Article Text

Abstract
Background Simulation-based medical education enables knowledge, skills and attitudes to be acquired for all healthcare professionals in a safe, educationally orientated and efficient manner. Procedure-based skills, communication, leadership and team working can be learnt, be measured and have the potential to be used as a mode of certification to become an independent practitioner.
Results Simulation-based training initially began with life-like manikins and now encompasses an entire range of systems, from synthetic models through to high fidelity simulation suites. These models can also be used for training in new technologies, for the application of existing technologies to new environments and in prototype testing. The level of simulation must be appropriate to the learners' needs and can range from focused tuition to mass trauma scenarios. The development of simulation centres is a global phenomenon which should be encouraged, although the facilities should be used within appropriate curricula that are methodologically sound and cost-effective.
Discussion A review of current techniques reveals that simulation can successfully promote the competencies of medical expert, communicator and collaborator. Further work is required to develop the exact role of simulation as a training mechanism for scholarly skills, professionalism, management and health advocacy.
- Simulation-based training
- medical education
- new technologies
- healthcare training
- patient safety
- team training
- training
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
- Simulation-based training
- medical education
- new technologies
- healthcare training
- patient safety
- team training
- training
Introduction
Primum non nocere ‘above all, do no harm’ is considered a fundamental of medical practice.1 Yet, the Institute of Medicine's landmark report of 2000, To Err is Human, revealed that up to 98 000 hospital deaths occur in the USA as a result of medical error each year.2 A number of global studies suggest that approximately 10% of patients admitted to hospital suffer from some kind of harm.3–7 Medicine has traditionally relied on a ‘see one, do one’ approach to learning and experience.8 This inevitably exposes patients to inexperienced healthcare practitioners, and the dangers and harm associated with this are increasingly unacceptable. The term ‘learning curve’ has repeatedly been used to account for higher complication and mortalities, as well as longer procedure times, among inexperienced practitioners and teams.9 Climbing the steep learning curve can no longer be done by trial and error, so it is necessary to explore, define and implement models of health professional training that do not expose the patient to preventable errors. One such model is simulation-based training.10
Simulation ‘is a technique to replace or amplify real-patient experiences with guided experiences, artificially contrived, that evokes or replicates substantial aspects of the real world in a fully interactive manner.’11 As an educational strategy, simulation provides the opportunity for learning that is both immersive and experiential. Thus, to improve education and ultimately enhance patient safety, healthcare professionals are using simulation in many forms including simulated and virtual patients, static and interactive manikin simulators, task trainers, screen-based (computer) simulations and ‘serious’ gaming. Moreover, simulation has the potential to recreate scenarios that are rarely experienced and test professionals in challenging situations, and to carefully replay or examine their actions.12 It is a powerful learning tool to help the modern healthcare professional achieve higher levels of competence and safer care.
Beyond the impact on individual and team performance, simulation techniques provide an opportunity to improve system performance. In addition to practitioner inexperience, the Institute of Medicine emphasised that most medical errors are systems-related and not attributable to individual negligence or misconduct.2 The key to reducing medical errors is to focus on improving the systems of delivering care and not to blame individuals. Research has shown that system improvements can reduce error rates and improve the quality of healthcare.13
There are three broad domains in which simulation is used by healthcare professionals. First, simulation techniques can be used for practice and assessment of technical procedures.14 This can take a variety of forms ranging from simple bench models to sophisticated virtual reality machines. Second, simulated or standardised patients have long been used to teach clinical skills and are the foundation for performance-based assessment.15 Third, simulation technologies have been used for team training, improving function in tension-filled complex situations.16
The aim of this review is to study the application of simulation-based technologies for the enhancement of healthcare with respect to improvements in patient safety. The article is structured to provide a background to simulation-based learning and practice within healthcare environments, and then discusses their relative effects on patient safety within an appropriate training framework. To enhance quality of care, training must occur within, and apply to, a greater system; this is also examined. Finally, a report card is defined on the basis of current simulation techniques and their application within different domains in healthcare.
History of simulation as applied to health-professional education
Simulation-based medical training programmes are often traced back to the late 1960s and early 1970s, when researchers from the University of Miami developed Harvey, the Cardiology Patient Simulator, a hybrid between a sophisticated task trainer and computer-enhanced manikin simulator.17 This simulator was able to integrate all of the bedside findings and realistically reproduce both common and rare cardiac diseases. A multicentre study of a cardiology patient simulator sponsored by the National Heart, Lung and Blood Institute (NHLBI) in the USA compared the level of bedside technical skills and cognitive knowledge of students taught using simulation versus students taught in a conventional patient-dependent programme; the study involved a total of 208 students (116 simulator-trained and 92 non-Harvey-trained) at five medical schools.18 A unique and critical feature of the study was the testing of bedside skills using actual patients with real findings. Fourth-year students who used simulation during their cardiology elective acquired more cognitive information and were better skilled in bedside cardiac examinations than their counterparts who were trained in the traditional manner. Importantly, this included better bedside skills on real patients with cardiac findings.
