Article Text

Statistics from Altmetric.com
INTRODUCTION
This issue of QSHC is accompanied by an online Supplement where abstracts are published from the International Forum on Quality and Safety in Health Care that took place in Paris in April 2008. The abstracts that were commissioned for this Supplement were originally selected by reviewers for oral presentations in Paris.
The over 900 abstracts that were submitted for the 2008 Forum reflect an extraordinary commitment to health care quality and patient safety. They represent improvement work from over 20 countries. These currently published abstracts, along with those that were linked to the 376 posters that were presented at the Paris Forum, emerged from a rigorous peer-review process.
The criteria for their selection reflected the consensus of reviewers and included clear aims, attention to explicitly defined methods, and accurate measurement of outcomes. Good improvement work invariably offers new lessons for better, safer care, and insightful analysis of these projects for lessons learnt was an important part of the successful reports. Finally, mindfulness of how the work might be adapted from these specific settings to other contexts of care is a vital part of effectively reporting good work so that it might contribute to wider opportunities for health care improvement and patient safety.
The Editors of QSHC congratulate the authors of these valuable reports, and look forward to the improvement work that will be reported at the International Forum in Berlin in March 2009.
David P. Stevens. Quality Literature Program, Dartmouth Institute for Health Policy and Clinical Care, 30 Lafayette Street, Lebanon, NH 03766, USA; david.p.stevens@dartmouth.edu
1. IMPLEMENTATION OF SEPSIS RESUSCITATION BUNDLE IN THE INTENSIVE CARE UNIT
B Afessa, O Gajic. Mayo Clinic, Rochester, Minnesota, USA
Background: Sepsis affects over 700,000 people annually in the USA alone and it is associated with a high mortality rate. To improve the outcome of critically ill patients with sepsis, the Institute for Healthcare Improvement (IHI) advocates implementing the Sepsis Resuscitation Bundle that includes tasks to be done within 6 hours after onset of severe sepsis. This study aims to assess the impact of a paper order set on compliance with the Bundle elements.
Assessment of problems: The study was performed in an intensive care unit (ICU) of a tertiary care hospital and included patients treated for severe sepsis or septic shock. We used performance of the following elements of the Bundle within 6 hours of severe sepsis/septic shock as quality indicators: central venous pressure (CVP) monitoring, measurement of central venous oxygen saturation, adequacy of fluid administration, appropriate vasopressor use, appropriate inotrope use, and appropriate red blood cell (RBC) transfusion. With the participation of ICU physicians, nurses, and pharmacists, we developed a written order set based on IHI bundle. We measured the compliance rate with each quality indicator, defects per million opportunities (DPMO) and process sigma level to measure the process of care, and hospital mortality to measure clinical outcome.
Results: There was partial improvement in the process of care, and the mortality rate declined non-significantly during the order set period (see table).
Strategy for change: With the support of the hospital leadership, these results were disseminated to ICU healthcare providers and real time feedback started.
Lessons and messages: The written order set improves some aspects of sepsis care. Potential solutions include a computerized physician order entry and reporting the defects to the healthcare providers in real time. A rapid response team specifically designed to implement the early resuscitation needs of septic patients within 6 hours may also be helpful.
2. UNDERSTANDING THE SAFETY CULTURE IN AUSTRALIAN MATERNITY SERVICES
S Allen, C Homer, M Chiarella. Centre for Midwifery, Child and Family Health, Faculty of Nursing Midwifery and Health, University of Technology Sydney, Australia
Outline of problem: Adverse events in Australian maternity care are common and often avoidable. Safety improvement strategies have focused on learning from adverse events. There’s limited evidence of significant improvements. Understanding organisational safety culture is a suggested strategy to improve safety. Little is known about maternity safety culture in Australia.
Aim: To identify whether measuring the safety culture within a maternity service is a useful method to develop strategies to improve the safety culture.
Outline of context:
Setting: Two public maternity units in NSW, Australia. Concurrently, NSW public hospitals were undergoing restructure.
Participants: Midwives, nurses, obstetricians and medical staff.
Assessment of problems: Study design included 3 stages:
Safety culture measurement:
Safety Attitudes Questionnaire surveys measuring, safety climate, teamwork, job satisfaction, working conditions, management and stress recognition domains.
Semi-structured interviews with key stakeholders.
Development and implementation of safety improvement strategies
Re-measurement of safety culture post intervention
Results: Survey domains were scored 1–100. Fives domains scored <75 and were appropriate for improvement. Improvement strategies were identified. Interview themes included clinical governance, feedback, restructure impact.
Strategy for change: Result feedback to participants occurred. Stakeholder engagement was essential for strategy sustainability; however, stakeholders lacked capacity to participate in strategy development and implementation.
Measurement of improvement: The study was suspended in order to undertake an in-depth analysis about barriers to developing positive safety cultures. Improvement strategies were not undertaken.
Lessons learnt: Safety culture measurement identified areas to improve safety culture. The ability to develop and implement sustainable improvement strategies was limited by stakeholder capacity to engage and competing external factors including organisational restructure.
Message: Safety culture is unit specific but also influenced by external factors existing in complex health systems. An understanding of these factors is important when developing sustainable safety improvement strategies.
3. FAILURE AND RISK FACTORS IDENTIFICATION IN INTRAHOSPITAL TRANSPORT OF CRITICALLY ILL PATIENTS: AN ITALIAN EXPERIENCE
S Amato, R Alvaro, F Germini, L Macale, G Scialò, A Sili, A Stievano, T Brancato, G Druda, A Panà. Rome “Tor Vergata” University – Quality Research Laboratory, Italy
Though in 2005, in Lazio, 71 claims, on a total amount of 15085 Intrahospital Transport (IT), were registered, in Italy there is a lack of standardized procedures and data regarding it.
Rome Tor Vergata University – Quality Research Laboratory – assembled a multidisciplinary working group (WG) to develop an Incident Reporting Form (IRF) in order to identify failure and risk factors in patients’ IT and set up standardized procedures for risk analysis, starting a continuous improvement process regarding medical and nursery procedures in order to prevent and reduce mortality.
The WG used the proactive quality method FMEA/FMECA, VA methodology, to analyse the transport process and created a specific IRF to implement transport safety and facilitate the RPN calculation.
WG mapped any possible failure, calculated behavioral algorithms, created check list for process standardization, univocal identification of patients’ requirements on boarding ambulance and related ambulance requirements, definition of monitoring activities during patient’s on boarding, transport and arriving at hospital, and availability of patients’ data records.
After the application of standardized procedures, WG analyzed 14251 IT in 2006. 14 IRF were gathered: 33 described near miss and 3 adverse events.
At the moment WG is analyzing 2007 IRF in order to gather a complete IRD for the regions involved (Liguria, Molise and Sicilia).
Implementation of measures developed by FMEA resulted in improved readiness and precision in failure and adverse event identification. In fact, data collected in 2005 and 2006 show a significant reduction of both near miss and adverse event.
FMEA success relies on involvement of a committed multidisciplinary and multiregional group of professionals who need to balance their time required to participate in the assessment against their daily duties.
So Italy needs to re-engineer its HCO in order to ensure financial and human resources are available to carry out a continuous improvement process based on prevention.
Warren J, Fromm RE Jr, Orr RA, et al, for the American College of Critical Care Medicine. Guidelines for the inter- and intrahospital transport of critically ill patients. Crit Care Med 2004;32:256–62.
Ehrenwerth J, Sorbo S, Hackel A. Transport of critically ill adults. Crit Care Med 1986;14:543−47.
Schmidt T, Atcheson R, Federiuk C, et al. Evaluation of protocols allowing emergency medical technicians to determine need for treatment and transport. Acad Emerg Med 2000;7:663–9.
Marks PJ, Daniel TD, Afolabi O, et al. Emergency (999) calls to the ambulance service that do not result in the patient being transported to hospital: an epidemiological study. Emerg Med J 2002;19:449–52.
DeRosier J, Stalhandske E, Bagian JP, et al. Using health care failure mode and effect analysis: the VA National Center for Patient Safety’s prospective risk analysis system. Jt Comm J Qual Improv 2002;28:248–67.
4. RESOLVING HETEROGENEITY BETWEEN DIFFERENT EXPRESSIONS OF INPATIENT SATISFACTION
C Auclair, A Giraud-Roufast, MA Grondin, JY Boire, L Gerbaud. Quality Department, CHU Clermont-Ferrand
Background: Results of satisfaction surveys are usually expressed in terms of mean satisfaction. This incites services to reach or exceed the hospital mean. If the results are presented in terms of proportions of very dissatisfied and very satisfied patients, services are incited respectively to identify and correct weak points, or to strive for excellence.
Assessment of problem: We studied the process of ranking services by inpatient satisfaction, considering its three possible expressions. If considering these ways to express satisfaction policy, the ranking of wards remains the same, there is no issue about which to take as the main criteria. But, if they produce different rankings, we have to use them all or consider another composite indicator.
Results: We analysed the results of the multidimensional inpatient satisfaction questionnaire used in 2005 among 2585 patients in Clermont-Ferrand University Hospital. Wards ranked differently according to the three expressions of satisfaction.
Strategies for quality improvement: For issuing this heterogeneity, we created a compound score summing up the three previous ones, based on an adjustment of the mean level of satisfaction by taking into account the percentages of very satisfied and dissatisfied patients, and using fuzzy logic techniques:
Fuzzy Score = Mean + Satisfaction Score − Dissatisfaction Score
The agreement between the ranks obtained with the “Fuzzy” score and the proportions of very satisfied and dissatisfied was stronger than the agreement between the ranks obtained with the mean and these proportions. The ranks according to the mean and the “Fuzzy” score were nearly the same.
Lessons: Using the single “Fuzzy” score is more efficient, because it supplies in one global information all the information provided separately by the mean score and the percentages of very satisfied and dissatisfied patients. One can therefore return this score to the services as the most informative single expression of inpatient satisfaction.
5. FROM “MYSPACE” TO ME SPACE: THE WWWORLD OF MENTORED LEARNING
C Bamford, P Schanzer. National Leadership and Innovation Agency for Healthcare
Background: “MySpace” has popularised the explosion of social networking sites.
What is the appeal? Is it that in today’s busy life there is no time? So “no time” for “me time” and “no space” at work or home to talk about yourself?
How could we give our leaders “MeSpace” by embracing the “MySpace” philosophy?
Our leaders were facing a number of challenges:
Delivering targets and a quality service
Leading change
No time for learning or reflection.
Such challenges required a very different approach to leadership development.
Strategy for change: Clinical leaders were requesting mentoring but had no time to travel or reflect. So an e-mentoring programme was developed that enabled “me time” without the need to travel (see model in fig 1).
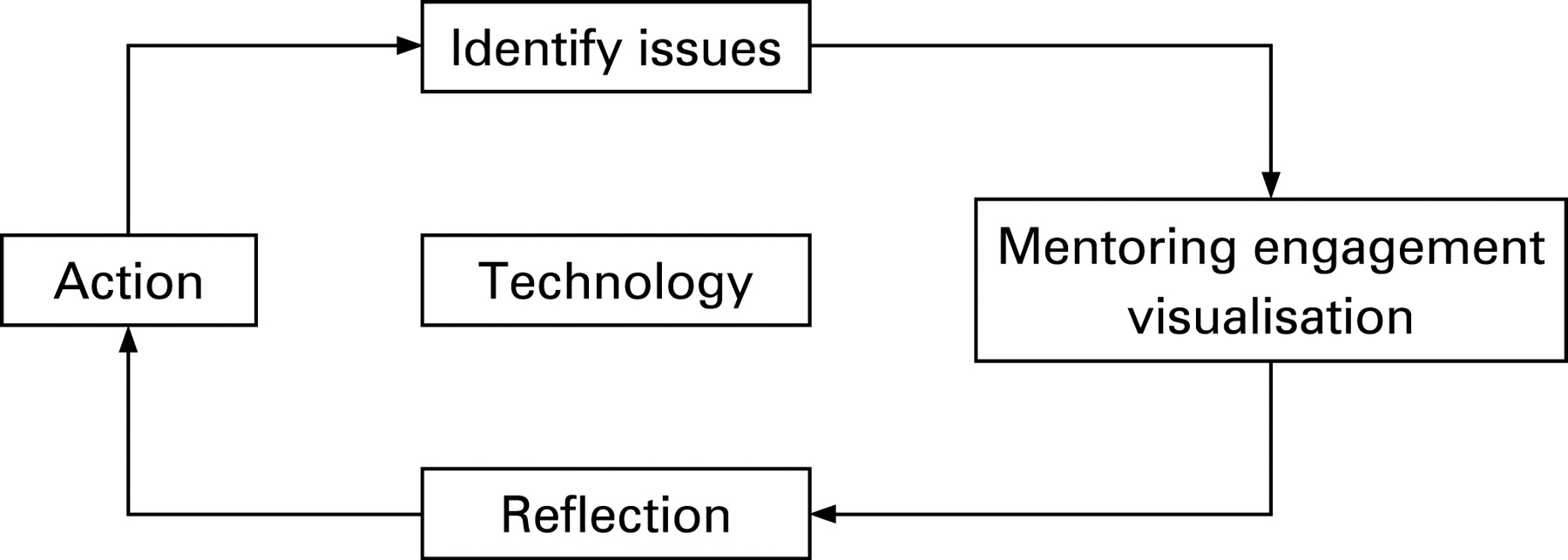
The programme included mentoring through face-to-face, email/telephone, PDA, webcam, and video conferencing. It was supported by a reflective question framework and training guide.
Comments from participants:
The mentoring relationship prompted me to action … focused my mind …identified change
The PDA mentoring made it possible for me to access mentoring support in a car park before a public meeting.
Had undivided attention and time just for me!
71% had a good experience, 29% a very good experience. 90% would recommend to a colleague.
The e-mentoring experience typically took 20 minutes, the maximum 60 minutes; a considerable reduction when measured against a traditional mentoring engagement.
Key lessons learned:
Participants valued face-to-face and matching process for establishing rapport
Acknowledged benefit that “e” element saved time and travel
Technology is only an enabler
Reflective questioning enabled self-discovery and action.
The new digital generation will expect to engage and learn through technology and mobile devices … so the work we are pioneering now will meet future “MySpace” learners’ requirements.
6. PILOT TESTING A QUALITY ASSESSMENT PROGRAM FOR FAMILY PRACTICES IN ONTARIO, CANADA
D Price, L Hilts, AM Barbara, L Dolovich, M Howard, S Laryea, C Levitt. McMaster University, Hamilton, Ontario, Canada
Background: There is no yardstick in Canada for family practices to measure how effectively they are providing safe, patient centred, timely, responsive and comprehensive primary health care. As the health care system and patients’ needs increase in complexity, teamwork becomes increasingly important. The project team of clinicians and researchers developed and tested a voluntary quality assessment program for family practices in Ontario, Canada.
Assessment of problems: International literature review, environmental scan, 13 inter-professional focus groups, teleconferences with experts, and site visits to international quality programs informed the development of the Quality tool and program. Quality assessors were trained with the assistance of international consultants. The program was pilot tested in 3 family practice sites for acceptability and feasibility, and then further tested in 7 Family Health Teams for impact on selected clinical outcomes and inter-professional activities.
Results of assessment/measurement: Practices demonstrated commendable changes: regular practice meetings; human resource policies; physical facility improvements; waiting room changes; patient satisfaction surveys; clinical outcome audits; infection control; medication management; record keeping; improved team behaviour; and increased morale.
Strategy for quality improvement/change: Practices used the Quality tool, containing 80 indicators and 335 criteria, to undertake the practice self-assessment. All practice members, including clinicians and office staff, were encouraged to work together. Practices received Advisor support and training in collecting data. Inter-professional Assessors conducted an external assessment to formally review the progress and provided a detailed written report to each practice.
Lessons and messages:Quality was acceptable, feasible and beneficial in the practice sites. Protected time and opportunity to focus on the “team” aspect of primary care allows busy practice members to identify and implement mechanisms to improve their practice. The application of the Quality tool encourages a culture of measurement, which will allow the evaluation of system-wide improvements in primary care service delivery.
7. SEVERE ASPHYXIA DUE TO DELIVERY-RELATED MALPRACTICE IN SWEDEN 1990–2005
1S Berglund, 1C Grunewald, 1H Pettersson, 2S Cnattingius. 1Department of Clinical Science and Education Södersjukhuset, Karolinska Institutet, Stockholm, 2Department of Medical Epidemiology and Biostalistics, Karolinska Institutet, Stockholm, Sweden
Objective: To describe possible causes of delivery-related severe asphyxia due to malpractice.
Design and setting: A nationwide descriptive study in Sweden.
Population: All patients asking for financial compensation because of suspected medical malpractice in connection with childbirth during 1990–2005.
Method: We included infants with a gestational age of ⩾33 completed gestational weeks, a planned vaginal onset of delivery, reactive CTG at admission for labour and severe asphyxia-related outcomes presumably due to malpractice. As asphyxia-related outcomes, we included cases of neonatal death and infants with diagnosed encephalopathy before the age of 28 days.
Main outcome measure: Severe asphyxia due to malpractice during labour.
Results: 472 case records were scrutinised. 177 infants were considered to suffer from severe asphyxia due to malpractice around labour. The most common events of malpractice in connection with delivery were neglecting to supervise fetal well-being in 173 cases (98%), neglecting signs of fetal asphyxia in 126 cases (71%), including incautious use of oxytocin in 126 cases (71%) and choosing a non-optimal mode of delivery in 92 (52%).
Conclusion: There is a great need and a challenge to improve cooperation and to create security barriers within our labour units. The most common cause of malpractice is that stated guidelines for fetal surveillance are not followed. Midwives and obstetricians need to improve their shared understanding of how to act in cases of imminent fetal asphyxia and how to choose a timely and optimal mode of delivery.
8. PATIENT SAFETY IN MEDICATIONS: INTEGRATING ADVERSE EVENTS INTO A QUALITY DRUG-PRESCRIBING PROGRAM IN STOCKHOLM, SWEDEN
U Bergman, H Almkvist, P Andersson, M Juhasz-Haverinen, Å Pehrsson, G Törnwall-Bergendahl, A Veg, B Wettermark. Division of Clinical Pharmacology & Regional Drug Safety Centre, Karolinska Institutet, Karolinska University Hospital, Stockholm and Division of Finance and Healthcare planning, Division of Drug Management and Informatics, Stockholm County Council, Sweden
A public health approach to adverse drug reactions (ADRs) was tested in Sweden.
Epidemiological studies of ADRs as cause of admission to hospital indicate that >90% are caused by known pharmacological reactions (Type A); 50–70% of these reactions are judged to be preventable. While unpredictable (Type B) reactions may cause withdrawal of the drug and thus is a major concern for the manufacturer and the regulatory agency, the pharmacological reactions ought to be the focus of the health care provider as a reflection of the quality of drug prescribing.
The Swedish Medical Quality Council suggested that reporting of clinically important ADRs should be stimulated by providing feedback to each clinic and that reporting of pharmacological reactions should be considered as a quality indicator. In a field study we found that providing feedback of their ADR reporting was regarded as a clinically useful quality indicator.
In 2006, in Stockholm all primary healthcare (PHC) centres were offered contracts where they received extra payment depending on adherence to guidelines. The contract required each practice to analyse their prescribing and annually to write a “quality report” including questions about ADRs. Among 139 PHCs participating in the program, 50% stated that they had local routines for ADR reporting and 80% discussed ADRs as part of their continuous professional education.
In agreement with the positive experiences, we are now providing feedback of ADRs to all seven emergency hospitals in Stockholm. In 2006, 529 ADR reports per million inhabitants were received at our Regional ADR Centre, a figure well above the highest in Europe (450 ADRs per million, Frauenhofer ISI 2005).
Feedback and economic incentives seem to be powerful tools in enhancing the awareness of ADRs. Integrating ADRs into a drug-prescribing program may result in better understanding of benefits and risks of drug treatment.
