Article Text

Abstract
Objectives To compare the prevalence of use of potentially inappropriate medicines (PIMs) between older patients living in their own homes versus those living in nursing or residential homes, and to test the association between exposure to PIMs and mortality.
Design Cohort study stratified by place of residence.
Setting Tayside, Scotland.
Participants All people aged between 66 and 99 years who were resident or died in Tayside from 2005 to 2006.
Main outcome measures The exposure variable was PIM use as defined by Beers' Criteria. All cause mortality was the main outcome measure.
Results 70 299 people were enrolled in the cohort of whom 96% were exposed to any medicine and 31% received a PIM. Place of residence was not associated with overall risk of receiving PIMs, adjusted OR 0.94, 95% CI 0.87 to 1.01. Exposure to five of the PIMs (including long-acting benzodiazepines) was significantly higher in nursing homes whereas exposure to five other PIMs (including amitriptyline and NSAIDs) was significantly lower. Exposure to PIMs was similar (20–46%) across all 71 general practices in Tayside and was not associated with increased risk of mortality after adjustment for age, gender and polypharmacy (adjusted OR 0.98, 95% CI 0.92 to 1.05).
Conclusions The authors question the validity of the full list of PIMs as an indicator of safety of medicines in older people because one-third of the population is exposed with little practice variation and no significant impact on mortality. Future studies should focus on management of a shorter list of genuinely high-risk medicines.
- Medication safety
- nursing homes
- patient outcomes
- primary care
Statistics from Altmetric.com
Introduction
Patients aged over 65 have the highest burden of illness, and therefore require drug-based interventions to prevent or treat multiple medical conditions.1 Unfortunately, older people may be prescribed unnecessary drugs; drugs that are contraindicated for their age group; or wrong dosages for their age.2 Such medication is characterised as potentially inappropriate medicines (PIMs) and is a concern for several reasons. Patients may receive an array of different drugs, many from different drug classes that increase the risk of iatrogenic harm, particularly in patients with multiple morbidities.3–5 A further consequence of PIMs is that an unrecognised side effect from a PIM drug may be mistaken for a new symptom for which another drug is initiated, leading to a ‘prescribing cascade’ and further iatrogenic harm.6
A particularly vulnerable group are patients in long-term institutional care (nursing and residential homes) because of their higher level of physical and mental impairment requiring drug treatment. Previous work shows that nursing home residents receive up to four times as many prescription items as people living in their own home and take, on average, five or more medicines.7–9 General practitioners (GPs) are responsible for the delivery of medical care to older patients in nursing homes. In the last 20 years there has been anxiety that ‘downsizing’ of NHS provision has increased demand on GPs in a group of patients with high morbidity and disability9–11 and that the delivery of care to nursing homes has become inconsistent and idiosyncratic.3
Particular concerns are raised about the risks of PIMs and medication error for patients in long-term residential care as there is evidence that poor monitoring of disease and prescription of unnecessary and inappropriate medication is more likely to occur in these patients, even after adjusting for multiple morbidity.12 13
In this observational study in Tayside, Scotland, the authors investigated whether there were differences in PIMs (globally and across different classes of PIM drugs) between older people living in their own home compared with people living in nursing or residential homes. They also assessed whether receiving a PIM was associated with an increased risk of death.
Methods
Identification of study cohort
The authors carried out this study using anonymised healthcare data for the population of Tayside, Scotland. These data are managed by the Health Informatics Centre (HIC) of the University of Dundee. HIC maintains internationally recognised record-linkage databases for approximately 400 000 individuals in 74 general practices. It links patient data by means of a community health identifier (CHI) allocated to all patients when they register with a GP. The CHI number allows individual patient data from separate databases (dispensed prescribing, hospitalisation, laboratory results and death certification) to be linked.14
All patients aged between 66 and 99 years and resident in Tayside on 1 January 2005 were identified. Patients aged 100 years or older and patients who moved out of the area during the study period (2005–2006) were excluded from the study. To determine whether a patient lived at home or in a care home, a list of addresses was compiled for all nursing homes, residential care homes and mixed care homes in Tayside. Care home lists were obtained from the relevant councils and hospitals in the area, and cross-checked with the local telephone directory to ensure that all homes had been identified. Care home addresses were compared with electronic patient addresses held by NHS Tayside (as of May 2005). If a patient's address did not match one of the addresses of the care homes, they were classed as living in their own home. This was carried out using a computer algorithm, but 377 addresses were manually checked where there was still uncertainty.