In the 1980s, Gaba developed and implemented the use of computerised manikins for anaesthesiology trainees.19 These techniques provided opportunities for repeated practice in a safe and pedagogically sound environment. There was a key focus on the concept of debriefing and on the importance of the operating team. Today, it is possible to purchase ‘off the shelf’ manikins that breathe, can dilate their pupils or experience an arrhythmia. Modern manikins are much more practical than their ancestral prototypes and can deliver sophisticated simulations using wireless technologies. Synthetic latex-based simulation models for procedural tasks, and more recently the use of virtual reality simulation, have added to the simulation armamentarium and have created a new science that has a rapidly expanding network of scholars in this area (figure 1).

Medical simulation time line: a notional timeline of patient-based, technical skills and whole-procedure simulation over the past four decades.
Despite the intuitive appeal of simulation as a learning tool, especially for procedural competence, there have been small gains to date. The first ‘Virtual Reality to Operating Room’ study to prove the benefit of simulation-based training on real patients was published over 7 years ago.20 Nonetheless, a systematic review published in 2004 was not able to show conclusively an added benefit from sophisticated surgical simulation.21 As such, it is currently widely accepted that simulators serve as an adjunctive tool, not a replacement, for patient-based operative experience. Despite a modest initial report card, simulation training and its associated science is expanding rapidly and must be currently viewed as being in its infancy. Simulation will undoubtedly play an increasingly prominent role as technologies improve and as educators attempt to cope with the stresses of training: including a reduced working week, increasing intolerance of error and the ever-increasing cost of the ‘procedural minute.’ In addition, when there is limited access to qualified faculty in clinical settings or limited exposure to actual patients who are experiencing low-frequency and high-risk situations, students might not receive the experience necessary to become confident and competent in early recognition and rescue. Simulation provides the opportunity for all learners to have a consistent experience with these potentially life-threatening conditions.
Patient-based simulations were first developed with the advent of the programmed patient; usually a lay individual who was taught to simulate a medical condition.22 This construct was quickly adopted by Harden and others with the development of the Objective Structured Clinical Examination (OSCE).15 In the OSCE, students rotate through a series of stations where they encounter actors functioning as simulated patients. The students take a history, conduct a physical examination, order and interpret investigations, initiate management plans and communicate with the patient. Over 30 years of experience with the OSCE has shown it to be a valid and reliable method of assessment across a wide spectrum of learners.23 This technology brought two major advances to the testing field for clinical competence. First, examinees saw the same ‘patients,’ resulting in a standardised and fair approach to testing. Second, examinees had to demonstrate what they would do in a given situation, not what they might do as inferred from less realistic assessment techniques such as essays and multiple choice examinations.
The OSCE has given birth to similar forms of assessment such as the Objective Structured Assessment of Technical Skills (OSATS), which was developed in Toronto and is now being used as a measure of assessing technical competence in a bench-model ex vivo situation, away from patients.24 This examination has candidates performing elements of a technical procedure while being scored by experts using structured checklists and global rating forms.
The use of simulation-based education or health professionals is not limited to the medical profession. Nursing and other health professions have embraced the same notion as both technology and pedagogy. In the USA, for example, Jeffries et al outlined the core elements necessary to integrate simulation into nursing curricula.25 Early studies have reported increased learner confidence and demonstrated skills in end-of-programme evaluation. Transition of this confidence and skill into practice are still being measured.
Principles of simulation-based training
The principal use for simulation in the domain of technical competence is to provide learners with an opportunity for deliberate practice.26 As such, they can make mistakes in a safe environment, learn from those mistakes and achieve proficiency by attaining predefined benchmarks. This applies to any procedural skill; for example, insertion of a central venous catheter, forceps delivery of a baby, construction of a small-bowel anastomosis or intubating the airway of a patient. Simple and inexpensive low-fidelity synthetic models exist, providing the operator with the opportunity to use real instruments to refine their skills.27 Another option is to use cadaveric or animal-derived tissue to practise such tasks.28 The recent advent of high-fidelity virtual reality simulation has further increased the role of simulation in training interventionalists, in image-guided procedures, for laparoscopy, endoscopy and endovascular surgery.29
Bringing members of the healthcare team together in a simulated environment enables ‘team training’ to explore communication, decision-making, judgement and leadership skills.30 Although potentially resource heavy, this has been shown to be a feasible and instructive technique for teams such as those involved in the operating room, delivery suites and intensive care units.31 Indeed, a few centres have now begun to use ‘in situ simulation,’ which brings the real team to the real environment but with a computerised manikin as the patient. Hunt et al report improved individual and team response in acute and ambulatory care settings following in situ simulation.32 Crisis scenarios can be played out with extensive debriefing performed on an individual and team basis.