9. IMPROVEMENT IN THE TREATMENT OF DEPRESSION IN PRIMARY CARE BY IMPLEMENTING GUIDELINES FOR DIAGNOSIS AND THERAPY IN DEPRESSION
1I Bermejo, 2F Schneider, 3W Gaebel, 4U Hegerl, 1M Berger, 1M Härter. 1Department of Psychiatry and Psychotherapy, University Medical Centre of Freiburg, Germany, 2Department of Psychiatry and Psychotherapy, RWTH Aachen University, Aachen, Germany, 3Department of Psychiatry and Psychotherapy, University of Düsseldorf, Germany, 4Department of Psychiatry, University of Munich, Germany
Objective: Depressive disorders are of great medical and political significance. Evidence-based guidelines have been published, and although educational initiatives have been launched to implement these, guidelines are rarely used. Aim of this study was to implement clinical practice guidelines (CPGs) for outpatient care of depression using a practice-oriented and interdisciplinary approach.
Method: Controlled clinical trial with a naturalistic design (data collection within routine practice) designed as a prospective pre-post study with 29 GPs (intervention (IG): 18; control (CG): 11) and 23 psychiatrists (IG: 17; CG: 4). Overall, 3282 patients (2 samples; pre: 1960; post: 1322) were screened for depressive disorders and GPs’ diagnoses recorded. Subsequent treatment of 698 patients (pre: 361; post: 337) was documented.
Results: 74% of the physicians evaluated the training as good and 88% of the CPGs as very useful for routine. The recognition rate (IG: 30 to 72%; p<0.001; CG: 56 to 76; n.s.) and the positive predictive value (IG: 16% to 33%; p<0.009; CG: 32% to 23%; n.s.) of GPs improves significantly. Physicians improved their clinical effectiveness (symptom reduction >50%) significantly (GPs: IG: 55% to 77%; p<0.04; CG: 56% to 51%; n.s.; psychiatrists: IG: 47% to 73%; p<0.02; CG: 37% to 36%; n.s.). Furthermore, a slight increase was found regarding referrals, but not in the use of the ICD-10 criteria or adequate antidepressant dosage by GPs. Psychiatrists improved their use of formal diagnostic criteria and adequate antidepressant dose prescription.
Conclusions: Through the comprehensive intervention, a substantial improvement in care was achieved. Although the physicians’ behaviour changed only slightly, this was enough to induce positive effects on treatment outcomes, thus challenging studies that did not find changes in clinical outcome. The action programme provides important work, materials and results for an integrated treatment model for depression.
10. THE CHALLENGES OF IMPROVING COMMUNITY HEALTHCARE SERVICES: CAN LEAN THINKING HELP?
E Bradbury. Bolton Primary Care Trust Provider Services, Great Lever Health Centre, Bolton, UK
In April 2007 Bolton PCT Provider Services commenced a Lean Thinking programme to improve access and quality in 10 older people, adult and child services as part of the 18 week elective programme.
Drivers were inability to meet an internal 6 weeks referral to treatment target by December 2007; breaching therapeutic treatment intervals; growing “lifelong” caseloads. Small community teams precluded a lean “kaizen” approach, demanding more flexibility.
Selected services gathered weekly demand and capacity data and categorised caseloads by volume and degree of standardisation. The voice of patients and staff highlighted expectations, frustrations and ideas. 120 patients, carers, front line staff, managers and “fresh eyes” formed 10 teams to walk the patient journey, observe real time processes and identify value, and waste. Root cause analysis showed real problems. Teams agreed ideal and future state service models and calculated impact on performance. They developed action plans, with immediate “Just Do Its” and projects and briefed stakeholders on planned outcomes.
Project teams focused delivery on actions within 1 week to 6 months, supported by sponsors. Ongoing facilitator support, coaching and team specific mini workshops followed. Bulletins, case studies and presentations cascaded improvements and impact.
Improvement measures included process time reduction tracked daily and weekly via visual team control boards; cost benefit and productivity impact were assessed monthly (see table).
Change is not imposed; staff and patients determined their own service model. The concepts of value, waste, and developing processes related to volume and degree of standardisation were embraced. Clinical goal setting can reduce active caseloads and release capacity.
Lean Thinking can be used with community teams and long term condition patients, but be flexible. The outcome is the important thing. Next time we will design a sustainability collaborative to support implementation into the engagement contract.
11. SIMPLE INTERVENTION TO IMPROVE SURVIVING SEPSIS CAMPAIGN BUNDLE COMPLIANCE TO REDUCE SEVERE SEPSIS RELATED MORTALITY
C. W. Buiter, D. H. T. Tjan, R. van Vugt, A. R. H. van Zanten. Hospital Gelderse Vallei Ede, The Netherlands
Brief outline of context/problem: Severe sepsis (SS) is the leading cause of death in the intensive care unit (ICU). It has been reported that sepsis diagnosis, APACHE-II score and Surviving Sepsis Campaign (SSC) goals achieved influence mortality. Initial compliance with sepsis bundles was low and needed improvement.
Assessment of problem and analysis of its causes: A prospective cohort study was performed in all (204) ICU patients with SS between January 2006 and September 2007 in a single centre. Type of sepsis (abdominal, pulmonary, urogenital or otherwise), patient demographics, APACHE-II score, SSC goals achieved and hospital mortality were recorded.
Strategy for change: We implemented an immediate order sticker 7 months after the start of the SSC to use on patient arrival in the ICU.
Measurement of improvement: We continuously and prospectively monitored bundle compliance and mortality in different sepsis categories before and after the implementation of the SSC bundle sticker.
Effects of changes: Total bundle compliance changed from 80.0% to 86.1% (p<0.05). This change was totally attributable to improvement in the Resuscitation Bundle goals achieved within the first 6 hours after ICU admission. No SS mortality change was noted overall. Mortality varied among categories, with a significantly lower mortality in urogenital sepsis than in all other groups. Severity of illness did not change over time. Initial compliance was poorest in patients with pulmonary sepsis. After the implementation of the sticker, in this group compliance significantly improved. A non-significant trend to better outcome was observed in this group (mortality rate 45% vs 37%; p = 0.47).
Lessons learnt: Implementation of an SSC bundle order sticker improved compliance in achieving SSC goals. A non-significant trend to better outcome (mortality) was observed in pulmonary sepsis.
Message for others: A simple intervention by means of an order sticker with combined medical orders of SSC bundles can improve compliance in a relevant clinical setting.
12. MOUTHING OFF ABOUT BEST PRACTICE MOUTH CARE TO REDUCE RISK OF VENTILATOR ASSOCIATED PNEUMONIA AT LYELL MCEWIN HOSPITAL, SOUTH AUSTRALIA
1W. S. Butvila, 1,2MR Reilly, 3,4G Sturman. 1Intensive Care Unit, Lyell McEwin Hospital; Elizabeth Vale, South Australia, 2Flinders University, Bedford Park; South Australia, 3Department of Health; South Australia, 4Children, Youth and Women’s Health Service; North Adelaide, South Australia, Australia
Brief context: The Lyell McEwin Hospital participated in the Australian “Safer Systems Saving Lives” (SSSL) initiative and implemented the “Preventing Ventilator Associated Complications” (PVAC) bundle for ventilated patients and demonstrated improved outcomes.
Non-standardised, pre-existing care for ventilated patients did not reflect the PVAC principles. Research highlighted an increased risk of ventilator acquired pneumonia (VAP) development from pooled sub-glottal secretions and colonisation of resident bacteria in the mouth and oropharynx.
Outline of problem: Analysis of bundle components identified disparity of practice and non-standardised oral care in ventilated patients. The preliminary audit of 58 patients ventilated >24 hours in intensive care unit (ICU) exposed a VAP incidence of 24%. Compared to non-VAP patients, VAP patients averaged 3 days longer in hospital, more than doubled the length of stay (LOS) in ICU and trebled ventilation hours. VAP added financial liability in every case.
Strategy for change: Clinical practice changes initiated by project leaders included education of all bundle aspects and the mandatory mouth-care regimen—costing $18.91 per patient.
Limited procedural documents to guide staff facilitated the development of the evidence based mouth-care routine.
Auditing indicators, including microscopy of tracheal aspirates enabled early intervention. Data results, tracking bundle compliance were reported and displayed monthly.
Measurement of improvement: Retrospectively analysed financial data compared VAP to non-VAP patients. VAP represented an additional $15,473/episode, and averaged $43,323 monthly prior to implementation of PVAC and mouth-care routine, after, PVAC expenditure decreased to $9025/month.
Within 1 year, the VAP incidence decreased to 5.3%. Coupled with the patient’s personal health benefit was 80% cost reduction—a monthly saving of $34,298 or $519,876 annually.
Lessons learnt: Team work, system improvement tools and applied evidenced based practice created a sustainable culture for patient improvement. The mouth-care package facilitated improved safety, clinical and financial outcomes for both patient and institution.
13. OBSTETRIC MATERNAL CRITICAL CARE: ARE WE DOING OUR BEST?
S Calva, E Gollo. Department of Anaesthesia and Intensive Care, St Anna Hospital, Turin, Italy
St Anna Hospital is a tertiary care university centre specialized in obstetrics and gynaecology (more than 8500 deliveries/year and a dedicated intensive care unit (ICU)).
Maternal mortality and severe morbidity can be still today a hard challenge to face (maternal mortality rate in ICU varies from 2.3% to 7.5% in developed countries).
In our hospital women with critical care pregnancy-related problems are admitted in a specialized ICU and from 1998 we have reduced the maternal mortality rate in ICU to 0.72% (0.013% of deliveries vs more than 0.02% as reported in international literature).
From 2003 we have implemented a client-oriented project to prevent potential life-threatening pregnancy-related complications. An interdisciplinary team has been working to appropriately respond to normal labour and delivery, so that uncomplicated cases do not become critical. We implemented: internal guidelines; anaesthesiological examination for all pregnant women; free epidural analgesia; communication skill courses; early and programmed admission in ICU for potentially critical patients. We joined the Italian Group for Intensive Care Evaluation (GiViTI network) and we are involved in a project for the assessment of the quality of ICU in Italy.
An early and prompt admission to a specialized ICU may help to lower maternal mortality and morbidity during pregnancy. The organization of a critical care team, with good communication skills, allows team members to anticipate potentially serious risk for mother and child and to implement best practice procedures. Improving communication skills for professionals allows to encourage individual excellence.
14. POSTOPERATIVE PAIN MANAGEMENT IN THE NEONATAL INTENSIVE CARE UNIT (NICU): BENEFITS FROM AN INTERDISCIPLINARY QUALITY IMPROVEMENT APPROACH
BS Carter, D Hodge, K Nelson, A Potts, SR Hays, J Deshpande. Vanderbilt Children’s Hospital in Nashville Tennessee, USA
Background: Postoperative pain management in the neonatal intensive care unit (NICU) is inconsistent. Unmanaged neonatal pain has negative outcomes.
Causes: A chart audit of 50 postoperative NICU patients revealed needs for improved pain assessment and management associated with the nature of the procedure, type, timing and dose of analgesics, pain scale scores, and responses to medication.
Strategy: Change was implemented through three repetitive Plan-Do-Study-Act (PDSA) cycles (50 patients each) with educational interventions, a computerized physician order-entry set, and a table of expected duration of pain following 17 common surgical procedures. An interdisciplinary NICU pain management team met regularly over 3 years guiding change. Results were disseminated through unit-based education, new staff orientation, physician education conferences and incorporation into a house-officer manual, and availability of team members on the unit for consultation.
Improvements: Change was measured during repeated PDSA cycles examining improvement in medication use, reduced time until first analgesic dosing, and improved documentation of the Neonatal-Pain Agitation and Sedation Score (N-PASS).
Effects: Pain control improved. Staff had less angst about delayed or inappropriate pain management. Physicians reported ease of ordering medications. Use of non-opioid analgesics improved and inappropriate use of anxiolytics declined.
Lessons: The value of the interdisciplinary team, unit-based staff involvement, and a continuous process that looks carefully at data cannot be overstated. Such efforts require a time commitment and also likely financial support. Our work was accelerated by extramural grant support.
Message: Pain can be better managed in the NICU, and the quality performance improvement methods described are applicable to other units of patient care.
This work was conducted in the Neonatal Intensive Care Unit (NICU) of the Monroe Carell, Jr. Children’s Hospital at Vanderbilt University Medical Center in Nashville Tennessee, USA by members of the Departments of Pediatrics, Nursing, Performance Improvement and Pharmacy.
15. REDUCTION IN THE RATE OF ELECTIVE TERM LSCS WITH NO MEDICAL INDICATION UNDERTAKEN PRIOR TO 39 COMPLETED WEEKS GESTATION

MA Cattell, MC Nicholl. Royal North Shore Hospital, Sydney, Australia
The risk of respiratory morbidity is increased in babies born by caesarean section (C/S) before labour, but this risk decreases after 39 completed weeks. Therefore elective or pre-labour caesarean section ought not to be routinely carried out before 39 completed weeks.
Primary data sources indicated the rate of term elective caesarean sections with no medical indication undertaken before 39 weeks gestation at our institution was approximately 30% in 2005 and 2006. The project team undertook this particular work for the 6 months from 1 March 2007 to 31 August 2007.
A multidisciplinary team with fundamental knowledge was formed to investigate the extent of the problem and included an obstetric consultant, delivery suite midwifery manager, clinical research midwife, delivery suite staff, quality improvement advisor and a data analyst.
The aim of the project was to reduce the rate of term elective caesarean sections with no medical indication prior to 39 completed weeks gestation to 10% of all term elective caesarean sections over the stated 6 months period.
A diagnostic phase was conducted and areas for possible intervention that would result in the greatest improvement were identified. These interventions included pre-emptive education and the provision of evidence folders in key clinical areas relating to the project aim.
Results demonstrated that over the 6 month period of the project, the rate of elective C/S with no medical indication done prior to 39 weeks gestation in the target group fell to 12.1%. Over the same time frame the number of admissions to the neonatal intensive care unit of term babies born by caesarean section at less than 39 weeks was reduced to zero.
To sustain these improvements, there will be continuing education of clinical staff and dissemination of the results. The project aim will continue to be monitored and interventions implemented as required.
16. INTRODUCING SERVICE IMPROVEMENT TO THE INITIAL CLINICAL EDUCATION OF HEALTH AND SOCIAL CARE STAFF
S Fowler-Davis, G Janes, S Lister, J Penny, M Cooke. University of Warwick, Coventry, UK
This paper describes the first year of a project to develop education for the early stages of healthcare providers careers. This project includes the development and piloting of the first iterations of the three modules across three sites.
All three courses focused their learning objectives around common elements:
That all clinicians appreciate the importance of their role in service improvement (SI)
Engaging service users and carers in both the education and in SI
Effective use of tools including process mapping, interviews, activity observation and PDSA cycles.
The importance of personal leadership and responsibility for improvement in practice settings.
All the modules consisted of a short introductory component, outlining the philosophy and basic tools and used an interdisciplinary learning approach and user experience. All had a second component focused on a project or work based learning.
The participating students expressed a high level of interest and enthusiasm for the course.
The key issues raised for consideration when spreading the adoption of these modules included:
Lack of timetable space
Relatively few faculty confident to teach such a course
NHS capacity to support and mentor students
Student projects must be realistic and relevant
Developing an infrastructure to support work based learning and development in improvement
An effective infrastructure to engage and support service users and carers to contribute to the learning
Limited range of service improvement undergraduate learning materials.
It is concluded that short modules, included as part of initial clinical education, are valued and have the potential to make a significant contribution to the service improvement agenda in healthcare. There are, however, major obstacles to overcome before it could be routinely included in the curriculum for all healthcare professionals.
17. CHALLENGES IN DEVELOPING A CRISIS SERVICE
C Crawford. NHS Forth Valley, Scotland, UK
Forth Valley is a Scottish Health Board region of over 1000 square miles, with a population of 277,000. In April 2005, there were 80 acute psychiatric in-patient beds, with around 71 admissions each month. The new Mental Health Act in Scotland was the catalyst for developing a home based treatment service for acute psychiatric patients. The Intensive Home Treatment Team (IHTT) is a multidisciplinary team that operates extended hours over 7 days. It is the gatekeeper for admissions providing an alternative to admission whenever possible. The team also facilitates early discharge of patients.
Clinical activity of the IHTT and the acute in-patient service was collected by the team. The Scottish Development Centre for Mental Health (SDC) gathered views and experiences from IHTT patients and carers using the Client Satisfaction Questionnaire (CSQ-8) and structured interviews. The SDC also gathered data from a wide range of other stakeholders, including GPs and other clinicians. Clinical outcomes were measured using the FACE assessment.
The in-patient bed numbers were reduced from 80 to 65. Even with this reduction, the average bed occupancy is currently below 80%. During the first 20 months of the service, there were over 1600 referrals to the IHTT, with 43% of them taken on for home treatment. 17.8% of assessments were admitted by the IHTT at some point. 75% of carers and users stated that they were very satisfied with this new service. Clinicians welcomed this alternative to inpatient care.
Home based treatment for the majority of psychiatric patients presenting in crisis is possible. Communication is vital within the team and the external agencies. Risk assessment has to be routine and well documented. Most patients and clinicians prefer home treatment. It is vital to collect evidence to continually inform partner clinicians at the beginning of a new service.
1. Johnson, et al. Outcomes of crises before and after the introduction of a crisis resolution team. Br J Psych 2005;187:68–75.
2. Gluber, et al. Crisis resolutions/home treatment teams and psychiatric admission rates in England. Br J Psych 2006;189:441–5.
3. Coutts P, McLaren G, Crawford C. Providing alternatives to inpatient care: the intensive home treatment team in Forth Valley. The Mental Health Review 2006;11(3):37–40.
4. Scottish Development Centre for Mental Health & NHS Forth Valley Mental Health Services. Forth Valley Intensive Home Treatment Team Pilot. Final Report. Available from the SDC and Forth Valley, 2006.
18. NATIONAL CLINICAL INCIDENT REPORTING: A DRIVER FOR PATIENT SAFETY
D Dunne, AM Oglesby, A Quinlan. State Claims Agency, Clinical Indemnity Scheme, Republic of Ireland
The Clinical Indemnity Scheme (CIS), managed by the State Claims Agency (SCA), is the state funded scheme within the Republic of Ireland that provides indemnity to health agencies funded in whole, or in part, by the Exchequer against the cost of claims brought against them for personal injury arising from clinical negligence. The SCA introduced STARS web, a national secure web based incident reporting system in 2003 which links hospitals and other healthcare enterprises to a national database. Organisations can only access their own data whereas the CIS has access to all of the incident data.
Between 1 January 2004 and 31 December 2007 there were 139,978 clinical incidents reported on this system. The number of incidents reported has incrementally increased during this period, reflecting both an increase in the number of facilities gaining access to the system as well as an increasing awareness of the need to report clinical incidents to the CIS.
The top five clinical incidents reported on the system during the above period are shown in the table.
Detailed incident data reports have been disseminated in an anonymised and aggregated fashion by the CIS in a variety of ways, such as inclusion in lectures and publication in the quarterly CIS newsletter.
Reports are provided to local, regional and national stakeholders to assist in identifying quality improvement opportunities and areas that require specific focus, changes in practices and policy/protocol/procedure development.
More detailed data analysis in conjunction with other sources of information, such as hospital activity, claims and clinical audit data is required to ascertain a more complete picture of the national patient safety status.
National incident reporting can act as a driver for patient safety by identifying adverse clinical events that represent quality improvement opportunities.
19. IMPACT OF A COMPUTERIZED MEDICATION SAFETY SYSTEM INTERFACE ON MEDICATION ERRORS
W Fields, R Snyder. USA Agency for Healthcare Research and Quality R01 HSO13131
An electronic interface was implemented between the pharmacy computer system and nursing electronic medication administration record (eMAR) in two tertiary community hospitals in California. The goal was to eliminate medication order inconsistencies between these two computer systems.
Before interface implementation, nursing and pharmacy entered medication orders into independent computer systems and conducted manual reconciliations to detect inconsistencies. An interface was proposed to improve order management consistency and decrease subsequent medication errors.
