were extracted and studied from the first 4000 incidents reported to AIMS. Subgroups were identified based on blood pressure at the time of presentation. Of the 145 causes, tachycardia was associated with hypotension (33%), normotension (27%), hypertension (26%), and cardiac arrest (17%). For simplicity it is recommended that other cardiovascular sub-algorithms are followed when the blood pressure is also abnormal. This includes cardiac arrest and hypotension. In hypotensive states the tachycardia sub-algorithm should be followed until the cardiac rhythm is diagnosed. Sinus tachycardia and hypotension should be managed as hypotension. It was considered that, correctly applied, the core algorithm COVER would have diagnosed 35% of cases and led to resolution in 70% of these. It was estimated that completion of COVER followed by the sub-algorithm for tachycardia would have led to earlier recognition of the problem and/or better management in four cases when compared with actual management reported.
Conclusion: Tachycardia during anaesthesia is frequently associated with a simultaneous change in other monitored vital signs. The differential diagnosis is large. Addressing it in a comprehensive fashion requires a structured approach. A specific sub-algorithm treatment for tachycardia based on the associated blood pressure and on the prevailing heart rhythm in the case of hypotension offers a systematic guide which complements the benefits obtained by employing the core algorithm COVER ABCD.
- tachycardia
- tachydysrhythmia
- crisis management
- anaesthesia complications
Statistics from Altmetric.com
Tachycardia during the course of an anaesthetic is a common event. The clinical significance of tachycardia will in part be determined by the blood pressure and cardiac rhythm of the patient at the time. This may vary from a hypotensive to a hypertensive crisis. Tachycardia and hypertension have been shown to be independently associated with a poor outcome after prolonged procedures.1 Hypotension may degenerate into a cardiac arrest or the patient may be pulseless from the outset.2
The scope of the problem is large when these situations are considered collectively. Problems are commonly resolved because the anaesthetist recognises patterns learnt from previous experiences. The potential exists, however, for the problem to lie outside the repertoire of the anaesthetist, particularly if they are inexperienced, the cause is rare, or the tachycardia is associated with an unusual phenomenon. Addressing the problem becomes increasingly difficult when there are simultaneous abnormalities in other systems. Attempting to initiate appropriate supportive therapy and consider a large differential diagnosis in a comprehensive manner may involve unacceptable delays in a crisis. It was therefore decided to examine the role of a structured approach to the problem of tachycardia associated with anaesthesia.
In 1993 a “core” crisis management algorithm represented by the mnemonic COVER ABCD–A SWIFT CHECK (the AB precedes COVER for the non-intubated patient) was proposed as the basis for a systematic approach to any crisis during anaesthesia where it is not immediately obvious what should be done or where actions taken have failed to remedy the situation.3 This was validated against the first 2000 incidents reported to the Australian Incident Monitoring Study (AIMS). AIMS is an ongoing study which involves the voluntary anonymous reporting of any unintended incident which reduced or could have reduced the safety margin for the patient.4
It was concluded that, if this core algorithm had been correctly applied, a functional diagnosis would have been reached within 40–60 seconds in 99% of applicable incidents, and the learned sequence of actions recommended by the COVER portion would have led to appropriate steps being taken to handle 60% of problems relevant to this portion of the algorithm.3 However, this study also showed that the 40% of problems represented by the remainder of the algorithm ABCD–A SWIFT CHECK were not always promptly diagnosed or appropriately managed.3–5 It was decided that it would be useful for these remaining problems to develop a set of sub-algorithms in an easy-to-use crisis management manual.6 This study reports on the place of the COVER ABCD–A SWIFT CHECK algorithm in the diagnosis and initial management of tachycardia, provides an outline of a specific crisis management sub-algorithm for tachycardia during anaesthesia, and provides an indication of the potential value of using this structured approach.