Although the airline industry is the commonly cited frame of reference for medical simulation, it is important to think of other high-reliability industries such as oil, military and nuclear that are safety aware and simulation-savvy. Training in the armed forces includes regular simulation exercises for potential future conflicts, in order to achieve the desired aim with casualties kept to a minimum. Only when recruits have passed the numerous simulation exercises will they be allowed to participate in real conflict. There are increasing efforts to translate lessons learnt in these environments to the healthcare industry. Efforts include the creation of screen-based virtual hospitals and health systems, as well as ‘serious’ gaming initiatives.33
Medical training
The traditional master-apprenticeship model, described by Halsted, has stood the test of time well;8 however, it faced a severe challenge in the 1990s with the rapid spread and dissemination of new technologies such as laparoscopic surgery.34 Put simply, there were not enough ‘master’ surgeons to teach the apprentices. Although many surgeons carried out practice simulation on animal models, the majority did not subject themselves to an adequate number of training sessions leading to unnecessary morbidity and mortality when they operated on their patients.9 The introduction of new technologies to surgery, such as robotics, endoluminal surgery and energy-based intervention, has the potential to repeat this mistake. A similar problem can exist when an established technology is introduced to a new setting, particularly in developing countries. There is a clear need for training to be part of the set-up package. Stringent regulation for the introduction of new technologies should be required, with audit of initial performance and comparison with conventional standard approaches. Early adopters, although enthusiastic, should not be provided with a free rein to repeat the ‘biggest unaudited free-for-all in surgery,’ a sobering commentary on the adoption of laparoscopic cholecystectomy.34
A key aspect of any type of training is the level of fidelity or realism that is required.35 The difference in price between a porcine, a synthetic or a virtual reality model of doing a cholecystectomy ranges from 10- to 10 000-fold. Is the higher-fidelity model really so much better? Grober and colleagues performed a study to compare clinically relevant outcomes for spermatic cord micro-anastomosis between synthetic and in vivo models.36 After only a second attempt at the outcome measure of a real-world microvascular anastomosis, there were no differences in outcome whether one trained on a low-fidelity or high-fidelity simulation. However, the mechanism by which fidelity affects learning is not clearly understood. Although certain high-fidelity features can be costly, lower-fidelity models have been shown to improve surgical skill acquisition. There is consensus that the level of fidelity should match the level of the learner and the educational goal. For example, expert-level learners might benefit more from learning environments that employ higher levels of fidelity. Figure 2 illustrates how the optimal level of fidelity might vary for novice, experienced and expert learners. This relationship needs to be substantiated by further evidence.37

Relationship between level of experience and simulator fidelity. A novice practitioner will gain most from a low-fidelity simulator that has the ability to teach generic skills. An experienced practitioner will require task refinement, which is more likely to be gained from a higher-fidelity simulator that can simulate complex tissue interactions or crisis scenarios such as bleeding.
Simulation is merely a tool for training, and the success of simulation as an exercise is dependent not so much on the level of fidelity, but on how simulation is used by the trainee and the trainer. It is important to view simulation as part of a system aimed at improving performance. For example, in 2007, an Intercollegiate Surgical Curriculum Project (ISCP) was launched in the UK aimed at the systematic use of simulation within a curricular framework to enable ‘high-quality care for the surgical patient,’ through systematic and competency-based progression, underpinned by robust assessment processes.38
Scope of simulation in healthcare using the CanMEDs framework
To consider the scope of simulation in healthcare, it was first necessary to set limits to the broad area of research available. This was performed through discussion and expert consensus, through the narrative that follows.
Simulation-based medical education can be useful in a broad range of areas and skill sets, with potential impact upon patient safety. To identify key skill sets, recognised frameworks that describe the roles or skills of a good healthcare practitioner were reviewed. Three frameworks were considered: Good Medical Practice,39 published by the General Medical Council in the UK, The CanMEDs Framework of the Royal College of Physicians and Surgeons of Canada40 and six competencies of the Accreditation Council for Graduate Medical Education (ACGME) in the USA.41
Good Medical Practice sets out the principles and values on which good practice is founded.39 These are the basic duties of a doctor, illustrated in box 1. With regards to the six competencies from the ACGME, these are presented in box 2 with brief descriptions.41
Box 1 Principles and values on which good medical practice is founded
Make the care of your patient your first concern
Protect and promote the health of patients and the public
Provide a good standard of practice and care
Treat patients as individuals, and respect their dignity
Work in partnership with patients
Be honest and open, and act with integrity
Box 2 Six competencies from the Accreditation Council for Graduate Medical Education
Patient care—to provide patient care that is compassionate, appropriate and effective
Medical knowledge—to demonstrate and apply medical knowledge
Practice-based learning and improvement—to demonstrate the ability to investigate and evaluate their care of patients, to appraise and assimilate scientific evidence, and to continuously improve patient care
Interpersonal and communication skills—that result in the effective exchange of information and collaboration with patients, their families and health professionals
Professionalism—to carry out professional responsibilities and adhere to ethical principles
Systems-based practice—demonstrate an awareness of, and responsiveness to, the larger context and system of healthcare.
The CanMEDs framework, developed in the 1990s, describes the abilities needed for physicians to provide high-quality care. The standards are used to describe the educational needs of practising physicians, as well as framing the training needs and the basis for evaluation of trainee physicians. The seven key competencies are the specialist physician as medical expert, communicator, collaborator, scholar, professional, manager and health advocate (figure 3). For the overview, the CanMEDs framework was chosen as a viable and tested classification of competency that traverses medical specialities, because it is comprehensive and has been the forerunner of later frameworks.

CanMEDs 2005 Framework.40 The CanMEDs framework describes seven key competencies required for physicians to provide high-quality care.