Medication safety event data were collected for 20 days at 1 month before and 6 months after interface implementation in 17 patient-care units. Events were detected with non-voluntary (e.g., computerized lab values) and voluntary (e.g., incident reports) methods. An event review panel classified events for type and severity. Event types included preventable and non-preventable adverse drug events (ADE), and intercepted and non-intercepted potential ADEs. Severity was determined from an adapted National Coordinating Council Medication Error Reporting and Prevention (NCC MERP) Index.
Statistical analysis with the Fischer’s Exact Test pre- and post-interface implementation indicated that Hospital 1 (n = 10 units) had a significant increase (p = 0.01) in number of events, particularly preventable ADEs (p = 0.001). Intermediate care units (n = 4) experienced the greatest impact with a significant increase (p = 0.01) in preventable ADEs. Hospital 2 (n = 7 units) had a decrease in overall number of events that was clinically but not statistically significant (p = 0.12). The critical care units (n = 2) experienced a clinically significant decrease (p = 0.06) in non-intercepted potential ADEs.
Health information technology (HIT) solutions will have different and, potentially, unintended consequences across hospitals. Careful attention needs to be given to the potential impact on work flow processes, and pre-post evaluation to accurately assess HIT solutions. Electronic interfaces do not always solve patient safety problems. When making decisions related to medication safety system solutions, broader organizational aspects, e.g., workflow impact, must be considered. [296]
20. COLOUR CODING: A WAY TO PREVENT SYRINGE SWAP ERRORS (SSES). PROBABILISTIC RISK ASSESSMENT APPROACH (PRA)
Ph Garnerin, T Perneger, D Tsoncheva, M Ares, P Chopard, P Bonnabry. University Hospitals of Geneva (HUG), Switzerland
Brief outline of context: This PRA analysis was conducted in addition to an experimental randomized controlled study.
Brief outline of problem: Our study showed that colour coding decreases the frequency of SSEs, increases the occurrence of omitted checks (O_CHECKs), and has a weak impact on selection errors (Sel_ERRs) when intra-colour similarities between drug names exist. To assess the robustness of this result, we conducted a PRA analysis.
Assessment of problem and analysis of its causes: a SSE always results from the combination of a Sel_ERR, and either an O_CHECK or a check failure (F_CHECK: check failing to detect Sel_ERR when performed).
Strategy for change: Colour labels (CLs) aim at reducing the frequency of Sel_ERRs by limiting the choice to drugs belonging to the same colour. However, the frequency of O_CHECKs could increase since operators could use colour as a way for identifying syringes. B&W labels (BWLs) are intended at decreasing the frequency of O_CHECKs by strengthening vigilance but could increase the frequency of Sel_ERRs because of closer similarity between syringes.
Measurement of improvement: The probability of SSEs was computed from the probabilities of Sel_ERR, O_CHECK and F_CHECK measured via our experimental study [pSSE = pSel_ERR*(pO_CHECK+(1−pO_CHECK)*pF_CHECK)]. Assuming binomial distributions for these three parameters, differences in pSSEs were explored using bootstrap analysis (n = 10,000) in three distinct circumstances (see table) to assess CLs dominance over BWLs.
Lessons learnt: CLs strongly dominates BWLs when there are no name similarities, or when name similarities are present within distinct colour codes. However, CLs provide only a slight advantage when name similarities exit within the same colour code.
Message for others: When drug name similarities are present within the same colour code, other differentiation means such as Tall Man letters (ATROpine) should be added to limit Sel_ERRs.
21. PEDIATRIC SEPSIS AND SHOCK EARLY INTERVENTION PROTOCOL
RA Greenberg, G Larsen, N Mecham, T Hill. University of Utah, Primary Children’s Medical Center
Early intervention for shock and sepsis improves the morbidity and mortality for pediatric patients. A multidisciplinary team of nurses and physicians developed an emergency department (ED) protocol to identify and treat patients with sepsis/shock.
Brief outline of problem: Cases of unrecognized and under-treated sepsis and shock were identified at our institution. We hypothesized that initiation of a care protocol to better identify and treat patients in the ED would improve outcome.
Assessment of problem and analysis of its causes: A retrospective review of sepsis and shock cases from 1999–2006 estimated a mortality rate of 8.6%. Upon review, it was clear that there were two areas for improvement: 1) earlier recognition and 2) more aggressive treatment.
Strategy for change: The protocol criteria were developed using published pediatric sepsis/shock guidelines. We conducted a 2 week pilot study in the ED to determine study feasibility. We used the results of the pilot to help educate and train the ED staff regarding implementation.
Measurement of improvement: Compliance with protocol elements and patient outcomes were monitored.
Effects of changes: Our protocol contains 6 elements (see table for the listed elements). We found an improvement in adherence to 3 of the 6 elements over time (see table). Overall mortality was 3/42 (7.1%). For those patients who met inclusion criteria but whose care deviated from the protocol, the mortality was 3/18 (16.7%). Our protocol thus far has identified all patients, except one, with sepsis in the ED.
Lessons learnt: We found that involvement of staff in the process of implementing the protocol and specific education, with timely feedback on outcomes of patients with sepsis/shock, has increased compliance.
Message for others: The successful implementation of an ED triage protocol has potential to improve the care given and the outcome from pediatric sepsis and shock.
22. IMPLEMENTATION AND EVALUATION OF THE IN-POSSESSION MEDICATION POLICY (2005) IN THE NORTHERN IRELAND PRISON SERVICE (3 PRISONS)
H Hirst, J Haines-Wood. Northern Ireland Prison Service
Outline of problem: There were large volumes of medication rigidly designated as abusable or non-abusable that had to be administered to prisoners by healthcare staff daily. Care was affected as prisoners were not getting medicines at an appropriate time and there was high risk of error.
Assessment of problem: A multidisciplinary team assessed the challenges relating to medication issue in the prison environment. Particular risks identified were restricted prisoner movement, access to prisoners, vulnerability of prisoner group, trading, bullying, drug addiction and overdose. Team agreed In-Possession Policy based on individual risk assessment.
Strategy for change: Policy developed, agreed by prison management and implementation plan drawn up. Key stakeholders briefed, staff communication and training delivered. In-cell storage for medicines agreed. Patient information leaflet produced for prisoners. Launched first in one location, reviewed, minor changes made, rolled out in one prison then full implementation in all prisons.
Measurements
% In-Possession medication calculated monthly
Issues arising discussed and resolved through multidisciplinary team
Healthcare staff carried out monitoring checks of medicines concordance
Policy reviewed after 6 months and amendments made
Full clinical audit undertaken during 2007.
Effects of changes
High level of in-possession medicines achieved averaging 70% across the 3 prisons
Increased prisoner knowledge about medicines
Healthcare staff time released
No significant medication related harm reported.
Lessons learnt
There would be a need to:
establish a baseline of medication related harm before making any changes
define monitoring required and clearly communicate this with staff
be realistic about what can be achieved due to variability of prison and prisoner type
ensure that policy balances individual assessment and risks posed by particular medicines.
Messages for others
Safe systems need to be maintained to administer medicines to vulnerable prisoners
Secure storage should be a requirement of every In-Possession scheme
Senior management need to be involved from the outset.
23. IMPROVING QUALITY IN WELSH CRITICAL CARE: A NATIONAL COLLABORATIVE APPROACH TO IMPLEMENTING CARE BUNDLES
CM Hancock. National Leadership and Innovations Agency for Healthcare (NLIAH)
The Welsh Critical Care Improvement Programme (WCCIP) was launched in March 2006 with the aim of improving the quality of care across all 18 Welsh adult general intensive care units (ICUs) by the introduction of ventilator and central line care bundles.
A collaborative programme methodology was used to implement the WCCIP involving frontline staff in leading change at a local level. Regular national events were used to train the local programme managers, agree the bundle contents, inform on programme progress and decide the direction for the smaller local improvement groups.
Compliance with the care bundles on an individual patient and then whole ICU basis was measured and calculated as a percentage at each site on each day of the programme and then uploaded and stored on a web based database.
The database generated reports giving mean monthly compliance with the care bundles for each unit. As this compliance figure represented a reduction in the adverse events which were due to omission of treatment, it was accepted as a proxy for quality improvement.
Aggregate national ventilator bundle compliance rose from 82% in June 2006 to 97% in March 2007, while aggregate national central line bundle compliance rose from 26% in June 2006 to 98% in March 2007.
All units have experienced an increase in service improvement activity as a direct result of this programme and most have demonstrated improvements in outcomes.
The salient features of this programme were collaborative decision making and strategy development at a national level, centralised electronic data collection, rapid feedback and the structured training programme. The participants have demonstrated that large improvements in patient safety can result from relatively small changes in the systems of care delivery.
24. CASE MANAGEMENT IMPROVES QUALITY OF CARE AND ENHANCES CLINICAL OUTCOMES FOR OUR CUSTOMERS: A 3 YEAR STUDY
M Hendriks, R Mahendran. Institute of Mental Health, Singapore
Introduction: The hospital’s objective was to provide coordinated quality care for patients from hospitalization to discharge. A service that could integrate and coordinate care was required.
Method: Case managers (CMs) were introduced in the acute, rehabilitation and forensic psychiatric units. A “brokerage model” was adopted for use and CM referrals and patients’ clinical outcomes were closely tracked to monitor the service.
Results:
a. Increased CM cases
1021 referrals in 2004, 1066 in 2005, and 2185 in 2006. Of these, 185(18%) accepted for CM in 2004, 375(35.2%) in 2005 and 1631(74%) in 2006.
b. Reduced readmissions, hospitalization days and treatment defaults
In 2004, 11 (5.9%) readmitted within 28 days and 15 (8.1%) readmitted after 28 days of discharge. In 2005, 8 (2.13%) readmitted within 28 days and 24 (6.4%) after 28 days. In 2006, 25 (1.5%) readmitted within 28 days and 71 (4.3%) after 28 days. In 2005, patient’s readmission rates showed 65 readmissions before CM but 26 readmissions (excluding the index admission) after CM; also hospitalization days decreased (1014 to 104) and 27 (7.2%) patients defaulted follow-up appointments.
c. Increased psychoeducation, counselling sessions and telephonic case management
1. Psychoeducation: 819 (2004), 448 (2005), 1263 (2006)
2. Individual counselling: 235 (2004), 289 (2005), 566 (2006)
3. Family counselling: 90 (2004), 172 (2005), 438 (2006)
4. Telephonic case management: 291 (2004), 707 (2005), 931 (2006)
d. Increased community linkages
227 (2004) to 520 (2005) and 993 (2006)
e. Reduced suicide, forensic complications, crisis management and cases requiring police assistance
1. Suicide attempts: 16 (2004), 1 (2005), 0 (2006)
2. Completed suicide: 1 (2004), 0 (2005), 1 (2006)
3. Forensic complications: 0 (2004), 4 (2005), 2 (2006)
4. Cases requiring police assistance: 1.73% (2004), 1.07% (2005), 0.18% (2006)
f. Service expansion to psychogeriatric unit and community psychiatry
Conclusion:
a. CM improved care delivery and enhanced clinical outcomes for patients.
b. Selecting the appropriate CM model, commitment, training and goal setting are crucial factors for success.
25. REDUCING MATERNAL MORTALITY IN ECUADOR THROUGH COLLABORATIVE IMPROVEMENT OF OBSTETRIC CARE
J Hermida. University Research Co, LLC/USAID Health Care Improvement Project
Context: To reduce maternal mortality (83/100,000 births in 2005), the Ministry of Health (MOH) and the Quality Assurance Project (QAP) had carried out in 2003–2005 a collaborative to improve essential obstetric care. The collaborative had limited impact on management of complications. Six of Ecuador’s 22 provincial hospitals participated in a follow-on collaborative to improve care for pre-eclampsia, haemorrhage and sepsis—the main causes of maternal mortality. The hospitals each attend approximately 2000 deliveries per year, and about half of maternal deaths occur in hospitals.
Change strategy: In 2006 QAP/MOH developed evidence based guidelines for management of obstetric complications. In 2007, hospital quality improvement teams participating in the collaborative introduced changes through PDSA cycles and assessed compliance with standards through monthly clinical record audits. Hospital teams met quarterly to share and discuss experiences. General changes introduced: (1) conducting highly visible audits of every hospital maternal death with MOH authorities and discussing results openly; (2) establishing a standard for time delay for a qualified provider to be at the ER when a complication arrives; (3) establishment of “code red” procedures; and (4) organizing daily supervision. Specific changes introduced in care of pre-eclampsia: immediate assessment of proteinuria using dipsticks; mandatory protocol for magnesium sulphate use; ensuring availability of C-sections on weekends and holidays; providing sphygmomanometers to ER providers. Changes introduced for haemorrhage: introduction of mandatory active management of third stage labour in every delivery; training staff in management of hypovolaemic shock; and ensuring blood availability
Effects: Compliance with standards has improved steadily over the year, although the changes have been resisted by some physicians (see fig). Pre-eclampsia and haemorrhage improved more than sepsis. In-hospital maternal deaths decreased by 37%.

Lessons learnt: Improving care processes for complications management can reduce in-hospital maternal mortality in a relatively short period, even without major additions of personnel or equipment.
26. CIRRNET: CRITICAL INCIDENT REPORTING & REACTING NETWORK (THEME–SAFETY: INCIDENT REPORTING)
MA Hochreutener, O Frank, S Staender. Swiss Patient Safety Foundation
Context and problem: Many Swiss hospitals have incident reporting systems, but little dissemination of local knowledge happens. Therefore we constituted CIRRNET —the Critical Incident Reporting & Reacting NETwork, together with the Swiss Association for Anaesthesiology and Reanimation. 24 Swiss hospitals (10% of public hospitals) are involved.
Strategy: Bring knowledge together on a technical and social platform—that’s the concept. CIRRNET is a learning network, based on local reporting systems. Local reports are gathered in a central database. Supraregional relevant safety problems (called “hotspots”) are identified. Experts analyse hotspots and develop broadly available improvement recommendations. Besides this centralized processing of reports, CIRRNET facilitates the mutual learning of network participants via web-based access to the database.
Results: For implementation, many technical and functional aspects had to be solved (definition of minimal data set, conceptualization of database and exchange platform, compatibility of local systems with database, data protection and flow) and a participation policy was developed. Then, the network was established. Since October 2006 we collected 460 reports (February 2008) and defined a concept for processing the reports and the identification of three types of hotspots: hotspots that need a working group based evaluation, hotspots that can be spread as pragmatic short recommendations about simple relevant problems (“Quick-Alerts”), and hotspots that speak for themselves. We identified several hotspots and called experts to work out improvement recommendations which are spread broadly. Beside that, participants exchange experiences directly on the internet platform www.cirrnet.ch.
Lessons learned: It is not essential to analyse every report and you don’t need a sophisticated classification system to identify safety hotspots. Just start with few key problems in a pragmatic way. Technology is nice to gather information, but for the analysis, you have to assemble people. CIRRNET as a model can be expanded on other institutions and specialties.
27. PATIENT INVOLVEMENT IN CLINICAL DECISIONS AND PATIENT SATISFACTION IN GERMAN PRIMARY CARE
M Härter, L Hölzel, L Kriston. Section Clinical Epidemiology and Health Services Research, Department of Psychiatry and Psychotherapy, University Medical Center Freiburg, Germany
Background: Involvement of patients in clinical decisions is intensively discussed in recent years. Empirical knowledge on patient participation is increasing rapidly. Involvement of patients in medical decisions plays a special role in primary care, as this setting is characterized by the most frequent patient-clinician contact. There is an important gap between patients’ preferences of being involved in treatment decisions and the involvement of patients in daily practice.
Objectives: The impact of being involved in treatment on the satisfaction with the primary care provider was investigated in a sample of 2000 primary care patients. This association was examined in order to identify key concepts for quality improvement strategies, e.g. training of physicians, development of decision aids, integration of patient involvement recommendations in guidelines, and financial incentives.
Assessments: Psychometrically sound instruments were used to assess patients’ preferences for being involved in medical decision making (Autonomy Preference Index; API), the involvement of patients in decision making (Shared Decision-Making Questionnaire; SDM-Q), the satisfaction with decisions (Decisional Conflict Scale; DCS) and the satisfaction with the primary care provider (self-constructed questionnaire). Structure equation modelling based path analysis was applied. Sociodemographic and clinical characteristics were included as possible confounders.
Results: Increased patient involvement in clinical decisions proved to be strongly associated with decreased decisional conflict. Both constructs predicted higher satisfaction with the provided health care. The expected positive association between patients’ preference for involvement in decisions and actual involvement could not be confirmed.
Lessons and messages: Patient participation can lead to higher satisfaction, thus it may be considered as an appropriate quality indicator for primary health care.
Acknowledgements: The project was conducted in cooperation with Gesundes Kinzigtal GmbH, Health Insurance Fund AOK Baden-Württemberg, Health Insurance Fund LKK Baden-Württemberg, and the Department of Medical Sociology, University of Freiburg.
28. ACHIEVING EARLIER DISCHARGE TIME THROUGH TEAMWORK AND LOCAL INITIATIVE
GY Jenq, SM Bacon, TJ Balcezak, LI Horwitz. Yale New Haven Hospital, USA
Background: Late mean discharge time reduces bed availability during peak hospital admission periods. We designed an intervention to increase discharges before 11 am.
Methods: Six units participated in an early discharge campaign (medicine, geriatrics, surgery, pediatrics and psychiatry). A centralized Throughput Committee set targets, convened periodic networking meetings, and disseminated real-time data. Units devised their own changes to workflow processes, task prioritization and communication. We measured percent of discharges before 11 am.
Results: Intervention units increased the mean percent of 11 am discharges from 12.1% to 20.5% after 6 months (p<.0001). Non-intervention units were unchanged (11.6% to 11.5%). However, after another 5 months 11 am discharge rate fell to 12.8% on intervention units (see fig).

Strategies: Successful units coordinated discharge discussions early in admission; provided 24 hour notice by physicians about patients eligible for discharge; initiated paperwork, prescriptions, transportation and patient/family discussions the day before discharge; and jointly confirmed the day’s discharges. Motivational strategies included recruitment of local physician and nurse champions, friendly competition, public recognition, individual feedback, symbolic rewards, unit-level pride and front-line dissemination of data. Competing priorities, lack of local champions, ambiguous lines of authority (particularly for cases involving multiple specialists), resistance by educators to extrinsic rewards, difficulty convening key players (especially on units without localized physicians), placement or transportation delays, and data that was not sufficiently unit-specific or actionable were the largest challenges to success. Failures after initial success were related to teamwork breakdown such as absence or replacement of key participants, and fewer patients with unit-based physicians.
Lessons: Intervention units successfully increased their 11 am discharge rates but sustainability was challenging. Teamwork, data feedback, local champions and advance planning were the driving factors in initial success, while teamwork was most crucial to sustainability. Improvement of 11 am discharge requires clear goals, local champions, culture change, actionable data and maintenance of full team involvement.
29. GOOD CATCH: FINDING NEAR MISSES AND PREVENTING ERRORS
R Hussain, YD Dlugacz. Krasnoff Quality Management Institute
Background:
Context. The Krasnoff Quality Management Institute, with the North Shore-LIJ Health System, has successfully created/implemented a perioperative specific “Good Catch/Near Miss” reporting program.
Problem. To alert caregivers to potential errors through developing a process and tool for increasing reporting of near misses by 100%.
Assessment of problem: During the 2 month pre-implementation, 19 near misses were captured using the original incident tracking system. To find the under-reporting causes, focus groups with line staff were conducted. Based on this, the following were implemented: (1) operationally-defining near misses; (2) creating a time-efficient data collection process; (3) innovating a real-time web-based reporting; and (4) prioritizing/implementing PDCA methodology.