METHODS
Of the first 4000 incidents reported to AIMS, those which made reference to tachycardia or tachydysrhythmia were extracted and analysed with respect to the following criteria: surgical group, anaesthetic technique, patient’s ASA status, phase of anaesthesia at the time of presentation, presenting features (cardiac rhythm, blood pressure, oxygen saturation and other associated vital signs), the presumed precipitating cause, management, and outcome. The COVER ABCD–A SWIFT CHECK algorithm, described elsewhere in this series of articles,6 was applied to each report to determine the stages at which the problem might have been diagnosed and to confirm that activating the COVER portion would have led to appropriate initial steps being taken. As tachycardia is not adequately dealt with by this algorithm, a specific sub-algorithm for tachycardia was developed (fig 1) and its putative effectiveness was tested against the reports. How this was done is described elsewhere in this series of articles.6 The potential value of this structured approach—that is, the application of COVER ABCD–A SWIFT CHECK to the diagnosis and initial management of the problem followed by the application of the tachycardia sub-algorithm—was assessed in the light of the AIMS reports by comparing its potential effectiveness for each incident with that of the actual management, as recorded in each report. It was also of interest to evaluate if delays in diagnosis and overall outcome could be improved with the application of the sub-algorithm.

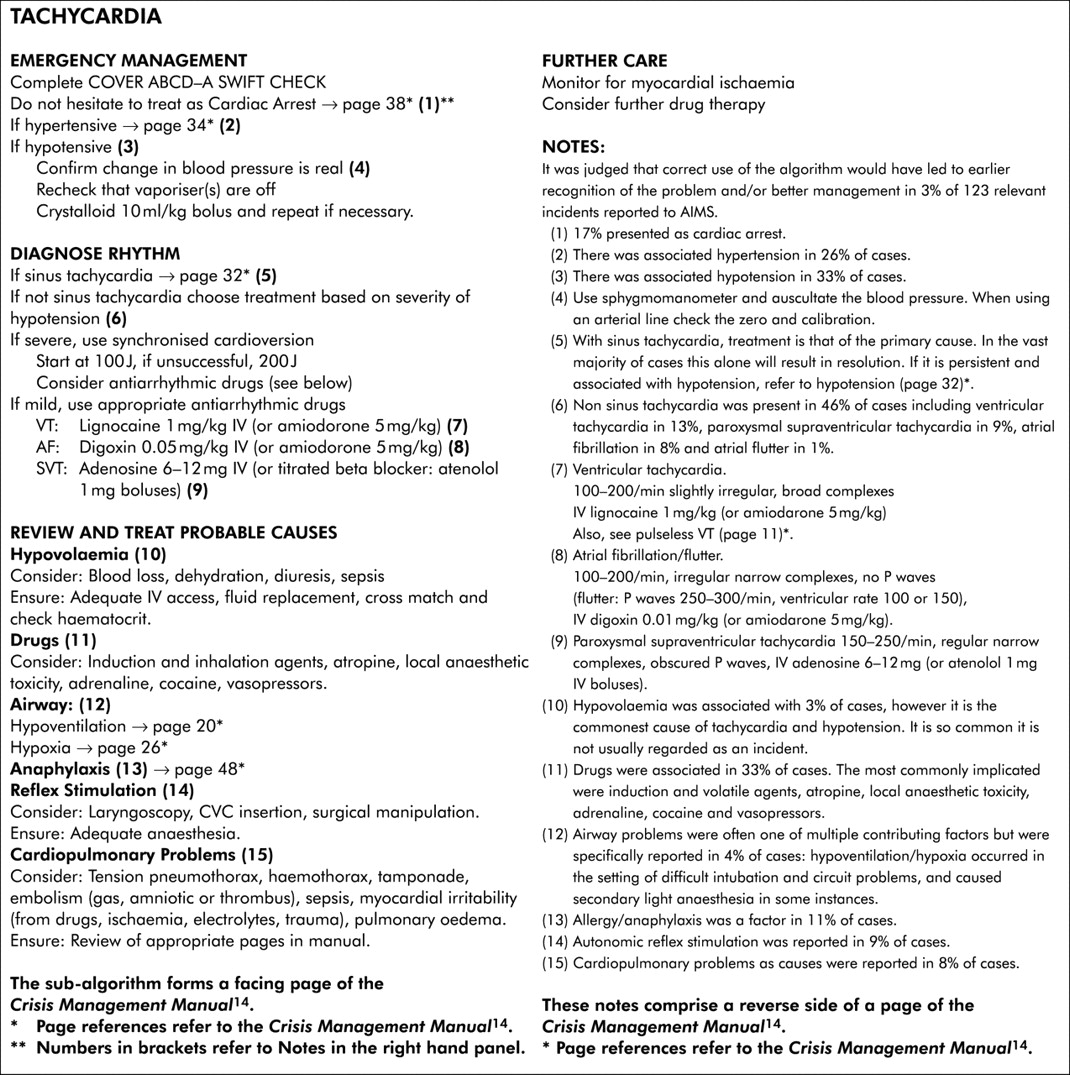{kind=link}
Tachycardia.