Following confirmation of the classification system to be used, a review of the literature was undertaken. This was guided by expert consensus through four teleconference calls between November 2008 and April 2009. The process led to the identification of key documents that demonstrate the use of simulation in each area, particularly with respect to a focus on patient safety. For each CanMEDs competency, a definition is provided, the importance of the competency with respect to patient safety is described, and one or more exemplar case studies that illustrate how simulation can be used to improve patient safety are outlined. A summary of the present use and potential for simulation in that area is also provided. A final face-to-face meeting of the working group was held in May 2009. The outputs were further critiqued by members of the other three working groups within this supplement. What follows is a narrative that seeks to distill the key findings of this process.
Medical expert
As experts, healthcare practitioners integrate all the CanMEDs roles, applying medical knowledge, clinical skills and professional attitudes in their provision of patient-centred care. This competency focuses on the cognitive component of medical knowledge, the technical competence in performing procedural skills and the application of judgement and experience to diagnostic and therapeutic decisions.
Simulation, and the use of simulators to educate healthcare practitioners, has been shown to be effective in transferring knowledge to both trainees and practising healthcare professionals. A wide variety of technologies including virtual reality, simulated patients, animal models, and static and interactive manikins have been shown to be effective teaching tools. Several studies have documented transfer of training to patient care settings. Barsuk and colleagues studied internal medicine residents and showed that trainees who have mastered central venous catheter insertion in a simulation laboratory have significantly fewer procedural complications (eg, needle passes) in an intensive care unit than residents who are not simulation-trained.42 In obstetrics, Draycott and colleagues have published extensive research demonstrating improved neonatal outcomes of births complicated by shoulder dystocia after the implementation of simulation-based training.43 Within the surgical domain, there exist a handful of studies which have proven that simulator-trained individuals are faster and more accurate, and commit fewer errors during their first real case.20 29 Two recent studies have measured this effect for the early part of the learning curve in the clinical environment: the curve was found to be both shorter and flatter than for groups trained in the standard manner.44 45
Another important aspect of simulation-based training is its durability in the real environment. Wayne and colleagues demonstrated that Advanced Cardiac Life Support (ACLS) skills acquired by internal medicine residents in a simulation laboratory do not decay at 6 and 14 months post-training.46 Likewise, Crofts et al in obstetrics showed that acquired skill at managing shoulder dystocia was largely maintained at 6 and 12 months postsimulation training among midwives and doctors in the UK.47 Simulation-based training for procedural skills is firmly established, but its widespread use remains a challenge. By removing the learning curve from patient to simulator, patient care will be made safer. The role of the medical expert is clearly wider than procedural-based skill, but the process of using simulated patients or simulators on which learning can take place and its effectiveness evaluated has tremendous proven value.42 Nonetheless, there are some aspects of high-level clinical judgement and decision-making that might be elusive even to simulated clinical environments; these might simply have to be mastered during clinical encounters. This probably refers to rare clinical episodes or mass casualty in rudimentary environments such as war zones.
Communicator
All healthcare providers have to communicate effectively to patients, relatives, colleagues and, at times, the wider public or media. Communication may be written or verbal. The Joint Commission on Accreditation of Health Care Organisations reported that two-thirds of the nearly 3000 sentinel events (serious medical errors) reported between 1995 and 2004 were attributed to poor communication.48 Poor communication between team members in the intensive care unit and in the operating room have been shown to be a common causal factor underlying adverse events in these locations.49 50 Patient handovers and transitions in care are particularly vulnerable to information loss regardless of setting.51 Excellent communication skills are vital for challenging situations, such as breaking bad news and medical error disclosure.52 ‘Being open’ policies are increasingly encouraged, and sought by patients, yet a lack of skills on behalf of the physician remains an important barrier.
A team at Imperial College (UK) has looked at training and assessing communication skills alongside the performance of procedural skills using standardised scenarios: a technique referred to as an Integrated Procedure Performance Instrument (IPPI).53 Examples of IPPIs that couple technical simulation with a real patient include wound closure, urinary catheterisation, removal of skin lesions, gastrointestinal endoscopy, laparoscopic cholecystectomy and carotid endarterectomy. In a similar vein, standardised patients have been used in situations where a trainee might be required to prescribe medicine to angry and aggressive (simulated) patients. With the additional realism of making decisions in a stressful ‘real-world’ environment, research has shown that trainees are more liable to make mistakes, such as administering penicillin without checking the patient's allergy status. Consistent with CanMEDs' definition of an effective communicator, the IPPI includes specific communication tasks prior to the procedure (history-taking, patient consent), during the procedure (team communication with nurses, anaesthetist, assistants and patients, if conscious) and after the procedure (disclosure of medical error, procedure note and patient orders). The IPPI has shown to be an effective tool for teaching and evaluating communication skills in residents and medical students.54
Collaborator
There is a growing appreciation of the need for healthcare personnel to work in a collaborative team in order to affect optimal patient care.55 The Institute of Medicine recommends interprofessional healthcare education as a patient safety strategy. The days when the model of healthcare delivery focused on the physician only, with other healthcare providers performing a subordinate role, are numbered. The skills to work collaboratively with others, both within and across healthcare teams and environments, will be crucial for the optimal delivery of patient-centred care. Improving teamwork to improve safety has been widely applied in a variety of high-risk industries, most notably with the use of Crew Resource Management (CRM) in the airline industry. Similar CRM initiatives have been used to improve patient safety.