Strategy for change: Potential errors were not reported because in the high-risk fast-paced environment of ORs, potential errors were simply corrected; without opportunities for improvement. The Good Catch Product Suite, that was developed, encouraged Near Miss reporting. The project was pilot-tested in 1 tertiary hospital for 2 months, then implemented across 6 hospitals over 1 year. The following steps were implemented:
Elicit/analyze staff feedback to understand hesitation in reporting
Develop anonymous reporting process
Create web-based database for data collection/real-time reporting
Encourage Blame-Free reporting of errors
Standardize reporting tool
Supply monthly feedback to Performance Improvement (PI) committees
Identify most critical potential errors.
Effects of changes: There was a 7-fold increase in near miss reporting. Using this, perioperative management developed a systematic method to prioritize improvement efforts. With approximately 1541 system-wide reported near misses, process/organizational changes occurred through PI initiatives.
Lessons learnt:
Listen to stakeholders.
Encourage a non-punitive atmosphere for PI
Get physicians and staff buy-in
Simplify tools to encourage increased reporting
Create real-time reports for real-time solutions
Tailor the tool to hospitals’ culture
Establish Good Catch monthly reporting to communicate improvements.
30. REDUCING NOSOCOMIAL INFECTIONS IN NEONATAL INTENSIVE CARE
1,2S Craig, 1,2E Rogers, 1E McCall, 1F Alderdice, 1J Jenkins. 1Neonatal Intensive Care Outcomes, Research & Evaluation (NICORE) Group, Queen’s University Belfast, 2Royal Maternity Hospital, Belfast
Problem: Nosocomial infection is associated with increased mortality and morbidity in very low birth weight (VLBW) infants. Poor hand hygiene is a modifiable risk factor for nosocomial infection. The project aims were to: (1) reduce nosocomial infection rates in VLBW infants; and (2) increase knowledge of evidence-based hand hygiene guidelines and use of alcohol-based gels.
Context: A prospective multi-professional collaborative quality improvement initiative was undertaken in five neonatal intensive care units in Northern Ireland.
Assessment of problem: Line-associated laboratory confirmed blood stream infection (LCBSI) rates were obtained prospectively using the National Nosocomial Infection Surveillance (NNIS) protocol for high-risk nursery patients.
Intervention and measurement of improvement: Quality improvement interventions involved: (1) presentation of evidence-based hand hygiene guidelines; (2) display of new infection related posters; and (3) individual assessment of hand hygiene with the aid of a GloGerm™ kit. LCBSI rates were ascertained 6 months after the interventions. Changes in knowledge, attitudes and personal practice of evidence-based hand hygiene were determined, using questionnaires, completed during pre- and post-intervention periods.
Results: Line-associated LCBSI rates fell from 25.3 (n = 31) to 19.3 (n = 19) episodes per 1000 central venous catheter days with wide inter-unit variation. Questionnaire analysis revealed that knowledge of the 6-step hand decontamination technique increased from 63% (n = 88) to 94% (n = 132) and that use of alcohol-based gels in clinical scenarios increased significantly (domain scores increased from 40.4 to 54.9; change of 14.5 (95% CI 9.7 to 19.3), p<0.001, paired t test).
Lessons learnt and message for others: Appointing an individual with clinical credibility (i.e. a neonatal nurse) and close involvement of key multidisciplinary links in each unit ensured reliable data collection and successful implementation of the hand hygiene interventions. These are essential to success in multi-centre quality improvement initiatives. Continuous focus on hand hygiene will be necessary to sustain improvements.
31. IMPLEMENTATION OF AN AUTOMATED PRESCRIPTION SYSTEM TO REDUCE MEDICATION ERRORS
AB Jiménez-Muñoz, A Muiño-Miguez, C Sanchidrián, S Monge-Corella, M Sanjurjo, MP Rodriguez-Perez. General University Hospital Gregorio Marañón, Madrid, Spain
The setting for this study was a 1800 beds Spanish General University Hospital with 5000 workers which is divided into several institutes.
Since 1998, when the report “To err is human” was published, to build a safety culture has become a priority at hospitals all around the world. Regarding the sanitary practice-related adverse events (AE), medication errors (ME) are the most prevalent problem.
A prospective study was carried out in an internal medicine department, to determine the rate and type of AE derived from medical assistance. Estimated rate was 3.9 patients per 100 patients-day (CI 95% 2.4 to 6.06), the majority being ME (38.5%).
An automated prescription system was implemented to decrease ME. An intense training was needed and was offered by the pharmacy department to physicians and nurses. Due to the high costs of the system, we wanted to confirm its utility to avoid AE before expanding it to the whole hospital.
Departments using traditional prescription and transcription were compared to departments with automated system. For data collection, clinical records of selected patients were reviewed, gathering notes about ME. Direct observation of administration was executed, the observed nurse ignoring the purpose of the study. To avoid biases, observers accompanied nurses attending their work, describing exactly what had been done and later comparing gathered notes with transcription, if existing, or otherwise with prescription. The clinical impact was assessed by experts.
As shown in the table, errors decreased in every phase of the medication process. The same table shows the impact of detected errors, which was evaluated following NCC MERP classification. Impact for patients was less serious with the automated system.
With the automated system, ME are decreased and, when occurring, impact for the patients is reduced. In the future, additional drops in ME rates are expected as a consequence of completely eliminating transcription related errors.
32. SERIOUS ILLNESS, RECOGNITION AND RESPONSE
IJ Kirby. Southport and Ormskirk NHS Trust, UK
This work took place in an NHS Acute Trust serving 240,000 people. A review by the Trust Medical Director identified eight hospital inpatients over a 5 year period who had suffered an unexpected adverse outcome. A commonality was that their deteriorating clinical condition had neither been recognised, nor treated promptly. The Trust established a Working Party chaired by the Trust Clinical Lead for Risk (the author) to investigate these cases, to recommend change in working practices to achieve rigorous and robust monitoring and management of inpatients with serious illness, and to implement the process of change. The Working Party, commissioned by the Chief Executive, comprised senior medical, nursing, and managerial staff, together with a Trust non-executive director. Thus the Working Party had a mandate and the necessary authority to implement change. It recommended the introduction of monitoring physiological observations in all patients at least twice per day, a new Early Warning Score (EWS) chart, a rigorous escalation policy involving early consultant notification of deterioration in a patient’s condition, and the introduction of detailed explicit handover charts for the transfer of patients to different wards within the Trust. A sustained programme of education was initiated, directed at both nursing and medical staff. This teaching was included as part of mandatory induction training for new staff. The Working Party continued to meet two monthly to review audits of the new working practices. The audits have demonstrated that the recommended changes have been successfully established, resulting in a considerable improvement in practice. EWS charts were previously completed correctly in 33% of cases. This has now improved to over 80%. We discovered that significant change can be introduced successfully in a large organisation, if it is enthusiastically supported by key senior personnel from different departments working together as a team.
33. INCORPORATION OF USERS’ VIEWS IN COLORECTAL CANCER PATHWAY IMPROVES SERVICE PROVISION
DM Latham. University Hospital of North Staffordshire
User involvement has been a key theme in recent national policy, and is an important factor in developing patient pathways for benign and malignant disease. Traditionally healthcare providers assumed that patient needs were based on professional standards and assessment, but an increasingly competitive health care environment has placed emphasis on patient satisfaction.
Patient focus groups were undertaken at a university hospital cancer centre by the colorectal cancer multidisciplinary team. Patients who had previously undergone colorectal cancer surgery were invited to attend a patient party where focus groups would be used to audit the patient perception of the current pathway; 60 patients attended the event. The aim of the audit was to improve future services for patients, carers and health professionals, by using emergent themes to change practice in line with user recommendations.
Focus group methodology, using trained facilitators, was chosen as the best way to gather maximum information on a given topic in a limited amount of time. Topic guides on diagnosis and investigation, inpatient stay and postoperative follow up care generated a wealth of information. Verbal feedback from the groups took place at the end of the evening to clarify emerging themes. A written action plan formulated following the event using the information gathered provided the impetus to change and clarify practice for the following year.
Following the inaugural meeting in 2001 the patient party is now a successful annual event. These events generate a wealth of information, with health care professionals being surprised at many of the process changes suggested by users. The formulation of an action plan ensures the team addresses the concerns of patients, and re-evaluation of the action plan at subsequent events evaluates how successful the action plan and changes made have been.
34. “THE RIGHT PERSON, THE RIGHT PLACE”: MODIFIED EARLY WARNING SCORING SYSTEM (MEWS)
C Lewis. Bro Morgannwg NHS Trust, Bridgend, UK
The introduction of a Modified Early Warning Scoring System, to assist staff in the early recognition and management of the acutely ill patient and those at risk of deterioration, has reduced the number of cardiac arrests by 21% annually, averted admissions to the intensive therapy unit (ITU), supported a more timely admission to intensive care, and assisted in appropriate “do not attempt to resuscitate” orders.
The aim of the Early Warning Scoring System is to educate and empower all ward based clinical staff in the early recognition and management of the acutely ill patient and those at risk of deterioration, as it has been suggested that staff within general clinical areas lacked knowledge and skill to manage the acutely ill patients, thus resulting in suboptimal care.
The Early Warning Scoring System was initially piloted within specific medical wards at Bro Morgannwg NHS Trust for a 3 month period. The project team worked in partnership with ward based multidisciplinary teams to ensure ownership from all involved and a multiprofessional education programme was developed. The Outreach nurse visited the wards daily to review the identified at risk patients and to follow up patients discharged from ITU.
Following the pilot programme for MEWS there was a number of benefits identified which included a reduction in cardiac arrests by 21%; also, of those patients reviewed within the general ward, 70% had an improvement in condition. As a consequence it was decided to fully introduce MEWS across the Trust in all acute clinical areas.
Summary of results/lessons learned: It is evident that the introduction of an early recognition tool can empower staff and assist them in the early identification of the at-risk patient. It has had a significant impact on patient outcomes and ensured that the acutely ill patient is managed appropriately.
35. WARD MODERNISATION PROJECT
LS Bevan. Bro Morgannwg NHS Trust, UK
A 6 month modernisation project was undertaken on an acute medical ward in an integrated NHS Trust.
An observational study was carried out at the start of the project which was designed to explore provision of service delivery and workforce practices. This provided a detailed picture of the working day and identified areas of best practice and key services that could be improved or redesigned.
PDSA cycles were employed as a method of identifying, testing and evaluating innovations. The ward team was encouraged to keep “work cards” to stimulate debate around their ideas for change.
Resulting changes included:
The re-design of a Healthcare Assistant role into a Housekeeper role
The application of LEAN principles to the environment with de-stocking of ward stores
A change in shift pattern to meet patient need
The introduction of protected mealtimes
The introduction of protected medication rounds
The introduction of a patient dependency and acuity tool which facilitated electronic handover.
Effects of the changes included:
The Housekeeper role ensured that the environment was kept de-cluttered and stores were closely monitored
The average length of time for the medication round reduced from 90 to 65 minutes. Improvement in patient drug charts was demonstrated through audit
Patients were able to eat in a relaxed, uninterrupted environment and nurses were available to support nutrition
Staff morale improved and sickness levels decreased
There was a reduction in complaints received.
The lessons learned from the initiative were:
When embarking on any modernisation project, ensure a high performance team is chosen to ensure the focus of the project is maintained
The Project Manager needs to be detached from the project site and have project management experience and qualifications
The focus of the project needs to reflect the time-scales for delivery.
36. A LARGE SCALE IMPLEMENTATION OF LEAN SIX SIGMA AT THE HOSPITAL GROUP OF SKARABORG (SKAS) IN SWEDEN
1S Lifvergren, 2B Bergman. 1Hospital Group of Skaraborg, 541 85 Skövde, Sweden, 2Chalmers University of Technology
The Hospital Group of Skaraborg (SkaS), situated in the Western Region of Sweden, consists of four hospitals and serves a population of 260 000. The care offered includes acute and planned care in a large number of specialities.
Strategy for change: SkaS has implemented a strategic Lean Six Sigma initiative since 2005. So far, 35 black belts working half-time with improvements have been trained/are in training. The clinics at the hospital identify critical areas to improve in their care processes. Every project is lead by a black belt with support from cross-functional teams as well as a steering committee consisting of managers responsible for the process to be improved. The systematic solving process in Six Sigma—DMAIC—is used. Every co-worker and manager with a role in the project receives a 3 day education in Lean Six Sigma methods. Identified solutions to quality problems are implemented using a method of iterat<~!?show=[fo]?>ing PDSA cycles. Permanent networks are used to share lessons learnt.
Effects of changes: So far, the program has produced sustainable results in many processes; 25 improvement projects have been completed, most of them with successful results—for instance, reducing variation in warfarin treatment, reducing haemolysis in blood tests, lowering HbA1c in patients with diabetes, reducing unnecessary cancellations of orthopaedic operations, reducing unwanted variation in hours used for supervising suicidal patients, and so on. Ten more projects have now started in 2008.
Lessons learnt: Lean Six Sigma approaches can be successfully translated to different healthcare settings. The fact based and result driven problem solving roadmap creates enthusiasm and stimulates everyday improvement.
37. DESIGNING EXPLICIT CRITERIA TO CONTROL THE QUALITY OF OUTPATIENT ELECTRONIC PRESCRIBING SYSTEMS IN FRANCE
1P Liot, 1M Toussi, 1I Anglade, 2G Simon, 1H Nabarette. 1Haute Autorité de Santé, 2ESIRIM
Context: The Haute Autorité de Santé (HAS) is the qualified body to design a voluntary certification procedure for electronic prescribing systems (EPS) in France. There are currently about 100 EPS for ambulatory medicine in France. They are thought to improve prescription quality and safety, but there is no procedure to assess this.
Strategy for change: A working group made up of experts in pharmaceuticals and medical informatics, users, and companies producing EPS was convened at HAS. The group discussed the minimum requirements of an EPS in ambulatory care. A DELPHI method was used to assess (i) which functions improved prescription safety, (ii) facilitated the work of the practitioner, (iii) helped contain costs, and (iv) to consider the feasibility of developing these functions. During the sessions, several aspects of EPS were considered, such as the administrative rules of a prescription, disease and drug coding, patient records, co-existing disease and allergic conditions, contraindications to drugs, drug interactions, dosing and the use of an international non-proprietary name for prescriptions. Draft criteria were sent to peer reviewers for their comments. A total of 72 criteria were finally selected. A second working group designed patient scenarios based on these criteria for use by the certifying bodies for the quality control.
Lessons learnt: Some brands of EPS were tested during test development. Each test was successfully passed by at least one EPS. However, no EPS passed all tests. The ability of EPS to detect contraindications, drug interactions, and aspects such as drug prices depended on the quality of pharmaceutical databases (PDBs). The EPS and PDB therefore need to be assessed together as a dysfunction in the PDB induces a dysfunction in the EPS. We thus drew up a code of practice for PDBs. PDB publishers will have to agree to apply the code for PDBs before prescription software can be certified.
38. BETTER ALZHEIMER CARE IN THE WEST OF SWEDEN 2007: A BREAKTHROUGH PROJECT IN THE CITY OF GOTHENBURG
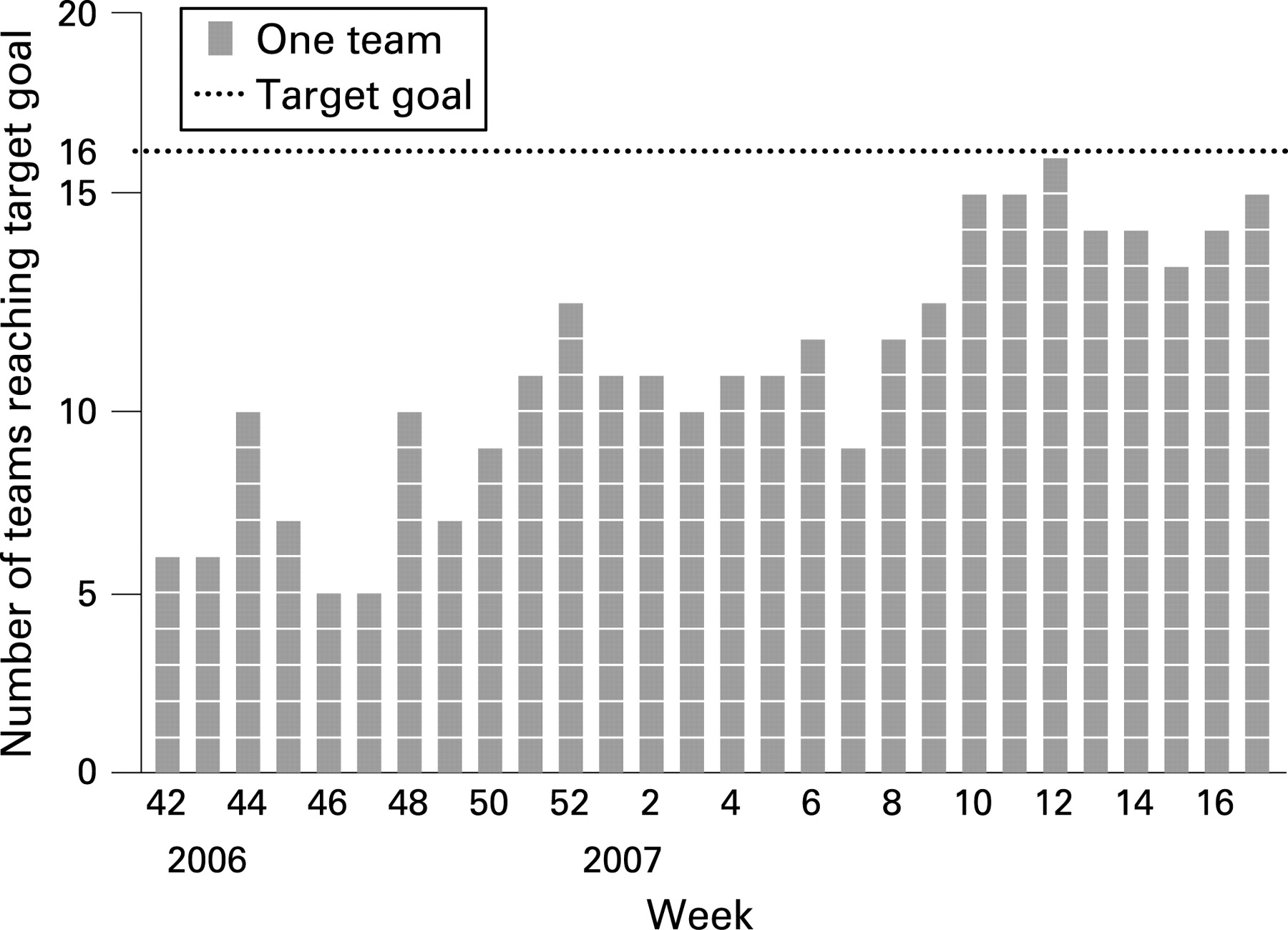
M Ljung, S Landhage. Göteborg, Sweden
Better caring, calmer environment and less sedative medication gave a higher quality of life for elderly with Alzheimer’s. With many small changes we achieved big improvements!
The breakthrough series is a time-limited method for spreading and adapting existing knowledge in a sustainable manner and to achieve a common goal. The so-called PDSA circle (Plan, Do, Study, Act) forms the basis for the improvement work.
Starting in 2006, 20 teams from the city of Gothenburg and one neighbouring community, worked for 7 months with the “Better Alzheimer care in west of Sweden” project, using the “Breakthrough series method”. During the project 327 changes were tried and 247 of these were made permanent routines. 80% of the teams reached one goal where subjects reduced anxiety. 90% of the teams experienced marked improvements and sustainable system changes due to the improvement work.
The improvement work was performed in the community care homes and in the home-help service for the elderly. The focus population was elderly with Alzheimer’s. Each improvement team included four individuals of different occupational groups and was supported by a supervisor. The teams identified problems and formulated their own objectives. They also decided on measurements, tested ideas, follow-up and reported monthly results. On three occasions, the teams met in seminars to exchange experiences. The results were eventually presented as case studies at a conference.
All teams changed their way of thinking i.e. they experienced improved teamwork, better cost efficiency and the elderly clients expressed satisfaction with the improvement work. Many improvements affected the elderly with Alzheimer’s directly by showing decreased anxiety, calmer environment, better caring and social stimulation. Less medication needed and fewer falls due to better care were also noticed.