Data from all prescriptions encashed in Tayside during the 2-year study period (2005–2006) for each patient were obtained (approximately 5 million). The information available included CHI number, the drug name, prescription date and British National Formulary code. Demographic data including patients' age and sex were obtained from the master CHI file.
Measurement of potentially inappropriate medicines
The authors used the updated Beers' Criteria to identify PIMs.15 These refer to a set of drugs and contexts that was devised in the United States in relation to PIMs in older people. They are the most widely recognised explicit process measures for inappropriate medicines. Although approximately half of the drugs on the Beers list are not available in Europe, use of these criteria has the advantage of enabling international comparison.16 Additionally, Beers' Criteria PIMs have been categorised and labelled by potential adverse outcomes of either low or high severity. For the purposes of this study, Beers' Criteria drugs were adapted so that drugs/drug names not used in the UK were replaced with the UK equivalent. A pharmacist was involved throughout this process and authorised any modifications that were made. Prescribing records were examined and prescriptions for drugs included in the Beers' Criteria were extracted. The numbers of prescriptions per patient were then calculated, along with the total number of different drug classes, grouped by the British National Formulary, as a proxy for multiple morbidities.
Four of the Beers' Criteria drugs included in the analyses were dependent on the dose of the prescribed medication. Directions regarding dose information were only available for registered diabetic patients in Tayside. The total numbers of these patients receiving the relevant drugs were retrieved. The proportion of patients that exceeded the recommended daily dose (Beers' Criteria) was calculated for the subset of patients whose dose information was available. An estimate of the proportion of patients in the total population who would exceed the criteria was then extrapolated from this subset of patients. The number of PIMs prescribed to each patient was also calculated. Dose related criteria for individual patients were only counted if the dose information was present and exceeded the recommended daily dose.
Statistical methods
Descriptive statistics of individuals living at home and in care along with the proportion receiving Beers' Criteria PIMs in these respective settings are described.
The association between place of residence and number of PIMs received using proportional odds models, both unadjusted and then adjusted for age, sex and comorbidity was assessed. The reported ORs relate to the likelihood of having a worse outcome (number of PIMs) across the range of possible categories. The authors also assessed the independent effects of demographic variables, number of drugs prescribed and place of residence in terms of probability of receiving a Beers' Criteria PIM.
In addition, individuals were grouped by an anonymous code representing their practice so that variability by practice of the proportion of elderly patients who had received one or more PIM was described. To examine the effect of clustering, the logistic regression model was repeated with the patients clustered by anonymous practice code, with a random effects model fitted.
Descriptive statistics and associations were assessed in terms of cumulative number of Beers' PIMs and place of residence by means of ordinal logistic regression. Overall and specific types of Beers' Criteria PIMs in relation to place of residence were also assessed using logistic regression analysis and adjusting for age, sex and polypharmacy. Last, logistic regression analysis was performed to investigate the impact of receiving at least one Beers' Criteria PIM on all cause mortality after adjusting for place of residence, age, sex and polypharmacy.
Results
Descriptive statistics
A total of 70 299 patients aged 66–99 years were resident in Tayside, Scotland, between 2005 and 2006. Of this 4557 (6.5%) were living in care, 2230 (3.2%) in nursing homes, 1799 (2.6%) in residential care and 528 (0.8%) in mixed care homes. Patients living in care were almost five times more likely to die, were predominantly female and were significantly older than patients living at home. Over the course of the 2-year period studied, patients received a median of 55 prescriptions (IQR 26–95), with 6% receiving no prescriptions, 27% receiving medications for between one and five different drug classes and 67% receiving medications from six or more drug classes. Patients living in care received almost twice as many prescriptions as patients still living at home and received a higher number of prescriptions from different drug classes (table 1).
Descriptive statistics of patients aged 65 years and older living in Tayside, Scotland, 2005–2006
Beers' Criteria drugs overall
The majority of Beers' Criteria drugs (n=19, 58%) were deemed not to be relevant for further analysis either because the drug was not prescribed in Tayside or was prescribed to very few patients (<0.5% of study population). These drugs were excluded from further analyses and are listed separately (web table 1).
When prescription of the remaining 14 Beers' Criteria drugs were assessed, patients living in care homes received more PIMs with a mean of 0.49 prescriptions, compared with a mean of 0.41 prescriptions for patients living at home (p<0.001); in absolute terms 1690 (37.1%) patients in care home received a PIM during the 2-year period of observation compared with 20 304 (30.9%) living at home (table 2). After adjustment for age, sex and polypharmacy, patients were more likely to receive at least one PIM if they were younger, female and had higher polypharmacy. However, place of residence was not independently associated with likelihood of receiving PIM when measured as a binary variable (none vs. any PIM) (table 3).