Researchers in Denmark have developed a framework for team-training courses: from needs assessment to delivery and evaluation.56 Simulation is a key part of an integrated education package. One report shows that simulation-trained internal medicine residents respond as teams to real hospital ‘codes’ (cardiac arrest events) with much greater compliance to treatment protocols than more educationally advanced resident teams that were not simulator-trained.57 Similar principles have been applied to other areas, such as trauma team training and neonatal resuscitation. A recent collaboration between the Agency for Healthcare Research and Quality and the US Department of Defence resulted in the development of the TeamSTEPPS simulation-based curriculum to improve patient safety through enhanced communication and other teamwork skills.58 One of the core competency areas of TeamSTEPPS is team leadership, including the ability to direct and coordinate activities of team members, assess team performance, assign tasks, develop team knowledge and skills, motivate team members, plan and organise, and establish a positive team atmosphere.
Simulation is widely used both within and outside medicine to deliver team training. The interactive and practical nature of teamwork make simulation the preferred method to deliver team training; however, it remains underused in hospitals and other healthcare settings. Salas and colleagues perceived a need to identify and describe key principles of team training in healthcare that can be embodied in curricula and taught using simulation technology.59 They performed a quantitative and qualitative review of available literature including a ‘content analysis of team training in healthcare.’ The result is a set of ‘eight evidence-based principles for effective planning, implementation and evaluation of team training programs specific to healthcare.’ The eight critical principles are shown in box 3.
Box 3 Eight critical principles of team training
Identify critical teamwork competencies—use these as a focus for training content
Emphasise teamwork over task work—design for teamwork to improve team processes
One size does not fit all—let the team-based learning outcomes, desired outcomes and organisational resources, guide the process
Task exposure is not enough—provide guided, hands-on practice
The power of simulation—ensure training relevance to transfer environment
Feedback matters—it must be descriptive, timely and relevant
Go beyond reaction data—evaluate clinical outcomes, learning and behaviours on the job
Reinforce desired teamwork behaviours—sustain through coaching and performance evaluation
Scholar
As scholars, healthcare professionals demonstrate lifelong commitment to reflective learning and applying new knowledge, as well as teaching others. To improve patient safety, healthcare practitioners need to reflect on their practice and to actively seek out, or learn, new ways to make their practice safer. Sportsman et al describe how both nursing students and hospital staff can use a regional simulation centre.60
The broad array of existing and developing simulation activities and technologies provide the opportunity for individuals and groups to efficiently and effectively deliver new content or reinforce existing knowledge, as well as to practise the application of new knowledge safely until mastery is achieved. Moreover, simulation teaches reflective practice. A key element of simulation is debriefing and the opportunity to reflect on one's actions and their impact.61
The relationship for simulation with this competency is different to the others. Simulation is a technique for teaching and learning. As scholars, all healthcare practitioners should embrace simulation as a tool to aid teaching and learning across a wide range of cognitive, behavioural and psychomotor competencies. As with the other competencies, simulation can be used as a tool to teach the roles and skills associated with being a scholar such as critical appraisal, teaching a group of students or assessing learners.
Professional
A professional is committed to the health and well-being of individuals and society through ethical practice, profession-led regulation and high personal standards of behaviour. Although teaching and evaluating professionalism remains a priority, with an obvious relation to patient safety, unprofessional or unethical behaviour continues to be reported. Professionalism tends to be seen as a skill somehow different from those cognitive, behavioural and psychomotor skills traditionally taught to health professionals. However, there is agreement that professionalism can be taught, although it may often be taught through the ‘hidden curriculum’ by observing, experiencing and discussing real-life events.
Ginsburg et al asked medical students to view five videotaped scenarios that required action in response to a professional dilemma; for example, role resistance.62 The aim, through the use of simulated real-time encounters, was to develop an understanding of reasoning processes that students undergo in response to a professional dilemma. Students were motivated to consider certain actions by referring to honesty, disclosure and fairness to patient care, but also mentioned other principles such as deference or obedience to a senior doctor or allegiance to one's team. In an examination setting, students know to always focus on patient care and comfort. Within these realistic simulations, it was possible to elicit behaviours that might be more likely to occur in the clinical setting. In a further study, Ginsburg compared students' reasoning to professional dilemmas with either interview, text-based or videotaped scenarios.63 There were no differences in opinion between the latter two, although when compared with interview scenarios, students' exam responses showed a shift towards acceptable actions, despite still considering implications for themselves.
Recently, Hochberg et al developed a curriculum for teaching professionalism to surgeons, consisting of six 1 h interactive sessions (eg, admitting mistakes, interdisciplinary respect) delivered through a variety of teaching methods (eg, video re-enactments of ‘the good, the bad and the ugly,’ faculty role modelling). The assessment methods employed a six-station OSCE using trained standardised patients in scenarios such as ‘patient transfer—receiving a phone request from the emergency room to accept a patient with a venous stasis ulcer (ie, a ‘dump’)’ or ‘taking a sign-out—identifying a resident colleague as an impaired physician.’ The authors state that the curriculum is feasible and acceptable, and improves patient satisfaction with their doctors.