RESULTS
There were 123 reports which contained the word “tachycardia” or “tachydysrhythmia”. These occurred across a range of surgical groups (table 1).
Surgical groups reported in cases of tachycardia
The patients’ ASA grades were available in 117 cases (table 2).
ASA rating
Tachycardia was reported during all phases of anaesthesia but occurred most commonly at induction and in the maintenance period (table 3).
Phase of anaesthesia at time of detection of tachycardia
Aetiology and diagnosis
The contributing causes for all reported cases of tachycardia and for the subgroups are presented in table 4. A total of 145 causative events were identified within the 123 reports. In this series, drugs are the dominating associated cause of tachycardia. The haemodynamic status of the patient at the time that tachycardia was detected included cardiac arrest (17%), hypotension (33%), normotension (27%), and hypertension (26%).
Causes of tachycardia expressed as percentage of total causes
Cardiac arrest was reported in 24 events (17%). The prevailing rhythm was sinus pulseless electrical activity (PEA), formerly known as electromechanical dissociation (four cases), pulseless ventricular tachycardia (VT; n = 9), and ventricular fibrillation (VF; n = 5). In one case a bizarre undiagnosable rhythm was present initially which degenerated into VT and VF and then asystole. One episode of VT could not be clearly distinguished from supraventricular tachycardia (SVT) on the monitor. In four cases VT degenerated into VF.
Most specified ASA grades were represented in the cardiac arrest group: ASA IV (n = 4), ASA III (n = 6), ASA II (n = 2), ASA I (n = 8), not stated (n = 4). Cardiac arrests occurring in ASA I patients were caused by anaphylaxis (n = 3, PEA), hypoxaemia (n = 1, VT-VF), and hypovolaemia (n = 1, VF). Two ASA I patients experienced sudden VT in association with intravenous induction agents and another during handling of the myocardium during thoracic surgery. None of these patients died.
There appears to be a higher incidence of allergy and cardiopulmonary events as causes among the reported cases of tachycardia (table 4). In 10 of the reports the patient was initially hypotensive and subsequently deteriorated to cardiac arrest. A pulseless state was reported from the outset to the remainder. No differences in aetiology were evident from an inspection of the reports. This supports the use of the cardiac arrest algorithm in every case of cardiac arrest, irrespective of how it presents.
Hypotension occurred in association with tachycardia in 48 cases (33%, table 4). Again there is a higher representation of allergy and cardiopulmonary events, but this is not the case for hypovolaemia as might be expected. The causes were also compared between sinus and non-sinus tachycardia. All cases of allergy were associated with sinus tachycardia. No other patterns were apparent; however, the number of cases was small. As a general observation, the profile of causes for hypotension and tachycardia occurring together is significantly different from either hypotension or tachycardia overall to warrant its own subgrouping.