39. QUALITY IMPROVEMENT IN RENEWALS OF PRESCRIPTION WITH ROHTO-WORKSHOPS IN HELSINKI
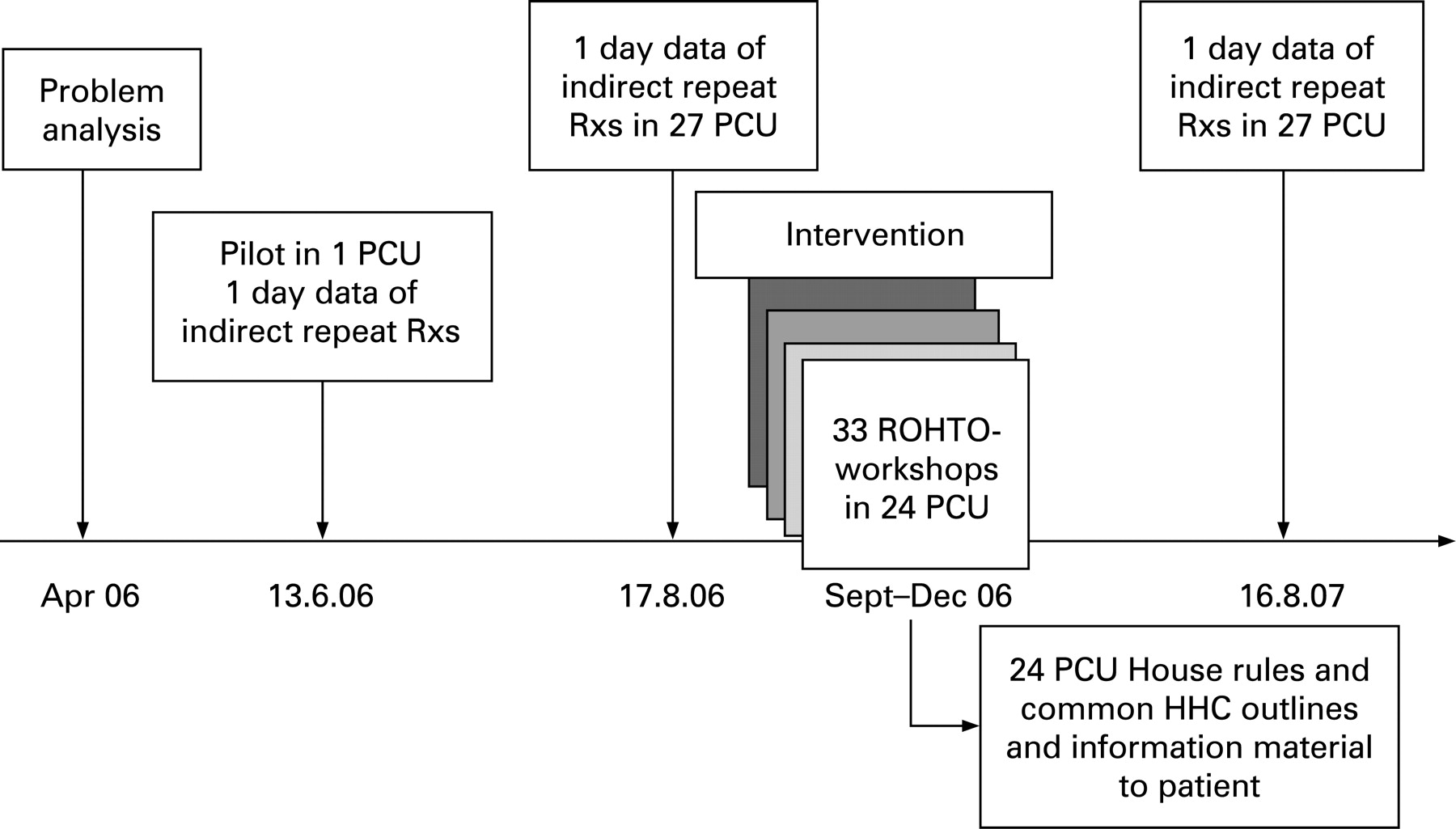
1M-L Lommi, 1R Mäkinen, 1A Helin-Salmivaara. 1Centre for pharmacotherapy development ROHTO, Helsinki, Finland
Background: The Helsinki Health Centre (HHC) provides public primary health care services for 560 000 inhabitants. The HHC is divided into 27 primary care units (PCU), employing over 300 GPs and 800 nurses or receptionists. Repeat prescriptions (Rxs) are often issued without personal doctor–patient contact (indirect repeat Rxs).
Problem: The large number of repeat Rxs without clear renewal process cause extra work load and include medication safety risks.
Objective: Workshops were created to clarify and harmonise the renewal process, to improve patient information on renewal, and to promote GPs to renew Rxs during consultations.
Intervention: In 24 PCUs altogether 33 multiprofessional workshops were organised by a trained facilitator pair (GP–nurse) from the PCU during autumn 2006. In total 242 GPs and 430 nurses or receptionists participated in the interactive workshops which lead to house rules and patient information material specific to PCU. Some general outlines could be agreed by leaders of the HHC, and were implemented to PCUs by facilitators. To inform inhabitants some articles on repeat Rxs were published in local newspapers.
Method: In every PCU the renewal process was explored among facilitators with a structured questionnaire, and the quantity and quality data of indirect repeat Rxs and individual guidance of patients was collected before the intervention during 1 day. Evaluation was repeated 1 year after.
Results: The number of indirect repeat Rxs decreased from 1713 to 1532 (−10.6%). Personal guidance of patients increased by 49% and availability of information leaflets increased from 5/27 to 27/27 of the PCUs. The variation in maximal delay of the renewal from 3 to 12 days was harmonised to 1 week in every PCU.
Conclusion: Interactive workshops facilitated by trained GPs and nurses can be used to effectively develop practices in primary health care—for example, practices in repeat Rxs.
40. SECURITY IMPROVEMENT OF THE MEDICATION CIRCUIT AT THE REINE BLANCHE CLINIC
1N Mabs, 1R Huguet, 1C Aigret, 2H Laborie, 3F Debouck. 1Cardiology Department, Reine Blanche Clinic, Orléans, France, 2MEAH: Mission d’Expertise et d’Audit Hospitalière, Paris, France, 3Air France Consulting
Context: The Reine Blanche Clinic is one of the eight volunteer institutions selected by the MeaH to work towards greater medication safety.
Assessment of problem: According to the Ministry of Health, the number of serious medication-related incidents is estimated at 1.4 per 1000 days of hospitalization.
Only in its infancy, the “positive culture” of error is based on voluntary reporting, analysis and the implementation of resources to avoid repeating errors in health care institutions.
Reine Blanche Clinic chose to develop a risk management program based on incident reporting, systemic analysis and corrective action implementation inspired by methodologies used in the aeronautic field. The two main objectives were:
increasing the number of reported incidents
working upstream of incidents in order to avoid recurring errors.
Strategy for change: First, management signed a non-punitive commitment statement that it would not punish the informants.
A Feedback Committee was set up with the assistance of outside aeronautic consultants. Comprised of doctors, nurses, pharmacists, pharmacy employees and managed by consultants, this Committee met on a monthly basis and selected a “undesirable incident” from the volunteer departments to analyze and suggest corrective actions.
Results of assessment: Constant increase in the number of reported events: 0 in 2005, 52 in 2006, 123 in 2007.
A climate of trust has been built through the objective reduction in anonymous reporting from 80% to 12%.
20 Feedback Committees gathered in 2007
18 treated incidents
41 corrective actions
90% of these actions realized in due time
Lessons learnt: With a structured method, removing the guilt attached to mistakes and using error to improve practices is indeed possible.
41. NURSES’ KNOWLEDGE AND ATTITUDES ASSOCIATED WITH NEAR MISSES: EVALUATION OF THE IMPACT OF A KNOWLEDGE TRANSFER INTERVENTION FOR PRESSURE ULCER PREVENTION & CARE
K MacMillan, L Jeffs, D Affonso, C Kennedy, L Dacres, J Kim, L Korkola, V Sivanantham. Humber Institute of Technology & Advanced Learning and University of Toronto, Toronto, Canada
As part of a larger project funded by the Ontario Ministry of Health on “near misses”, we investigated a knowledge transfer intervention for evidence-based wound care in three complex continuing care (CCC) units among a sample of 8 late career staff nurses (LCIs) and 223 nursing colleagues. Effective pressure ulcer (PU) prevention and wound care is an example of a “near miss” activity. An existing wound care curriculum was translated to an on-line education program plus clinical mentoring by expert nurses for 8 LCI nurses (active intervention). The remaining CCC nurses had no active intervention. Identical pre-test and post-test questionnaires on knowledge and attitudes regarding pressure ulcer prevention and treatment were administered to the entire population of nurses, 11 weeks apart, and a focus group was held with the LCI nurses at the end of the experience. LCI nurses significantly increased their scores on all survey sub-scales and the total score (p<0.05). CCC nurses showed no significant differences in scores, except on the Ulcer sub-score. Active intervention of the wound care course with the LCI group resulted in increased knowledge, but Passive intervention (diffusion of the information from the LCI to staff nurses) did not substantially increase knowledge scores. Although quantifiable changes in practice were not examined, the LCI nurses qualitatively described changing their own practice in ways that benefited patients and their colleagues. They recognized “near misses” and acted to prevent them. Simply placing “content experts” onto units, with limited time and resources, did not increase the knowledge of colleagues’ community of practice as measured by the survey tool. Knowledge translation strategies should be considered to maximize evidence based practice for PU “near misses” with all nursing staff. A structured on-line learning program may benefit knowledge transfer and change in practice.
42. NATIONWIDE PERFORMANCE MEASUREMENT CAN IMPROVE THE QUALITY OF CARE
1JB Mainz, 1A-M Hansen, 2P Bartels. 1Aalborg Psychiatric Hospital, Department South, Aalborg, Denmark, 2The National Indicator Project, Olof Palmes Alle, Aarhus, Denmark
Outline of context and problem: This study is based on data from the Danish National Indicator Project (DNIP). Evidence based disease specific quality indicators have been developed by multiprofessional clinicians appointed by the scientific societies for seven diseases: stroke, diabetes, hip fracture, schizophrenia, acute gastrointestinal surgery, heart failure and lung cancer.
Assessment of problem and analysis of its causes: Quality indicators have been implemented in all Danish hospital units. Participation is mandatory for all relevant clinical departments treating patients with the seven diseases. The data elements for quality indicators are collected specifically as part of the project for all patients.
Strategy for change: Structured audit processes have been implemented by audit groups consisting of clinicians at national, regional, and local levels, both to explain the risk-adjusted results and to prepare implementation of improvements.
Measurement of improvement: Each department receives results every month to enable continuous evaluation of their performance. The case-mix-adjusted data for each participating department, together with a short summary of audit comments, is released publicly.
Effects of changes: Results from 2004–mid 2007 for 6–10 evidence based quality indicators related to the respective diseases show improvements for the individual indicators between 10–15% on average per year. The percentages of patients that received all relevant interventions as described by the process indicators increased from 2004 to 2006 between 7 and 40. These changes were statistically significant.
Lessons learnt: The results of this study indicate that systematic nationwide performance measurement emphasising continuously feedback to multiprofessional clinicians, followed by systematic national, regional and local audit processes, in order to implement interventions in clinical practice and public disclosure of quality data can improve the quality of care for specific diseases.
43. TRANSFORMING FLOW, TRANSFORMING CARE: APPLYING LEAN METHODOLOGIES TO ONE OF CANADA’S LARGEST TEACHING HOSPITALS
M Caesar, A Ko, MK McCarthy. University Health Network, Toronto, Ontario, Canada
A major Toronto, Ontario healthcare landmark, University Health Network (UHN) has served the Canadian community for over 200 years. Comprised of three hospitals (Toronto General, Toronto Western, and Princess Margaret), over 11,600 staff, and seven major programs, UHN has the largest Canadian hospital-based research program and is a teaching facility affiliated with University of Toronto.
In 2006, UHN began an enterprise-wide initiative, focusing on patient flow, access and wait times in emergency departments (ED), general internal medicine (GIM), operating rooms (OR), palliative care and medical imaging.
Multidisciplinary teams of frontline, administrative and project management staff worked synergistically with management, learning and applying Lean methodologies and principles to drive change.
The teams used baseline data for gauging current state and determining targets. Targets were based on government objectives, hospital goals and measured area capabilities.
Each area completed a Value Stream Analysis, mapping patient flow and developing an improvement plan aimed at standardizing work, defining and tightening hand-off points, increasing process transparency and eliminating non-value-added activities for patients.
Rapid Improvement Events allowed teams to diagnose issues, design, test, and implement solutions quickly. Evaluation and sustainability efforts included regularly reviewing key performance indicators with staff, conducting management “tours”, holding formal 30, 60, and 90 day performance reviews, and having monthly “continuous quality improvement” meetings to review change efforts utilizing the “A3” problem solving framework.
Some outcomes included:
47% less time required to admit next patient from ED after GIM discharge;
59% less time required for initial ED nurse review of patient chart;
83% increase in OR case cart completeness;
33% more CT patients being seen on time;
50% less time to discharge home or to a palliative care unit.
Lessons learned included early definition of targets and baselines, ensuring senior management buy-in and commitment, and open communications with all staff.
44. EVALUATION OF THE IMPLEMENTATION OF AN ELECTRONIC INCIDENT REPORTING SYSTEM AIMED AT IMPROVING REPORTING PRACTICES IN A LARGE TEACHING HOSPITAL
P McKernan, C Hayes, J Copeland. St Michael’s Hospital, Toronto, Canada
St Michael’s Hospital is a large (550 bed) urban hospital affiliated with the University of Toronto. We undertook an assessment of our adverse event reporting infrastructure in an attempt to improve the culture of reporting.
A cross-sectional organisation-wide assessment of the reporting system, user and system needs was done. 86% of the workshop participants agreed or strongly agreed that the paper based incident reporting system was ineffective. The hospital incident reporting policies and procedures were revised. An electronic incident reporting software was implemented hospital wide.
Incidents reporting for inpatients areas increased from 32.0 reports/10 000 occupied bed days in the baseline period to 68.8/10 000 after the intervention (36.8 additional reports/10 000 occupied bed days). The post intervention adverse event (AE) rate for the hospital compared to the Canadian Adverse Event Study (Baker et al, 2004) was 5.5 compared to 7.5 per 100 hospital admissions.
Analysis of AEs, by degree of severity out of the total reported compared to teaching hospitals in Canada, showed greater variability (see table).
Based on current incident reporting rates, death would be associated with an AE in 0.017% of patients at St Michael’s Hospital compared to 1.11% of patients in other teaching hospitals in Canada (95% CI 0.1% to 2.59%)
The introduction of an electronic incident reporting tool can increase the reporting culture. Other methods for the measurement of harm are needed in order to validate the sensitivity and specificity of this method of AE identification.
45. THE SAFETY OF THE JOURNEY: REDUCING THE RISKS OF INTERFACILITY TRANSPORT OF CRITICALLY ILL CHILDREN
1M Montgomery, 1D Lutman, 1P Ramnarayan, 1B Sims, 1E Polke, 1S Revanna, 1S Agrawal, 1A Petros. 1Children’s Acute Transport Service for North Thames, London; 2St John Ambulance Service, London, UK
Between November 2001 and November 2005 our dedicated paediatric retrieval team, the Children’s Acute Transport Service (CATS), performed over 5000 critically ill child transports, and was involved in three (0.06%) serious motor vehicle accidents, some with injury to staff. At the time, standards used by CATS to transport critically ill children were similar to those set by other major ambulance services and retrieval teams, including the use of exemptions (passing through red lights; exceeding the speed limit) with blue lights and sirens (L&S) both outward (en route to the child) and inbound (with the child to the receiving paediatric intensive care unit). Following a road traffic accident in March 2004 routine use of emergency driving techniques was suspended for a period of 3 months. Strategic review was performed to determine current safe practice and areas for improvement. A transport time study was undertaken to determine time delays without the routine use of L&S.
The strategic review highlighted a lack of available worldwide expertise in the field of interfacility transport safety. Potential areas of risk and intervention were identified. A bespoke system of safe practice for interfacility transport of critically ill children was developed with wide ranging interventions in many areas of practice, including driving technique, team mobilisation, triage, use of restraints, equipment and vehicle design (see fig). Other areas were developed in parallel in order to facilitate safe practice including education, outreach and networking, and communication. The process was multidisciplinary and continuously audited.

We report on this continuous quality improvement process, with particular emphasis on the rationale behind the decision to use L&S and the introduction of a triage system, the need for driver training in interfacility transport, safe practice by the team in the ambulance, and equipment and vehicle design modifications.
46. THE USE OF E-LEARNING IN PATIENT SAFETY EDUCATION
1K Nakajima, 2H Takeda. 1Department of Clinical Quality Management, Osaka University Hospital, 2Department of Health Information and Science, Osaka University Hospital, Japan
Outline of problem: For patient safety education, attendance of hospital employees at seminars has been mandated by Japanese healthcare regulations since 2001. Questioning the efficacy of this method, we have introduced a new educational approach by using e-learning at Osaka University Hospital (1076 beds).
Assessment of problems: Limitations of the seminar-style education that we have experienced comprise poor attendance seminars due to busy practice or work schedules, mismatch of educational contents to different professional disciplines at a single seminar, repeated occurrences of similar incidents, time-consuming checking of attendance, and difficulties in evaluating effects on learning as well as obtaining attendees’ feedback.
Strategy for change: The Patient Safety Committee decided to introduce an e-learning system via the hospital intranet. With hospital-wide collaboration, a set of quiz questions about basic clinical knowledge and a simulative animation about communication skills among health care providers were developed. A trial run was launched in December 2006 for physicians and nurses with repeated pre-announcements through Clinical Risk Managers.
Effects of change: During the 7 month period following the launch, 10% of the potential subjects took part in the quiz with an average score of 80 points out of 100. Only 5% studied the simulative animation and approximately 80% of the respondents answered they “enjoyed learning the content”, “want to apply it in their practice”, “gained new knowledge” and “think it would be effective in actual practice”.
Lessons and messages: Use of e-learning for patient safety can provide a more appropriate educational environment for busy clinicians, easier evaluation and tracking of the learners, and more appropriate educational contents for specific disciplines. It will be necessary to obtain additional budgets and personnel for ongoing system management including frequent updating of the employees’ list, as well as the development of contents and educational management.
47. THE FIGHT AGAINST MALNUTRITION AT THE VEXIN HOSPITAL CENTER
1M Noah, 2D Le Spegagne, 2D Talandier. 1Vexin Hospital Center, France, 2MeaH, France
The Vexin Hospital Center (400 beds of which 195 are dedicated to dependent elderly persons) has a catering service that serves 900 meals per day. A survey of the nutritional state of all patients was conducted in September 2006 and showed a high rate of malnutrition (between 22–90% depending upon the department). In fewer than 3 months, three major assessment axes were defined as to the food preparation:
axis 1: better understanding of patient expectations and in particular those of the elderly
axis 2: decompartmentalise occupational fields
axis 3: better fighting against malnutrition by adapting production to the current nutritional imperatives.
Three actions were undertaken:
return to homemade soups/change from an industrial quality bread to wholesome bread/create an additional choice for the elderly patients who want to replace their main dishes with a protein-rich substitute (savoury pies, assortments of deli meats and cheeses, etc) closer to their usual eating habits;
take into account the socio-cultural dimension of the meal by allowing the patients to visit the kitchen and introducing genuine collaboration between the caregivers and the kitchen staff;
making of protein-enriched desserts (bavarois, mousses, crèmes, stewed fruit, cake, etc) as part of the menus and not added to meals as supplements.
As a result:
dinnertime was pushed back from 6 pm to 7 pm in all units, significantly reducing night fasting, hence the risk of denutrition;
improved interaction between the cooks and care givers;
progressive shift towards a more united cooking staff who rediscovered greater meaning in their jobs and whose work is recognised and valued;
introduction of regular evaluations of the food service; one satisfaction survey per year; one consumption survey every 2 years.