A further difficulty is the method of rating professionalism. Mazor et al analysed the ratings of standardised patients, doctors and lay people to 20 videotaped encounters between medical students and standardised patients.64 Raters varied in which behaviours they attended to, and how they evaluated them, being true for between and within rater type. This study describes the challenge of rating professionalism in doctor–patient encounters and draws attention to the need for multiple assessments by multiple raters at different time points.
Manager
As managers, healthcare practitioners are integral participants in healthcare organisations, organising sustainable practices, making decisions about allocating resources and contributing to the effectiveness of the healthcare system. A key challenge in patient safety is developing safe healthcare systems, in which healthcare practitioners should take a lead role. Although nurses have often stepped up to this leadership challenge, there is a concern that clinical leadership among doctors is underdeveloped and underutilised. Leadership and supervision of colleagues are important for promoting a safety culture.65 66
There is some evidence on the effect of simulated patient-based programmes on health professionals' communication and teamwork skills, which have a clear overlap with some aspects of their management skills.16 However, the explicit use of simulation-based training to improve management skills of leaders in the health profession or to train professionals for management skills is not described in the literature. Simulation-based training could be used for health professional leaders deploying extremely challenging managerial scenarios; for example, giving an apology to a patient for a serious mistake that occurred, managing a violent crisis or managing a crisis with staff members who are behaving unethically. Similarly, scenarios have been developed for training risk-management teams; for example, encountering multiple difficult tasks as they manage crisis with health professionals, patients and families, malpractice insurance lawyers, media and ministry of health officials.67
Health advocate
A health advocate is someone who speaks out for a cause. Advocacy gives voice to several questions: What is wrong here? Could we do better? How can I work with the system in order to benefit my patient? Consequently, advocates often witness and bring to light inequities, unfair practices and potentially dangerous health conditions and practices. Advocates can operate on a local scale championing patient safety in their department or hospital, or might act on a national or global scale. Advocates could be healthcare practitioners, patients and their relatives or people with a special interest.
In the USA, the Johns Hopkins' Bloomberg School of Public Health (JHSPH) runs an advocacy training programme for their graduate students. The course has a three-pronged ‘advocacy construct’ that integrates didactic lectures, presentations by real-world experts and skills practicum using case studies.68 The skills practicum involves a 90 min simulated group exercise, targeting media advocacy and communication. Students are given a health-related topic about which to develop a policy position, messages that frame the policy position and advocacy strategies to advance the proposed policy improvement. When the group has completed its preparation, a simulation exercise occurs with a ‘mock’ television reporter and video film crew. The reporter interviews each student, asking challenging, real-life questions to help the students learn to communicate effectively while advancing a health-policy position.
Advocacy, although clearly important, is perhaps not always seen as a skill that can be trained. Simulation is presently underused to teach advocacy but has potential within the field of patient safety.
A systems-level approach to changing the culture of healthcare
The airline industry has often been cited as the example for healthcare to follow in learning to improve safety. Simulation is embedded within aviation, used regularly and routinely for training, rehearsal, certification and revalidation of pilots. Can a paradigm shift in healthcare culture be achieved so that simulation is routinely and regularly integrated into education and practice?
An example of a national effort that uses simulation to promote patient safety can be found in the Israel Centre for Medical Simulation (MSR).69 Established in 2001, this centre's mission is to improve patient safety and change the culture of health professional education within the Israeli medical system. The centre provides a virtual medical environment with the ability to simulate a range of clinical settings (both prehospital and inpatient settings such as intensive care units, emergency rooms, wards, operating rooms and clinic rooms). There is an extensive network of audio-visual equipment for debriefing purposes, as well as one-way mirror observation booths. Both low-tech, such as basic manikins and actors, and high-tech, such as full-body computerised anaesthesia simulators and virtual reality laparoscopic simulators, are utilised.
Currently, over 7000 health professionals are trained at the centre every year, including doctors, paramedics, nurses, pharmacists, social workers, health managers and occupational therapists. The centre is also used for national high stakes simulation-based performance assessment applications including the selection of medical students, by probing of their humanistic qualities, and in board exams for anaesthesiologists, paramedics and advanced nursing in multiple nursing specialities.70 A wide range of medical specialities are covered in over 100 national training programmes, as well as a broad set of skills (communication, teamwork, procedure-based, management, coping under stress, ethical reasoning such as error disclosure, informed consent and apology). Significantly, all medical students complete a 5-day course at MSR before starting their internship. This includes challenging scenarios that interns might face in their early years as doctors, such as emergency scenarios during patient transport, various acute life support scenarios, as well as difficult human interactions such as managing a patient who is threatening suicide or disclosing an error. The key emphasis of this preintern programme is improving the hands-on skills and clinical readiness of interns and their awareness to medical error identification and patient safety. The success of this centre underscores the need for rationalisation and sharing of efforts.