Hypertension was reported in 37 cases (26%). The majority of cases involved sinus tachycardia. The remaining seven cases were associated with non-sinus tachydysrhythmias: VT (n = 1), SVT (n = 2), atrial fibrillation (n = 1), bigeminy (n = 2), and ventricular ectopy (n = 1). There was no apparent difference in causes with respect to rhythm.
There are notable differences in the causes in this group compared with hypotension. Light anaesthesia was the attributed cause in six cases. This included frank awareness and perceived pain. Two of these involved the inadvertent administration of muscle relaxant and one involved an empty vaporiser. Three cases were associated with hypercarbia secondary to rebreathing resulting from malfunction of the expiratory unidirectional valve or soda lime exhaustion. Drugs were implicated in 11 cases and again the profile of drugs differs considerably from hypotension (table 5). Four of these were associated with syringe or ampoule errors, three of which involved adrenaline.
Drug related causes of tachycardia expressed as the number of cases in which the drug contributed to tachycardia within various presentation groups
Tachycardia occurred without a change in blood pressure in 39 cases (27%). The causes described in this category represented those already observed in hypotension and hypertension (tables 4 and 5).
An apparent abnormality of gas exchange as evidenced by desaturation on pulse oximetry, inadequate ventilation, obstruction, or dyspnoea was described in 30 reports (24%). Evaluation of these cases showed that desaturation may represent an artefact on pulse oximetry secondary to diminished peripheral perfusion,7 but this could not be distinguished at the time of detection of tachycardia from those cases in which real abnormalities of gas exchange existed.
Outcomes
The outcome of patients experiencing tachycardia during anaesthesia was studied. Poor outcomes are given in table 6. Thirty nine cases were considered to have had a poor outcome because they were not resolved by the completion of the normal recovery period. Three cases resulted in death on the table or in the postoperative period. This contrasts with previous reviews of death resulting from cardiac arrest under anaesthesia which described a 50% mortality rate.8 Factors contributing to a poor outcome were considered in terms of ASA rating, rhythm, cause and management.
Poor outcome associated with tachycardia
A poor outcome was more likely to occur if tachycardia was associated with a pulseless state. All deaths occurred in this group. It appeared otherwise independent of blood pressure. Similarly, no strong relationship could be found with ASA rating (table 7). There were no cases in which it was felt that outcome could have been improved.
Poor outcome related to ASA grade in tachycardia (number of cases)
Verification of the sub-algorithm
When COVER ABCD–A SWIFT CHECK was applied to each report it was considered that the problem would have been detected in all cases either at the C1 stage of COVER or at C of ABCD; 40 cases (33%) from the database would have been diagnosed and, of these, 28 (70%) also resolved by application of the core algorithm COVER. The majority of these dealt with vaporiser incidents V2 (n = 1), circuit problems V1 (n = 7), possible artefacts from monitors R1 (n = 3), equipment malfunction or errors with non-anaesthetic drugs R2 (n = 25). The remaining cases required either completion of the sub-algorithm for tachycardia or pursuit of the sub-algorithms for the specific aetiological incidents dealt with under ABCD–A SWIFT CHECK. It was considered that carrying out the recommendations shown in fig 1 (the sub-algorithm) would have constituted appropriate management in all cases.
When the effectiveness of the structured approach represented by COVER ABCD–A SWIFT CHECK algorithm and the special sub-algorithm for tachycardia was compared with that of actual management as documented by each of the reports, it was considered that, if properly applied, the structured approach recommended would have led to quicker and or better resolution of the problem in four cases. There was a significant delay in diagnosis in three of these and inappropriate management in one.
DISCUSSION
The specific sub-algorithm for tachycardia is shown in fig 1. The hallmarks of the sub-algorithm are early clarification of the haemodynamic status and context specific treatment.
Tachycardia is frequently associated with abnormalities of blood pressure and separate sub-algorithms have been developed for these. Following multiple sub-algorithms may generate unnecessary workload and delays. The data were inspected for patterns which may provide guidance in this event and the following recommendations are made:
Key messages
-
From the first 4000 incidents reported to AIMS, 123 reports of tachycardia identifying 145 causes were extracted and studied.