48. IMPROVING CHILD HEALTH IN NICARAGUA
O Nuñez. University Research Co, LLC/USAID Health Care Improvement Project
Context: Since 2003, the Ministry of Health of Nicaragua has implemented a national Paediatric Hospital Improvement Collaborative with technical support from USAIDs Quality Assurance Project (now, USAID Health Care Improvement Project). The collaborative, which now includes 16 maternal-child hospitals (73% of those in Nicaragua), aims to improve care of children with serious infections or severe malnutrition. Before 2003, Nicaragua lacked national guidelines for management of critically ill children.
Change strategy: The WHO Referral Care Manual was adapted to Nicaragua and standards and indicators defined to monitor quality of hospital paediatric care. Hospital teams conducted self-assessments of compliance with standards to identify gaps. Changes implemented by QI teams formed at each hospital: instituting triage in emergency services, assessing client satisfaction, making lab tests and essential drugs available in each consultation area, and initiating active communication between the hospital and primary health centres to referral and counter-referral. In-service training centres were created to build staff competency in management of acute paediatric illnesses through short rotations. Hospital teams competed in “Prize for knowledge” contests that gave prizes (electric fans, coffee makers, etc) based on correct response to clinical management questions.
Measurement: Each hospital’s improvement team audits clinical records monthly to monitor nine indicators related to care processes and one related to availability of inputs. Initially, teams had difficulty collecting data systematically, but now monitoring is a routine. Not all hospitals continue to collect monitoring data.
Effects: The 12 hospitals reporting have documented sustained compliance with clinical standards and a reduction in number of deaths from key paediatric conditions, particularly pneumonia and respiratory distress syndrome (55% and 32% declines, respectively, comparing data for last 2 years (see fig)).
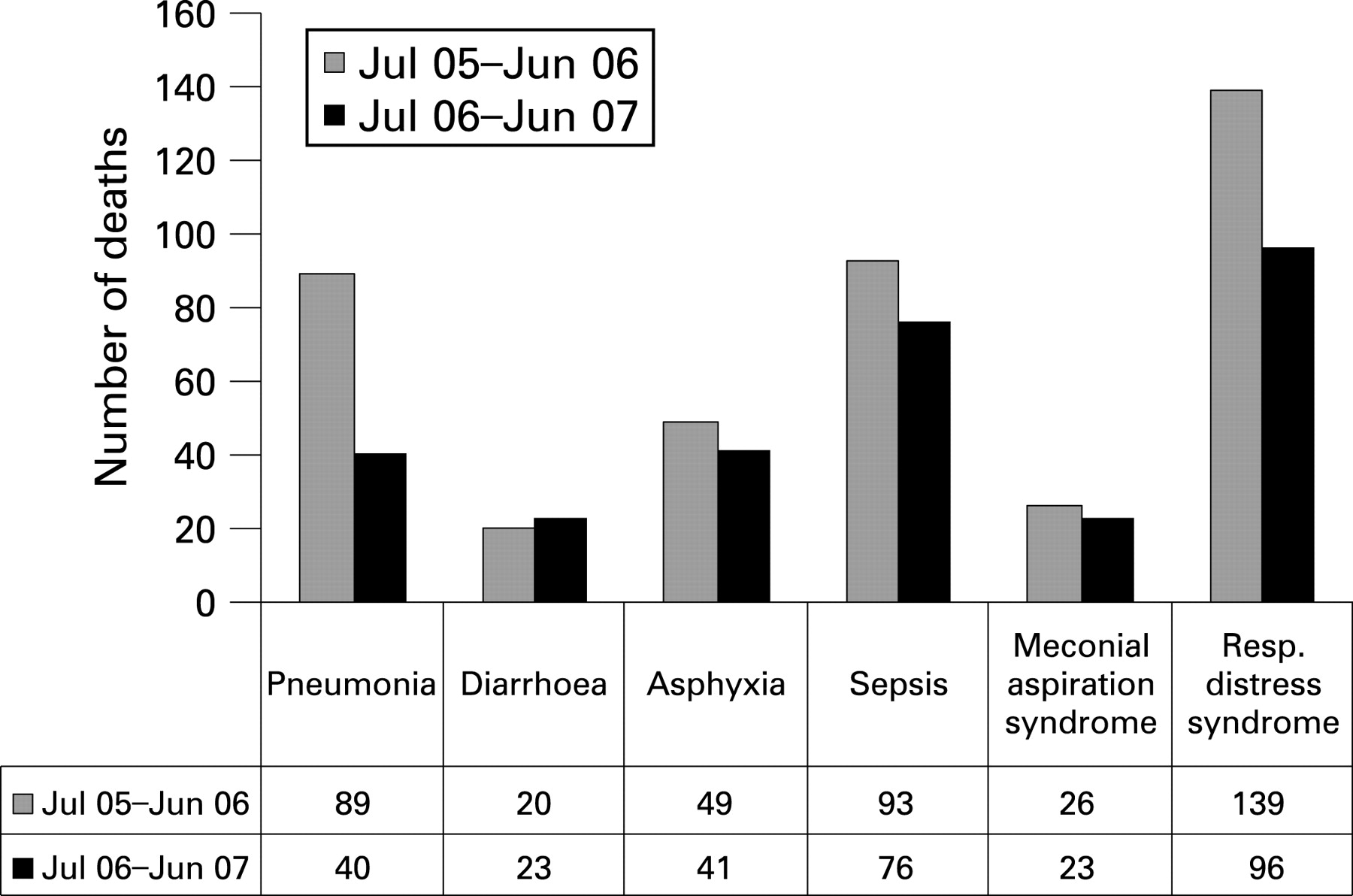
Recommendations: Improvements in content of care need to be balanced with more child-friendly care, and incentives are needed to reward and encourage quality champions.
49. IMPLEMENTING A UNIT-BASED SHARED GOVERNANCE MODEL OF LEADERSHIP ON A SPECIALISED BLOOD AND MARROW/ONCOLOGY UNIT
R Pascua, K Geraghty, M Saria, M Neel, C Noble, M Esser, AH Miu. University of California San Diego Medical Center, La Jolla, California, USA
The nursing shortage and the discriminative eye of the public compels the nursing profession to think innovatively of ways to reduce cost while maintaining quality care. In an effort to address this challenge, healthcare decision-makers have explored different models of leadership that will facilitate cost effectiveness and quality care. The shared governance model of leadership is one model that has been shown to foster a desirable work environment and has been associated with empowerment of nurses, job satisfaction, nursing retention, and improved patient outcomes.
This evidence-based practice project was designed to pilot a customised shared governance leadership model on a unit based level. Specific aims include: (1) facilitate the continued productivity of the unit (ie, meet the needs of the unit, its staff and patients as well as those of the hospital); (2) continue to maintain and elevate the level of quality care delivered to patients (through evidence-based policy and procedures); and (3) foster teamwork and staff development both professionally and personally (ie, empowerment of the nurses and increased job satisfaction).
This study describes the effectiveness of establishing a unit-based shared governance system of leadership on a specialised blood and marrow transplant and oncology unit. Effectiveness was measured in terms of the indicators that have been identified based on the fiscal and regulatory requirements required for each nursing unit, staff satisfaction, professional growth, and the metrics identified by the institution as documented on the balanced scorecards. Preliminary results based on indicators that have been identified revealed overall improvement.
In conclusion, we submit that a unit based shared governance model fosters a desirable work environment and empowers nurses that ultimately leads to improved outcomes based on indicators identified by this study.
50. ARE QUALITY BONUSES EFFECTIVE? EVIDENCE FROM SELECTED PHILIPPINE PUBLIC HOSPITALS
JW Peabody, O Solon, S Quimbo, K Woo, R Shimkhada. Institute for Global Health, University of California San Francisco, USA
The Quality Improvement Demonstration Study (QIDS), conducted in the Visayas region of the Philippines, evaluates the impact of two hospital-based interventions—(1) expanded health care coverage and (2) a pay for performance (bonus) scheme for hospitals—on the health status and cognitive development of children. QIDS is a randomised controlled policy experiment involving 30 public hospitals, physicians, and over 4500 children that have been followed since 2003.
The QIDS bonus scheme rewards high quality of care. Quality of hospitals is evaluated twice a year and those found to meet pre-set quality standards receive bonus payments and recognition from PhilHealth, administrator of the national health insurance program. QIDS uses a composite measure of quality encompassing physician practice, patient satisfaction, and caseload. Physician practice is assessed using clinical vignettes, a validated quality of care measure. The quality metric is computed for QIDS hospitals on a quarterly basis and issued to hospital chiefs; vignette scores are made available to hospital directors, governors, and the participating physicians. Bonuses are released quarterly.
Analyses show that bonus hospitals have higher average quality levels compared to control hospitals. In bonus hospitals, quality metric improvements were sustained through 36 months post-intervention. A slight decline in the improvement of physician vignette scores observed in the final quarter, suggests a variety of factors, including the relative smallness of the bonus, delays in payments, and limitations posed by the quality monitoring system.
An important lesson is that financial incentives are powerful instruments in quality improvement. These effects have been difficult to observe in previous studies, which are often confounded by selection and non-random assignment. An equally important observation is the impact of quality monitoring systems and feedback. Health care providers ultimately benefit from quality assessment, especially if the system is transparent and the metric is something providers can directly influence.
51. A METHODOLOGY TO DESIGN HOSPITAL CLINICAL RISK MAP AND TO INTRODUCE THE INCIDENT REPORTING
1M Pincetti Nervi, 1F Ardizzone, 1L Scotti, 2D Ripamonti, 3S Jucker, 3G Cristoforetti, 3M Meregalli, 3C Pinerolo, 4T Vitali, 5C Farina, 3M Gibelli, 6E Giubileo. 1Quality Improvement Unit, 2Emergency Department, 3Medical Area Department, 4Surgical Area Department, 5Diagnostic Department, 6Pharmacy, Ospedale S. Carlo Borromeo, Milano, Italy
Setting: General Hospital of 600 beds in urban area, 24000 discharges per year.
Objective: To approach patient safety and mistakes, through proactive behaviour.
Design: 1°: description of the principal processes; 2°: identification of critical points; 3°: identification of real risks of damage; 4°: cause analysis; 5°: description of implemented prevention/protection methods; 6°: identification of improvement opportunity; 7°: assignment of risk priority; 8°: development of improvement project for the worst risks; 9°: indicators to survey the appropriateness of the chosen tools; 10°: choice of an incident reporting form; 11°: beginning of incident reporting.
Materials and methods: We worked with 2 people per unit and developed a flow chart for each unit; we used an Ishikawa diagram; priority has been determined with 3 criteria: severity, frequency and management ability; we applied the FMECA.
Results: We found 104 general risks, plus many specific risks; every unit has identified 10 worst risks that are monitoring with one or more indicators; every unit is planning 5 improvements. The incident reporting form criteria were: identification of patient, hour of the event, setting, production stage, kind and severity of risk, description of the event, while reporting is anonymous.
Lesson learnt: The complexity of process allows us to find innumerable risks and in many cases the organisation offers some protection, but often insufficient. We believe, after this project, the health professionals are more careful of this subject than other fields of continuous quality improvement.
52. THE CHANGING ROLE OF THE NHS CEO
S Ramsden. Luton & Dunstable Hospital NHS Foundation Trust, UK
There is too much emphasis on operational performance, constantly reinforced by the wider NHS performance management culture. This has caused neglect of the really important agenda of transforming our organisations, setting ambitious improvement goals (way beyond national targets), being visible to our staff, and developing talent in our organisations.
At the Luton & Dunstable Hospital I have begun to change my role through a combination of a transformational approach, a philosophy of devolved autonomy to new Strategic Business Units and a strengthened Executive Team.
On the premise that to achieve transformational change you must first change yourself, I transferred the line of accountability for Clinical Directors from CEO to Medical Director and stopped attending the weekly Executive Team meetings. This sought to create more interdependence and independence from Executive Directors.
The time freed up has allowed me to concentrate on increasing CEO visibility to staff and on promoting the hospital nationally in accordance with the transformational vision of “Leading the NHS in patient safety”. It has allowed a greater focus on “moving the big dots” such as reducing our hospital standardised mortality rates and a strategy of “no avoidable harm”.
The NHS should take another look at the role of its CEOs. Freed from the day to day operational role, we can be more effective. If the CEO isn’t leading this transformational change, there’s a good chance no one is!
53. NATIONAL SURVEY OF INPATIENTS AND OUTPATIENTS AND THEIR RELATIVES IN DANISH PSYCHIATRY
P Rhode. Centre for Quality Improvement, Central Denmark Region
Objective: To gain detailed nationwide information about how treatment quality and contacts between relatives and psychiatric staff is perceived by patients and their relatives. The ambition is to supply information to the managerial level and at the same time to form the basis for quality improvement on local units.
Methods: In spring 2005 the staff in all wards handed out questionnaires to patients, and asked for permission to post a questionnaire to one relative. The survey included the total population of patients and relatives to obtain enough responses to report results on the local level. The questionnaires were adapted to inpatients and outpatients and their relatives, respectively. They contained 20–25 attitudinal items, a few open ended questions, and questions about socio-demographic characteristics and diagnose.
Measurement of improvement: 20,712 patients and relatives answered a questionnaire. Response rates vary from 48% (relatives to hospitalised patients) to 67% (outpatients). Patients assess their treatment more positively than relatives assess their contact with staff. Furthermore, levels of satisfaction vary a lot from ward to ward. This variation is not only due to variations in respondents’ socio-demographic characteristics and the patients’ specific diseases, but is also explained by factors such as work practices genuine to each ward.
Effects of changes: The results are published in ways that allow wards to compare their results with results of compatible wards in the region and in the whole country. Thus, each ward can identify areas where treatment and information practices can be improved. The data collection will be repeated every third year, so that wards will be able to compare their results over time. The surveys are now extended also to include child and adolescent psychiatry as well as social psychiatry.
54. CATHETER RELATED BLOOD STREAM INFECTIONS AND VENTILATION ACQUIRED PNEUMONIA IN INTENSIVE CARE: A REGIONAL QUALITY IMPROVEMENT PROJECT BASED ON A COLLABORATIVE NETWORK IN ITALY
S Rodella, S Forni, M Castagnoli, G Aldinucci, C Francone, B Rosadoni, P Angiolini, M Balestri, M Bonizzoli, M Buoncompagni, U Buoncristiano, D Calamandrei, D Calonaci, L Cubattoli, N De Feo, F Del Francia, M Feri, A Guadagnucci, D Guarducci, P Innocenti, G Lattarulo, A Lucerni, E Maglioni, P Malacarne, V Mangani, G Minelli, S Moretti, R Nassini, S Niccoli, R Oggioni, A Pedullà, C Pelagatti, A Piccioli, A Puorto, V Tucci, PL Nicoletti, G Privitera, G Bertolini. Regional Agency for Health in Tuscany, Quality Unit, Italy
Background: CRBSIs and VAP are internationally recognised crucial issues in ICU, causing prolonged LOS and fatal complications. The Regional Agency for Health in Tuscany supports a project targeted to catheter related blood stream infections (CRBSIs) and ventilation acquired pneumonia (VAP) in intensive care units (ICUs). Forty-four ICUs and 41 hospitals are involved.
Assessment of problems: Regional incidence of CRBSIs and VAP are 1.2 per 1000 central-line days and 7 per 1000 days of ventilation, respectively. User-friendly regional guidelines (RGs), standardised checklists for daily monitoring and homogeneous methods of microbiological diagnosis are needed in order to reduce variability of care processes and improve reliability of occurrence estimates.
Strategies for change: Three priorities were selected: to produce and disseminate user-friendly RGs on CRBSIs and VAP control; to promote standardised diagnostic procedures in microbiology laboratories; to implement priority recommendations in a pilot group of ICU. In 2005–2006 RGs on CRBSIs were produced and disseminated as a continuing medical education project involving almost 50 professionals; a monitoring checklist also investigating compliance to central-line bundle, was drafted in 2007, tested for feasibility in 11 ICUs and subsequently proposed to ICUs and other units handling central-lines; a set of diagnostic rules for CRBSI and VAP was defined through a consensus process involving ICU professionals and microbiologists. Drafting of RGs on VAP control is still ongoing. Implementation process will take place throughout 2008.
Lessons and messages: Process improvement can be measured through rates of RGs diffusion, checklist adoption, adherence to the central-line bundle, application of sound outcomes indicators on infections. These measures can monitor true changes in the field of common tools and language, but an effect on patient care is not yet measurable. Sharing and discussing real everyday data is a strongly effective method to involve people and build consensus; nevertheless, building consensus is a time-consuming process: waiting and pushing should be balanced.
55. PRACTITIONER ENGAGEMENT IN QUALITY IMPROVEMENT: DATA FROM THE SAFER PATIENTS INITIATIVE IN NHS TAYSIDE, SCOTLAND
RK Rushmer. The Social Dimensions of Health Institute, The Universities of Dundee and St Andrews, UK
Brief outline of context: In 2005, NHS Tayside, Scotland, participated in the Safer Patients Initiative. NHS Tayside serves 400 000 people with three acute hospitals (1216 beds), performing 35 000 surgical procedures a year. The Institute for Healthcare Improvement provided support in quality improvement (QI) methods. Multidisciplinary teams introduced evidence-based QI across professional boundaries.
Brief outline of problem: Practitioner engagement in QI is problematic. Barriers include: conviction that local services are already good; scepticism, apathy, limited time and resources; challenges to professional roles; misunderstanding of QI data and methods; difficulty in sustaining improvements within rigid systems.
Assessment of problem and analysis of its causes: NHS Tayside committed to introducing QI (tackling major causes of patient harm), planning that this would (simultaneously) facilitate practitioner engagement.
Strategy for change: Invited practitioners received training in QI methods. Small changes were initiated in their clinical areas, spread (by themselves) using rapid cycle change.
Measurement of improvement: Who led, and numbers adopting, the changes became measures of practitioners’ engagement. Follow-up interviews offered insight into continued engagement or withdrawal.
Effects of changes: Within 18 months the changes reached 50% of all eligible patients (90%+ compliance).
The change package unified multidisciplinary teams towards common goals
Local data – provided evidence that present care was suboptimal
Starting “small”: reduced practitioners’ time commitment
Modifying changes to “fit” local contexts reduced risk and increased uptake
Data practitioners collected provided feedback, prompting critical enquiry to get professionals talking (and working) in new ways
As local evidence illustrated improvement initial scepticism reduced.
Lessons learnt: Typically, nurses led the QI, with interesting exceptions. Most practitioners comply, if compliance is easy. Undertaking QI prompts culture change. Senior management may need to change hospital-wide routines to support local changes. Starting small facilitates practitioner engagement by adapting changes to local settings and managing the pace.
Message for others: QI programmes can prompt practitioner engagement and behavioural change, if “self-selectors” are supported and local data are used to persuade initial sceptics.
56. THE INTEGRATIVE ELECTRONIC PORTFOLIO: ENHANCING PATIENT SAFETY USING A NOVEL STEERING INSTRUMENT FOR SURGICAL RESIDENT TRAINING
MP Schijven, P Barach, ThJten Cate. University Medical Center Utrecht, The Netherlands
The Department of Surgery of the University Medical Center Utrecht, together with the Expert Center for Education and Training, have developed an Integrative Electronic Portfolio for surgical residents.
At present, Dutch surgical residents do not follow a standardised format for specialist training. Only a specified “number of performed procedures” is required to certify as a surgeon after completion of training. This criterion has never proven to be valid. Some persons do need more numbers to be competent in medical skills than others.
Other aspects of becoming a good clinician, such as knowledge, patient interaction and reflection of one’s own performance and attitude, is, at present, incompletely and subjectively assessed. The newly developed Portfolio is based on the canMEDS (Canadian Medical Competencies) framework, focusing on developing and assessing core competencies needed in medical specialist training. Our instrument integrates a variety of objective, validated performance outcome measurements, such as Virtual Reality simulation outcome, 360 feedback reflections, and other objective outcome measurements, together with the number of surgical procedures performed seamlessly in an online format.