Cost-effectiveness of simulation
The development of a simulation centre is a costly undertaking. At present, the majority of simulation centres are funded through research grants, commercial support and charitable donations. Although it is an appropriate and important research exercise to define the cost-effectiveness of simulation-based training, it might be more appropriate to develop a framework that can provide ideas for training within the local context. Cost of training is also an important issue with respect to efficiency of medical throughput—training someone to do a procedure adds time to the procedure. In terms of additional time in the operating room alone, Bridges and Diamond in 1999 calculated this to add almost US$48 000 to the cost per graduating resident.71 When extrapolated to over 1000 graduating residents per year in the USA, this makes the annual cost of training residents in the operating room US$53 million. By contrast, increasing the use of simulation in nursing programmes is being considered as a cost-effective method to expand capacity.
The concept of training in a simulation laboratory and subsequent reduction in time to achieve proficiency in the clinical environment is not new. The nuclear industry runs regular simulation exercises to train their workers for mass incidents. This is cost-efficient and safer for workers and the public. A cost-effectiveness argument can thus be proposed for training junior practitioners using simulation, not only in terms of their technical skills but also in terms of their communication, leadership, professionalism and clinical judgement. The ‘trained novice’ is thus proposed to have a shorter learning curve in the real environment, leading to increased productivity and potential decreases in medical error.
An understanding of the cost-effectiveness of simulation shall certainly enable trainees, experienced practitioners, institutions and health systems to make more informed choices with regard to the use of simulation-based medical education programmes. However, educational space is at a premium, and the tools are expensive. There are only a handful of companies working in the field of simulation technologies, and their customers are also strapped for funding. In order to dramatically advance the concept of simulation as applied to medicine, it is necessary for significant seed funding to be provided for research, development and implementation of such tools and curricula. There is a need to lobby and engage governments to resource the technologies, and to provide adequate financial support to enable learners and faculty to work in appropriately designed simulation environments.
Equally, although modern high-tech simulators are very expensive, training on much cheaper low-fidelity simulators can be just as effective. Low-fidelity simulation has huge potential to be used widely throughout the world with a significant impact on training and patient safety. For example, Helping Babies Breathe (HBB) is an evidence-based curriculum in neonatal resuscitation for use in resource-limited areas (currently in Kenya and Pakistan).72 The curriculum was developed by the Global Implementation Task Force (GITF) of the American Academy of Pediatrics in response to the need for an evidence-based, renewable, harmonised training programme in neonatal resuscitation. The programme was designed to meet the challenge of a WHO Millennium Development Goal to reduce child mortality by two-thirds from 1990 to 2015. This global curriculum is designed to be used by skilled birth attendants who are responsible for the care of both the woman and the newborn infant at delivery, and who might not have assistance from a second trained helper. Simple, but effective, task trainers (less than US$100) are being used to train providers (skilled birth attendants), obtain feedback through practice and written and oral testing, and sustain the training.
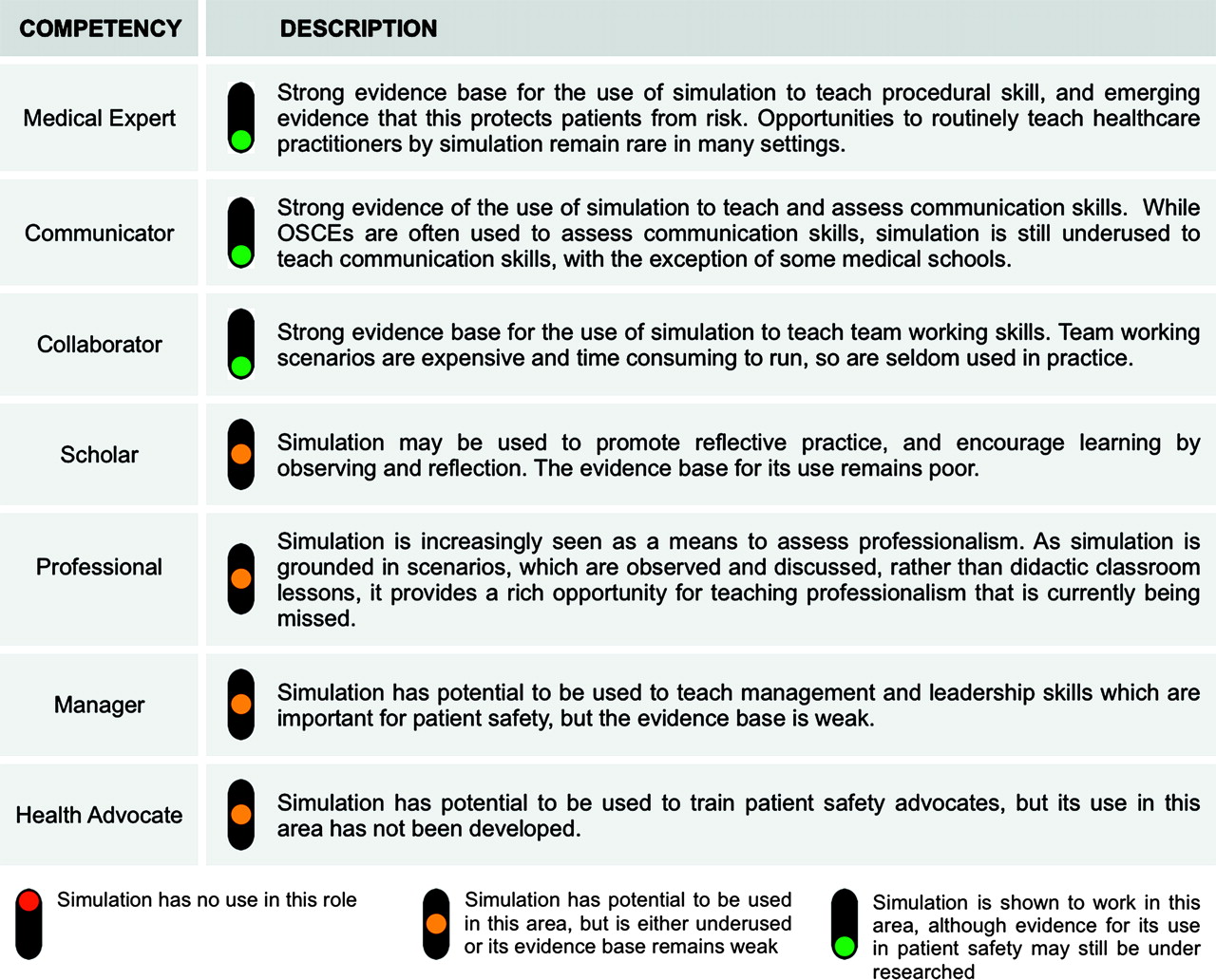
A simulation report card: patient safety
On the basis of current simulation techniques and their application within different domains of healthcare, a report card had been defined based on the framework of seven competencies (figure 4). It has been shown that simulation can already promote the competencies of medical expert, communicator and collaborator; however, further work is required to develop the exact role of simulation as a training mechanism for scholarly skills, professionalism, management and health advocacy.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Simulation report card for patient safety. Through the process of expert consensus and literature review, a ‘traffic light system’ was employed to define the potential of simulation-based medical education to train each of the seven desired competencies within the CanMEDs framework. The traffic lights were defined as follows: red, simulation has no use in this role; orange, simulation has potential to be used in this area, but is either underused or its evidence base remains weak; green, simulation is shown to work in this area, although evidence for its use in patient safety might still be under-researched.