-
The predominant surgical groups implicated were orthopaedics, general surgery, ENT surgery, and cardiothoracic surgery.
-
Most tachycardia was detected during the induction and maintenance phases of anaesthesia. At detection, 20% of patients were in cardiac arrest.
-
There were no deaths among the cardiac arrest patients. All ASA grades were represented. Three such ASA I cases had pulseless electrical activity caused by anaphylaxis.
-
The data in this series support the use of the cardiac arrest algorithm in every case of cardiac arrest, irrespective of how it presents.
-
The causes of tachycardia associated with hypotension and those associated with hypertension were notably different (for example, the drug profiles involved).
-
Light anaesthesia (including frank awareness) occurred in six of the tachycardia cases associated with hypertension.
-
Poor outcomes were reported in 39 cases (32%), with predominance among the higher ASA grades.
-
While 23% of the cases would have been fully resolved using the core algorithm, it was considered that the remaining 77% required either the specific tachycardia sub-algorithm or the application of other sub-algorithms in this series, as indicated by the aetiologies revealed by the core algorithm.
If the patient is:
-
Pulseless: follow the sub-algorithm for cardiac arrest. A detailed discussion of the management of cardiac arrest is beyond the scope of this paper but can be found in other reviews2,9 and guidelines.10,11
-
Hypertensive: follow the sub-algorithm for hypertension. The differential diagnosis evident in the AIMS reports closely resembles that for hypertension described in other series12 and elsewhere in this set of articles.13 Management differs from other scenarios involving tachycardia in that immediate support of vital signs is not generally required, a diagnosis often being considered before any treatment is initiated.
-
Hypotensive: the sub-algorithm for tachycardia should be followed until the cardiac rhythm is diagnosed. There will be some benefit in cross referencing to the hypotension sub-algorithm when hypotension co-exists with sinus tachycardia. Physiological models emphasise that sinus tachycardia is most likely to occur as a secondary response to hypotension. Immediate supportive and further definitive treatment will be similar to that described for hypotension. An exception to this is hypotension occurring as a result of tachycardia induced myocardial ischaemia. The sub-algorithm for hypotension incorporates this into its differential diagnosis.7 Management of hypotensive patients with non-sinus tachydysrhythmias is specified in the tachycardia sub-algorithm.
CONCLUSION
Tachycardia during anaesthesia is a common event which is frequently associated with a simultaneous change in status of other monitored vital signs. The differential diagnosis is large and addressing it in a comprehensive fashion must be preceded by supportive treatment. Tachycardia appears to be managed in an appropriate and timely manner in the majority of cases, but this is not without exception. Treatment pathways based on associated blood pressure and prevailing rhythm, in the case of hypotension, appear to offer a functional systematic guide which complements the already proven benefits obtained by employing the core algorithm COVER ABCD.
Acknowledgments
The authors would like to thank all the anaesthetists in Australia and New Zealand who contributed to the 4000 incident reports upon which this and the other 24 papers in the Crisis Management Series are based. The coordinators of the project also thank Liz Brown for preparing the draft of the original Crisis Management Manual; Loretta Smyth for typing; Monika Bullock RN for earlier coding and classifying of data; Dr Charles Bradfield for the electronic version of the algorithms; Dr Klee Benveniste for literature research; and Drs Klee Benveniste, Michal Kluger, John Williamson and Andrew Paix for editing and checking manuscripts. Dr Craig Morgan carried out detailed review of cases and was an author of the initial draft of this paper but declined authorship of the final draft. He is thanked for having done the original hard work and participating in the development of the manuscript.
REFERENCES
Footnotes
-
This study was coordinated by The Australian Patient Safety Foundation, GPO Box 400, Adelaide, South Australia 5001, Australia.
Linked Articles
- Crisis management