VR practice results (among other outcome parameters) are integrated in the E-portfolio. This makes it possible to signal capability problems early, before they lead to hazardous patient situations.
The transparency of the E-portfolio, together with benchmarked assessment criteria and methods, are believed to optimise the curriculum, as well as reveal possible shortcomings. The Integrative Electronic Portfolio is now accepted as a national steering instrument by the Dutch National Society for Surgery, and will be implemented nationwide as of 2008.
57. BEST EVIDENCE BECOMES EVERYDAY ACTION: RESULTS FROM A NEW ZEALAND COLLABORATIVE
S Kuehl, N Coupe, E Sutich, S Scobie, J Fraser. New Zealand Guidelines Group
Suicide is a serious health issue in New Zealand. In recent years, problems identified within crisis services were a lack of collaboration between them and low adherence to best evidence practice. Hence, a nationwide Collaborative was established, modelled on an existing quality improvement programme (IHI). The New Zealand Guidelines Group adapted the implementation model by overlaying a strong consumer focus, and the Maori concept of “whakawhanaungatanga”—connected relationships and shared responsibilities between the individual, the family and the service provider. It applied the latest evidence to create and sustain change at a local level, while encouraging collaboration and learning across the health and disability sector.
The main objectives of the Collaborative were to:
improve crisis care for people at risk of suicide
promote collaboration
contribute to the knowledge base regarding methodologies for guideline implementation.
The Collaborative involved emergency departments, crisis mental health and Maori (indigenous people in New Zealand) services, as well as consumer and family advisors in 10 District Health Boards (DHB) in New Zealand. Teams at each DHB completed detailed consumer pathway maps; made systematic improvements based on The assessment and management of people at risk of suicide (2003) guideline and recent evidence; and reported monthly on four national targets.
Some of the results were:
changes of attitude towards people at risk of suicide
introduction of cultural assessments for Maori
implementation of initial assessment processes, leading to decreased waiting times
accelerated learning from the sharing of resources between DHBs.
An independent evaluation identified that DHBs would have appreciated more information up front to accelerate their progress and understanding of the methodology. Using a collaborative approach with a consumer focus and strong emphasis on supportive relationships provides an excellent basis to implement an evidence based guideline, and ultimately improve the consumer experience.
58. “WHY SHOULD I BE TREATED DIFFERENTLY?” CONTINENCE AND DEMENTIA: A SPECIALIST APPROACH TO TREATMENT
J Spencer. South West Yorkshire Mental Health Trust
Background: Incontinence in people who have dementia is often a gateway into full time care. Carers find it very difficult to manage and it is frequently cited as the determining factor in a relative or carer deciding that they can no longer cope. It can be very embarrassing for the person experiencing incontinence and the resulting behaviours can be upsetting and difficult for the carer to understand. Incontinence is often regarded as a symptom of dementia. The Continence Nurse Specialist role working within the Rapid Assessment service for older people with mental health problems had a dramatic impact on the continence of people with dementia.
Assessment of the problems: By applying the same approach to assessment as would be applied to any person presenting with bladder or bowel dysfunction, the role has been able to identify and treat physiological problems that are often overlooked in a person with a diagnosis of dementia. The application of diet and lifestyle techniques, and carer education as to how dementia affects a person’s ability to locate the toilet, can be effective in addressing a perceived incontinence.
Results of assessment: An audit of the service showed that in over 90% of people referred, continence was regained without the use of products.
Lessons and messages:
The value of a specialist continence approach to people with dementia
The underpinning principles of good continence assessment and management for older people with dementia
Practical continence promotion and management techniques for people with dementia
Educating other clinical practitioners in this innovative approach to continence and dementia.
59. IMPROVING PAEDIATRIC HOSPITAL CARE: FROM REDUCING INFECTIONS TO REDUCE LENGTHS OF STAY IN EMERGENCY DEPARTMENTS
B Spreadbury. Child Health Corporation of America
Forty-three leading paediatric hospitals in the United States reduced catheter-associated blood stream infections, narcotic-related adverse drug events, and emergency department length of stays, and improved surgical infection prevention practices.
Baseline hospital-specific rates were produced for each topic; a multidisciplinary expert panel was convened, and they developed the change packet and measurement strategy for the topic. On a monthly basis, the hospital teams reported data via a web-based tool, displaying their own performance and the reports from all participating hospitals. For example, the reduction in blood stream infections was achieved through the implementation of standardized insertion and maintenance bundles, and routine review of the need of the continued use of the lines.
The IHI’s model was used to implement the changes. Two to three learning sessions, coupled with action periods where the hospital teams implemented the changes, resulted in the improvements. Hospital teams, including physicians, nurses, other clinical staff, and quality improvement staff, made up the improvement teams. Results were shared in a variety of ways, including web-based monthly reports, conference calls, and storyboard reviews, all done transparently among the participating hospitals. The improvements were achieved in a 9–15 month period.
Improvements were achieved for all topics. For example, the 28 participating hospitals in the blood stream infection project prevented 112 children from suffering from an infection, with a savings of almost $1 million. The changes were monitored to ensure that they were maintained for an additional 12 month period, as well as spread to other units.
Lessons learned include: (1) improved safety for paediatrics can be achieved through changes that are customized for that population; (2) the breakthrough model provides an effective method for achieving improvement in a short period of time; (3) multidisciplinary teams, supported by leadership commitment, can achieve improvement in paediatric hospitals.
60. INDIVIDUALISED CARE SCALE FOR THE MEASUREMENT OF QUALITY ASPECTS OF CARE FROM PATIENTS’ POINT OF VIEW
R Suhonen, H Leino-Kilpi, A Berg, E Idvall, M Kalafati, J Katajisto, L Land, C Clemonidou, L Schmidt, M Välimäki. University of Turku, Department of Nursing Science, Turku, Finland
Background: Individualised care in health care services is receiving increasing attention in the development of health policy. Individualised care is one aspect of care quality. The Individualised Care Scale (ICS) has been designed to evaluate patients’ views of their individualised care in a hospital environment.
Assessment of problems: Outcomes of clinical care for similar patients often show large variations between countries, regions, hospitals and individual providers. There is need for international comparative analysis. The aim of this study was to adapt the original Finnish ICS for international use. The ICS was employed to study a sample of pre-discharge orthopaedic and trauma patients (n = 1126) in Finland, Greece, Sweden, UK and the USA.
Results of measurement: Between-country differences in patients’ perceptions of individualised care on a North-South European axis were found. The psychometric properties supported the validity and reliability of the adapted scales.
Strategies for quality improvement: These results may be applied to: (1) the evaluation of health care quality and its improvement; (2) the national and international development of nursing care; and (3) the involvement of patients in their care.
Lessons and messages: Trends in healthcare systems stress the increasing importance of involving patients in their care. Considering this preliminary evidence, the ICS shows promise as a tool for evaluating individualised care in Western cultures from patients’ perspective. The ICS has the sensitivity to discriminate between the responses of patients in different countries. It is important to establish equivalence of measures when translating and adapting a questionnaire.
Further research in different contexts is needed to further develop the instrument. Closer examination of the results in association with cultures, care protocols, practices, health care organisations and roles of personnel or patients in different Western countries may help to develop and harmonise clinical care in these countries.
61. BALANCING RULES AND DISCRETION: THE CASE OF AN EARLY WARNING SCORING SYSTEM
1A Suokas, 1M Dixon-Woods, 1E Pitchforth, 2RJ Lilford. 1Department of Health Sciences, University of Leicester, 2Department of Public Health and Epidemiology, University of Birmingham
Outline of context and problem: Early detection of patient deterioration can help to avert late admissions to intensive care units (ICUs) and reduce mortality, morbidity, and hospital costs. Many hospitals have introduced early warning systems (EWS) to standardise processes of observations and response. Discretionary behaviour is, however, likely to influence how these tools are put into practice. Based on an ethnographic study of patient safety and ward culture in four medical wards in four UK hospitals, we explored how the formal rules relating to EWS are enacted in practice.
Assessment of problem and analysis of its causes: We aimed to identify reasons for difficulties in identifying and responding to deteriorating patients, and what might inhibit the effectiveness of early warning systems. We explored the balance between standardisation and discretion, the positive and negative aspects of both, and wider issues that may influence implementation of EWS.
Effects of changes: Despite efforts to standardise the process of detecting deterioration, variation persists. We identified four areas of discretionary behaviour when using EWS in practice: setting frequency of observations for each patient; use of criteria for assessing patients; interpretation of vital signs and early warning scores; and decisions about involving other members of staff. Some observed variation was desirable and reflected appropriate use of discretion by staff. Some use of discretion was, however, less desirable and may reflect quality problems. Discretion will remain a key element of EWS because inflexible use may trigger unnecessary alerts or provide false reassurance. The challenge is how to encourage appropriate use of discretion.
Lessons and messages: Optimising detection of deteriorating patients is unlikely to be addressed successfully solely with formal rules. The performative aspect of EWS requires long-term “maintenance” in order to manage and support discretionary behaviour, which can be achieved through training, socialisation, monitoring and feedback.
Sponsoring institution: The Health Foundation.
62. PATIENT SAFETY AND MEDICATION WITH FOCUS ON CHILDREN
1C Svensson, 2A Kvarnefors, 1J Krook, 2B Andersson-Gäre. 1Apoteket AB (The National Corporation of Swedish Pharmacies), Qulturum, Jönköping, Sweden, 2Jönköping County Council, Qulturum, Jönköping, Sweden
Background: Overuse, underuse and misuse of medication is a general problem which is even more pronounced for children. Some serious events with unfortunate consequences have occurred lately in Sweden when handling and administering medication to children. Thus a structured improvement work is needed to improve the general patient safety for this patient group.
Objective: Improve knowledge about patient safety, i.e. in general as well as in paediatric care; implement improvements for increased safety in medication.
Method: An idea and dialogue seminar which took place in October 2006 preceded the start of the collaboration. During the collaborative from March to December 2007 the teams, consisting of at least one paediatrician, one paediatric nurse and one pharmacist, were offered tools in their improvement work; a risk analysis tool, the general methods for improvement work, e.g. the PDSA cycle, statistic tools, a safety culture enquiry and a web based work place called Reflex.
Results: Examples of team results:
The number of correctly ID-marked children has increased
The number of wrong prescriptions has decreased
A better environment in the room for preparing medication has been created
Standardised dilution schemes have been introduced in several units
A network between representatives for the Swedish Paediatric Society, the Swedish Association of Paediatric Nurses and the Scandinavian Paediatric Pharmacist Group has been established for further national collaboration regarding patient safety.
Conclusion: When teams from the same clinical speciality in health care come together for a collaborative it creates opportunities for good interaction and learning between one another. By involving the national interest associations for paediatricians, paediatric nurses and paediatric pharmacists the possibility for national spread of lessons learnt is facilitated.
63. WHY ARE DETERIORATING PATIENTS NOT RECOGNISED OR NOT ACTED UPON? A MULTI-METHOD APPROACH
K Beaumont, D Luettel, RG Thomson. National Patient Safety Agency (NPSA)
Many patients with cardiopulmonary arrests show prior deterioration; however, repeated studies reveal continuing failure to recognise or act upon deterioration.
An NPSA review of reported deaths showed that deterioration incidents included:
No observations for a prolonged period. (23%)
No recognition of the importance of the deterioration and/or no action taken. (49%)
Delay in the patient receiving medical attention. (28%)
Communication: problems occur during handovers and transfers of care, in relation to “outlying” patients and between medical and nursing staff. Nurses can struggle to convey information in a manner that would convince doctors of the urgency of the situation, making prioritisation difficult.
Tasks: nurses perceive observations as a low priority task and they are delegated to staff without sufficient knowledge or understanding. Respiratory rates are often not recorded.
Teamwork and responsibilities: high staff turnover and the way medical teams are organised inhibit effective team working; professional hierarchies and unclear roles and responsibilities are significant contributory factors.
A lack of strong and effective leadership further contributes to the problem. Nursing staff on acute wards are sometimes not led by a sufficiently experienced nurse, with responsibility for an overview of the wellbeing of all patients on the ward and available to junior staff for consultation, supervision and support.
Detecting and acting upon patient deterioration is a much more complex task than one might imagine, as shown by the triangulation of in depth studies. The findings have generated a series of reflective questions that hospital staff can use to identify priorities for change to address this serious patient safety problem.
64. IMPROVING PAEDIATRIC MEDICAL STAFF’S PRESCRIBING COMPETENCE
1D Tuthill, 2Z Taylor. 1Children’s Hospital for Wales, 2Department of Pharmacy, University Hospital of Wales
Doctors prescribing competence was assessed over a 7 year period. Developments to improve this were managed jointly by a paediatrician and a paediatric pharmacist in combination with other local protocols.
Background to problem: Paediatric medication errors complicate around 5% of all hospital admissions. Some are prescribing errors and are a significant problem. The recent introduction of the British National Formulary for Children (BNFc) has been designed to improve practice.
Assessment of problem and analysis of its causes: To try and reduce medication errors caused by doctors’ suboptimal prescribing practice, we set out to evaluate and improve the prescribing ability of paediatric doctors.
Methods: A standardised 30 minute lecture on paediatric prescribing was given in the Junior doctor induction programme from 2000 onwards. Participants then completed four prescribing questions in optimal conditions, using the BNFc or Medicines for Children and a calculator.
Strategy for change: Twice yearly training was provided. Two doctors scored 1 or less and were not permitted to prescribe until further individual education and reassessment.
Measurement of improvement: Assessment of Junior doctor scores at induction continued on a yearly basis. 44 doctors have participated.
Effects of changes and lessons learnt: Many doctors still make unforced prescribing errors. However, using the methods described, the situation has improved over the last 7 years. It is difficult to comment on how many medication errors had been prevented by this as prescribing errors are underreported.
Conclusion: Junior doctors’ competency to prescribe should be proven and not assumed. It is possible to improve prescribing ability to reduce the chance of medication errors happening.
65. IMPROVING MEDICATION PRESCRIBING IN INTENSIVE CARE: THE INTRODUCTION OF AN ELECTRONIC SYSTEM
1K Went, 2P Antoniewicz, 2DA Corner, 2S Dailly, 1P Gregor, 2J Joss, 2S McLeod, 1IW Ricketts, 2AJ Shearer. 1School of Computing, University of Dundee, Dundee, UK, 2Ninewells Teaching Hospital, NHS Tayside, Dundee, UK
Background: In close liaison with a clinical development team, a prototype of an electronic prescribing tool has been developed that is based on practices widely adopted by clinicians in the intensive care unit (ICU) which seeks to reduce prescribing errors.
Assessment of problem: An audit was conducted to identify deviations from local prescribing procedures and to form an understanding of the prescribing errors that occur in ICU.
Prior to introducing the system to ICU a pilot study was carried out to investigate whether the electronic system would reduce the errors identified in the audit. A patient scenario was created where participants were given 10 tasks. Participants were randomly split into two groups with one group performing tasks on the electronic system followed by the paper system and vice versa for the other group. The paper and electronic prescription charts created from the study were checked against 13 criteria derived from the local hospital policy.
Results of assessment: Compared with the established criteria the electronic system had an overall compliance of 84.23% compared with the paper system which had a compliance of 63%. The electronic system demonstrated an improved level of compliance against 11 of the 13 criteria. The two criteria where there was a drop in compliance highlighted a flaw with the interface and a requirement that was not fully identified. Feedback from participants suggested that the electronic system produced a positive user experience and was favoured by the clinicians, who considered it “very user friendly and intuitive”.
Lessons and messages: Applying usability techniques and engaging users throughout the design and development process have resulted in a system favoured by the users that demonstrates a reduction in prescribing errors. Adopting this iterative and responsive approach has also led to the users developing a strong sense of ownership of the system.
Funding: This research was funded in part through a Queens College Scholarship to the principal author
66. PUTTING EVIDENCE INTO PRACTICE: A MODEL SUPPORTING THE HEALTH CARE SECTOR WITH EVIDENCE-BASED KNOWLEDGE BY INTEGRATING METHODS FOR RESEARCH AND PROFOUND KNOWLEDGE OF IMPROVEMENT IN THE CURRICULUM OF HEALTH CARE EDUCATIONS ON ADVANCED LEVEL
1S. Johansson, 1,2H Wijk. 1Sahlgrenska University Hospital, Gothenburg, Sweden, 2Sahlgrenska Academy Institution of Health and Care Sciences Gothenburg University, Gothenburg, Sweden
Brief outline of context: The improvement work was done by health care students during a course on advanced level in Profound Knowledge of Improvement.
Brief outline of problem: There is a need for integration between practice based and evidence based knowledge among professional specialists in health care.
Assessment of problem and analysis of its causes: Profound knowledge of quality improvement in the health care curriculum has been missing.
Strategy for change: The management at the hospital was engaged in the project, as was supervising nurses around the hospital by presenting clinical problems for the students for them to improve during the process of the course, and to support the implementation of the result into clinical practice. Until now 65 students have been examined between March 2007 and 2008.
Measurement of improvement: Evaluation considering quality of hypothesis and methods, the value for caring, and students’ opinion on the importance of evidence- and experience-based knowledge for the development of caring.
Effects of changes: A specialist nurse-led out-clinic in oncology for better patient education, a tool for improved pain assessment at a dementia unit, a program for decreased post-operation nausea and vomiting among orthopaedic patients. Improved attitudes towards evidence-based knowledge in caring among hospital staff and need for knowledge of tools and methods of improvement among the specialist students.
Lessons learnt: The course is open for all professionals from the health care sector in order to support team-training within the frame of the course. The majority of the students have so far been specialist nurses, which calls for an extended promotion towards the broad sector of health care professionals.
Message for others: This model increases the possibility of integrating evidence-based content of the theoretical curriculum and methods for research and profound knowledge of improvement in close cooperation with the health care sector.
67. THE EMPLOYMENT OF STANDARD OPERATING PROCEDURES (SOPS) IMPROVES TRAUMA TEAM PERFORMANCE IN THE EARLY IN-HOSPITAL MANAGEMENT OF PATIENTS WITH MULTIPLE INJURIES
1T. Wurmb, 2P Frühwald, 1N Roewer, 1J Brederlau. 1Klinik und Poliklinik für Anästhesiologie der Universität Würzburg, Würzburg, 2Institut für Radiologie, Heinrich-Braun-Krankenhaus Zwickau, Zwickau, Germany
Background: Delayed and insufficient medical interventions in the trauma resuscitation room have a high impact on negative patient outcome.
Assessment of problems: Time wasting chaos is still one of the most important causes for inadequate care for patients with multiple injuries.
Results of assessment: Standardisation is well known to improve trauma team performance and to reduce fatal outcome.
Strategy for change: In our level I trauma centre a multiple trauma pathway describes the interdisciplinary organisation of multiple trauma care. In order to further optimize trauma team performance the decision to formulate standard operating procedures (SOPs) was made in 2005.
Measurements of improvement: Objective of the presented study was to determine whether the formulation of SOPs and the incorporation in our trauma pathway was associated with an improvement of trauma team performance, resulting in a more rapid initial assessment and resuscitation (Period A), in a more speedy diagnostic work up (Period B) and in a shortening of total stay in the emergency room (Period C).
Effects of changes: In a retrospective analysis 161 trauma patients were analyzed, with 82 patients in group I (non-SOP) and 79 patients in group II (SOP). Period A took 13 (10–17) minutes (median and IQR) in group I and 10 (8–15) minutes in group II, respectively (p<0.001). Period B was finished after 23 (17–33) minutes in group I and after 17 (13–21) minutes in group II (p<0.001). Period C was 47 (37–59) minutes in group I and 42 (34–53) minutes in group II, respectively (p<0.05).
Lessons learned: It was demonstrated that organisation and timing of life saving procedures lead to a more effective trauma treatment process and that organizational factors are an important determinant of trauma team performance.
Message for others: SOPs and a trauma clinical pathway are important tools which might contribute to continuous improvement of trauma care.