Conclusions
The report card for simulation as applied to patient safety is positive. Since the development of bench-top workshops and anaesthetic scenarios, there have been rapid advances in the technology, augmented availability and a growing belief that simulation is a useful and appropriate tool for training healthcare practitioners of the future. Although high-tech simulators are exciting, to date most advances in simulation have been made through low-fidelity, low-cost approaches. This is important because simulation has tremendous potential to be used globally, removing the patient from the healthcare practitioner's learning curve and improving patient safety. A good example of the growing use of low-tech approaches is Fundamentals of Laparoscopic Surgery (FLS), a new system to assess competence in laparoscopic surgery.73 As of July 2010, every graduating surgical resident in the US must have demonstrated proficiency in FLS before the completion of a general surgery residency, setting a bar that is objective and standardised across the country.
Nonetheless, simulation-based medical education should not be viewed as a panacea or silver bullet to solve current challenges within the healthcare system: working hours restrictions, patient safety, quality and service targets and the emergence of new technologies. Although simulation-based training can certainly extinguish the early part of the learning curve, instil the adoption of safe practices and reduce patient harm, it is unlikely that simulation will replace the importance of key clinical experiences, and learning from them. Furthermore, the road to expertise might only be achieved through clinical practice rather than repeated exposure within the simulation laboratory.
Ultimately, the major challenge to adopting simulation-based training is to show that a difference is being made on real clinical outcomes. This is difficult for a variety of reasons and might only become evident through inferential studies. This, however, should not thwart efforts to analyse the benefit of simulation in real-world outcomes, such as lymph node harvest as a measure of quality cancer surgery, central line infections or stillbirth deliveries. An alternative approach is to initiate the use of simulation, without the need for robust clinical data on its effect. This is a strategy that has been used in a variety of settings. Arguably, the use of simulation in a national setting, for example in Israel, has dramatically affected the safety culture in a positive way, as evidenced by the sheer number of healthcare personnel who attend the simulation centre daily.69
In the macro environment, it is likely that simulation-based training will become the norm. Practising in an environment where it is permissible to make mistakes, and being able to do so repetitively and deliberately, will improve training outcomes. Performing 100 simulated colonoscopies and achieving a predetermined performance benchmark of proficiency is likely to enable an individual to perform their first case on a real patient in an acceptable manner, under guidance and supervision from a properly qualified trainer.
It is necessary for simulation-based training to be fully integrated and funded within training programmes for clinicians at all stages. It is also necessary to train the trainers through the development of a skilled faculty of expert clinical facilitators, supported by adjunctive support staff in dedicated simulation suites. Further research is needed to extend the use of simulation to serve as a tool in identifying suboptimal performers, credentialling, revalidation and learning new technologies. There must also be a move away from using experience as a proxy for competence and, on a continuous basis, to analyse a practitioner's skills. Simulation, therefore, has an immense capacity to become an integral part of the drive to build a safer healthcare system for patients everywhere.
References
Footnotes
Funding The project was funded by WHO Patient Safety.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.