68. HEALTHCARE-ASSOCIATED INFECTIONS MUST STOP: A BREAKTHROUGH PROJECT AIMED AT REDUCING HEALTHCARE-ASSOCIATED INFECTIONS IN AN INTENSIVE CARE UNIT
D Yngström, K Lindström. Gällivare Hospital, Sweden
Gällivare Hospital in the north of Sweden is a multidisciplinary district hospital. In 2004–2005 the intensive care unit attended a breakthrough project with the aims of studying methods of increasing patient safety and systematically improving treatment outcomes.
Healthcare-associated infections are a problem within the Swedish health care system. The intensive care unit lacked a system for registering infections and we wanted to know their incidence, register and prevent them. We needed to increase compliance to basic hygiene procedures and to improve routines to prevent treatment related infections among ventilated patients.
Assessment of problems: 40% reduction in healthcare-associated infections in ventilator treated patients. 100% of staff to implement the basic hygiene rules.
Strategy for change: Base data were collected to provide a background for our work and the changes to be tested. Changes were implemented through instruction, verbal information and written routines. All personnel were involved in the change process and received continuous information, education and run-throughs of existing and new routines. Reporting and follow-up of measurements, evaluation and discussion took place at departmental meetings.
Measurement of improvement: Creation of treatment routines to prevent healthcare-associated infections. Registration of acquired infections in ventilator treated patients. Protocol for measuring staff compliance to basic hygiene routines.
Effects of changes: We achieved our goal and reduced the frequency of healthcare-associated infections in ventilated patients by 43%. Compliance to the basic hygiene routines has improved to 98%. Current measurements show that the improvement trend has continued.
Lessons and messages: During the project period we have made several changes, now established. To reduce the risk of acquiring healthcare-associated infections, a continuous systematic effort with continual measurements and review is necessary. We don’t know which particular changes were responsible for the achievement of our goal, but it has resulted in better routines.
69. REDUCTION OF MULTI-RESISTANT PSEUDOMONAS IN AN INTENSIVE CARE UNIT FOLLOWING IMPLEMENTATION OF A COMPUTERISED ANTIBIOTIC DECISION SUPPORT SYSTEM
MK Yong, KL Buising, KA Thursky. Royal Melbourne Hospital, Grattan Street, Parkville, VIC Australia 3050
Nosocomial gram negative organisms are of particular concern in ICUs throughout Europe and US with reported increasing rates of drug resistance—particularly with Pseudomonas.
This study evaluates the long term impact of an antimicrobial decision support system on drug resistance among common gram negative organisms. The study was undertaken within the Royal Melbourne Hospital ICU over the period of January 2000 to December 2006. High rates of broad spectrum antibiotic use in the ICU led to the development of a computerised antibiotic decision support system (ADVISE) that was implemented in 2002. A pre- and post-evaluation study demonstrated a 39% reduction in carbapenem use, a 42% reduction in third generation cephalosporins and a 33% reduction in vancomycin use. We analysed the numbers and percentage of drug resistant organisms from 2 years prior to implementation up to 2006 in order to observe whether significant changes in antimicrobial use impact on subsequent isolation of drug resistant organisms.
There was a marked reduction in carbapenem resistance of all ICU isolated Pseudomonas organisms in the years following the ADVISE program from 45% resistant in 2002 to 19% resistant in 2006 (see fig). Similarly the percentage of gentamicin resistant Pseudomonas organisms reduced from a peak of 24% in 2003 to only 3% in 2006. All other gram negative organisms demonstrated a stabilisation of drug resistant patterns in the study period since carbapenem resistance was not noted to be a major problem to begin with (near 100% sensitivity). A trend towards a reduction in resistance toward piperacillin-tazobactam was also observed with Klebsiella spp, Enterobacter spp and Escherichia coli.

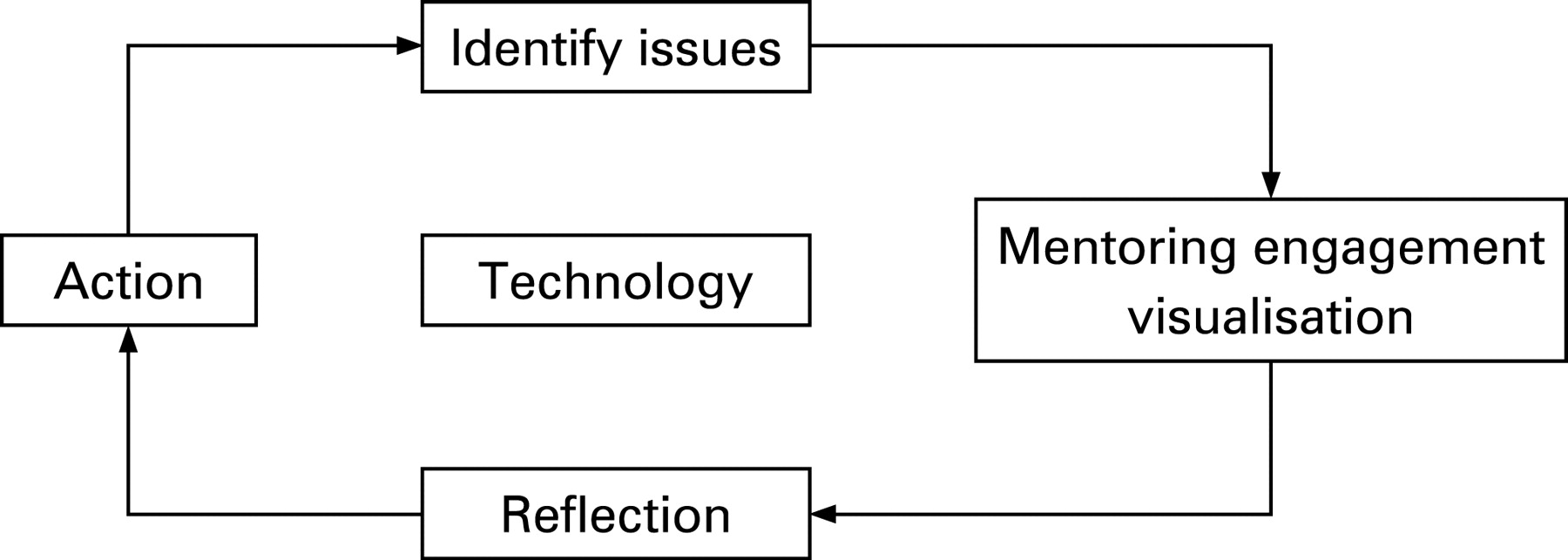{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
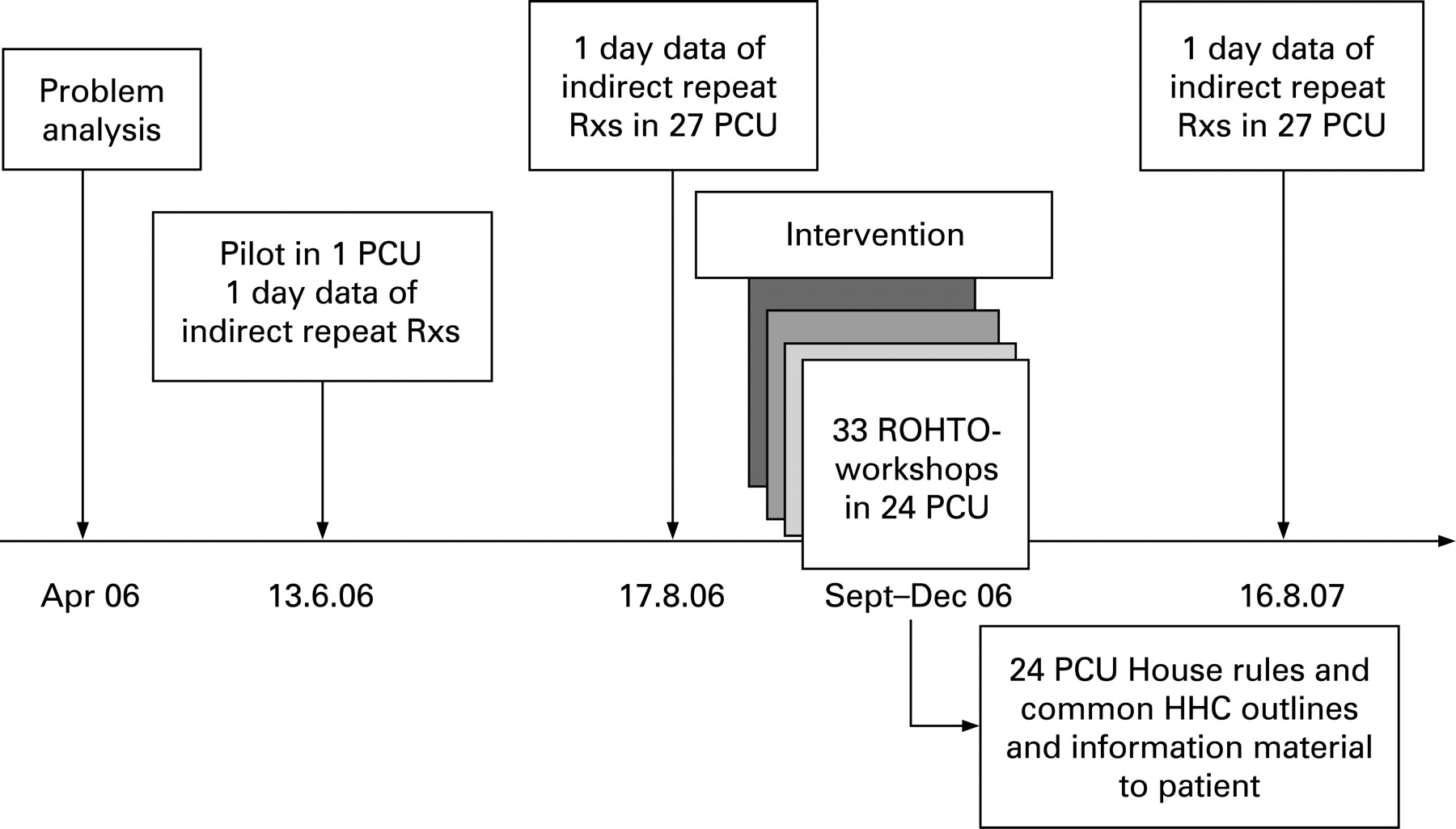{kind=link}
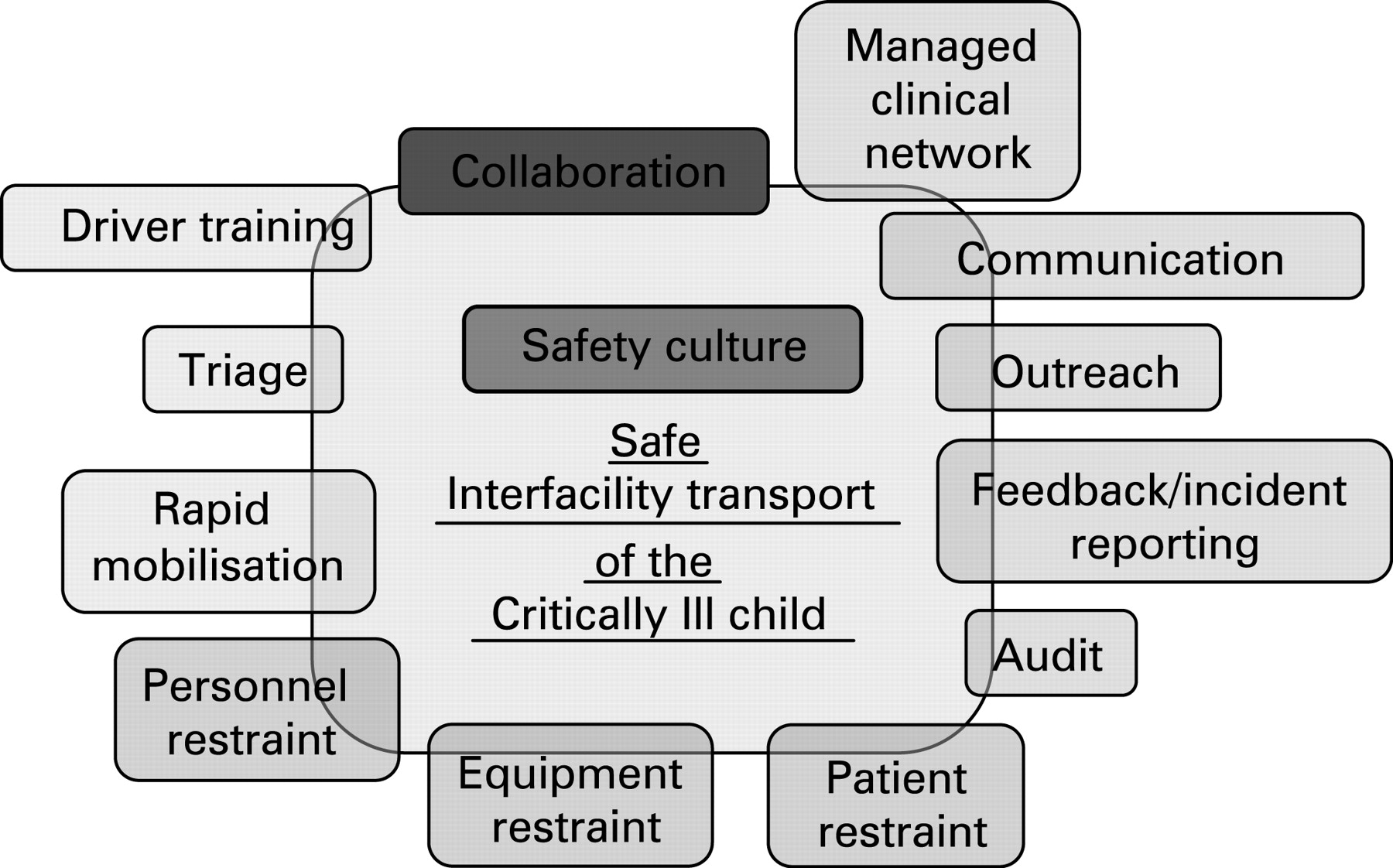{kind=link}
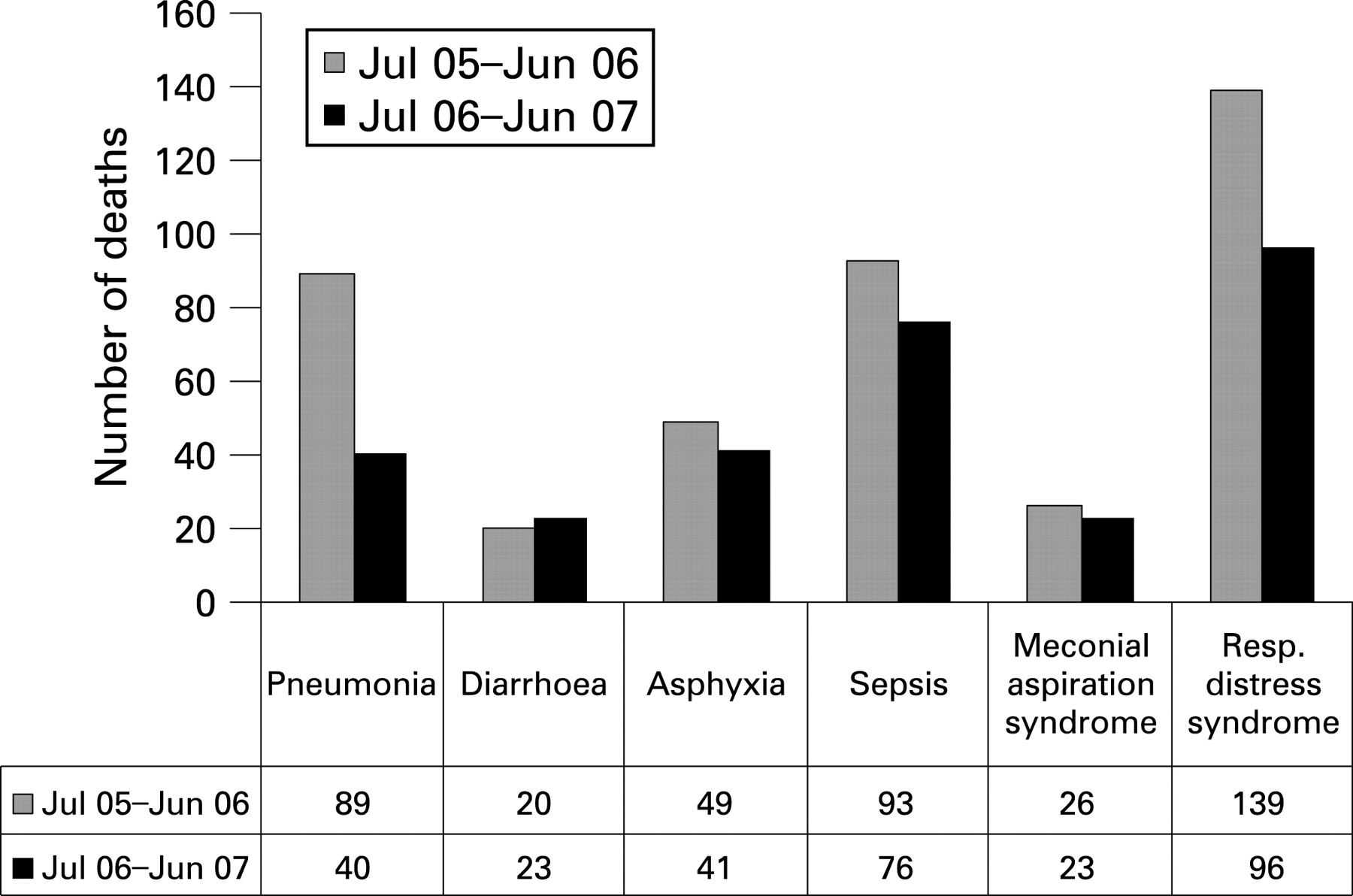{kind=link}
{kind=link}
The emergence of multi-resistant gram negative organisms within an ICU can be stabilised and even reduced, as in the case of multi-resistant Pseudomonas, by interventions aimed at reducing the use of broad spectrum antibiotics.
70. SAFE INCIDENT REPORTING IN A DUTCH GENERAL PRACTITIONERS OUT-OF-HOURS SERVICE
DLM Zwart. Patient Safety Centre, UMC Utrecht, The Netherlands
Background and problem: Primair GP services is an out-of-hours organisation in The Netherlands which covers 1.6 million inhabitants with 8 GP services. Primair implemented a central incident reporting procedure (CIRP) in 2005, to which all healthcare workers (880 GPs and 200 GP assistants) from these 8 out-of- hours-services could report their incidents. CIRP received only a small number of incident reports, representing only a small proportion of the actual incidents.
Strategy and effect of change: To improve number and outcome of incident reporting a pilot was started using an alternative method, Safe Incident Reporting (SIR). SIR is based on reporting safely and easily in a clinical setting, using root cause analysis and a short feedback loop. It was tested during 9 months in 2007 in one out-of-hours service covering 137 000 inhabitants. This resulted in 90 incidents reports, compared with 6 incident reports to the central committee in the year before. 36% of the incidents were reported by GPs, 59% by GP assistants, 5% by GP residents or drivers. 3% of the reports concerned medical errors, 48% process errors, 36% communication and team work errors, and 11% related to material, technology or logistics. Incidents with high risk scores (n = 16) were analysed. 55 root causes were found: 20 organisational, 23 human, 3 technical, and 8 causes could not be categorised.
Lessons learnt: SIR is a useful method in a primary care out-of-hours setting. It increases the number of incident reports and enhances analysis compared to CIRP. Because analysis is done close to the working environment by care givers who actually work in the GP service, it’s done faster and more detailed. The number of reports concerning medical decisions is low. Possibly this was due to a feeling that it was unsafe to report these sensitive incidents, or because they are considered as “part of the job” and not a possible learning moment.
Sponsoring institution: SBOH (Dutch financing organisation of GP vocational training).