Number (percentage) of patients receiving prescriptions of PIMs by place of residence
Relationship between receiving a PIM with demographic variables, number of drugs prescribed and place of residence
Practice level prescribing of Beers' Criteria drugs
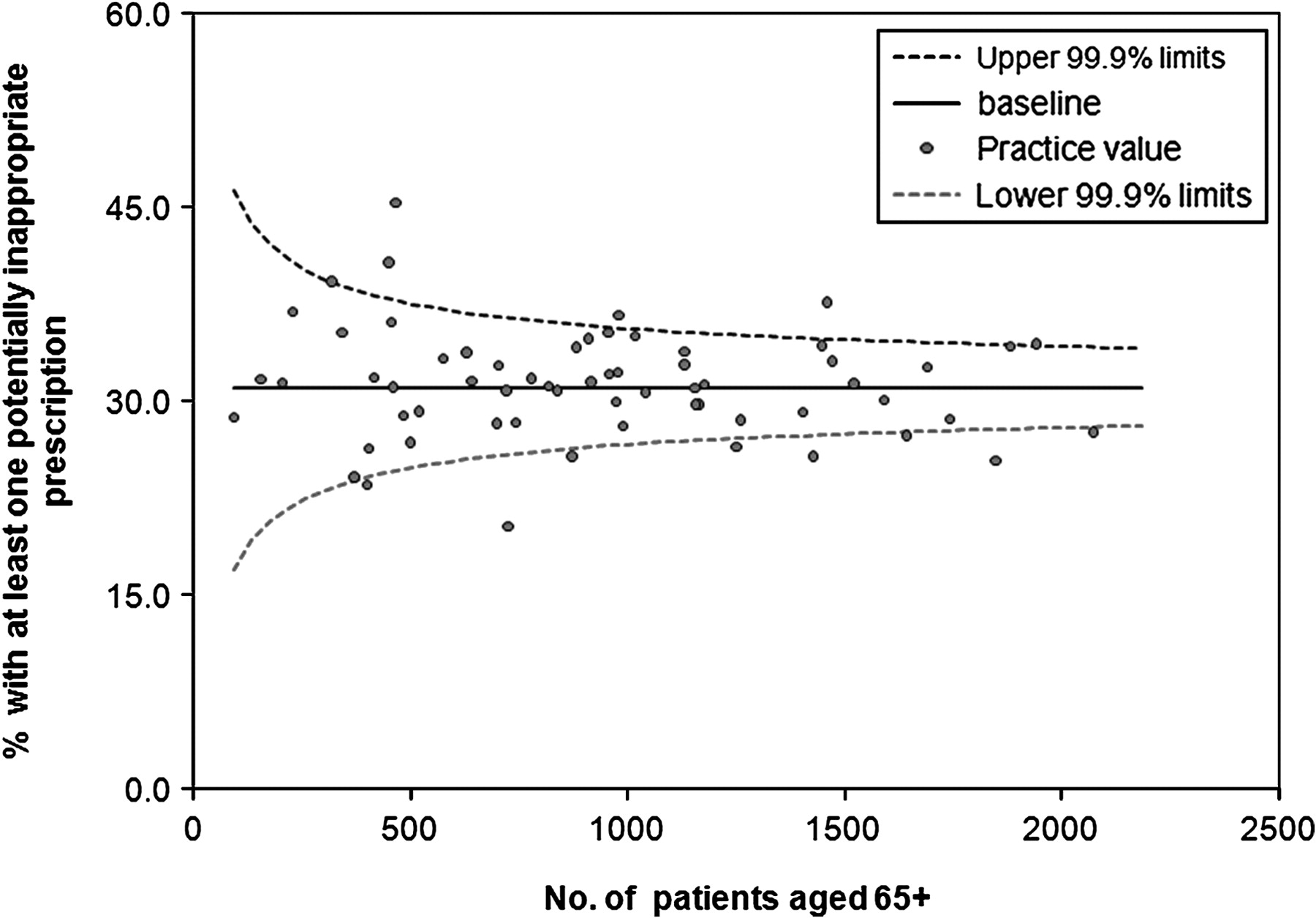
A reasonably consistent pattern emerged across the 71 Tayside practices, with 20–46% of their practice population aged >65 years receiving at least one Beers' Criteria PIM during the 2 years of the study (figure 1).

{kind=link}
Practice level prescribing of Beers' Criteria drugs.
Drug-specific Beers' Criteria
Overall, 37.1% of patients in care received a Beers' Criteria PIM compared with 30.9% at home. Amitriptyline (7.6%), ferrous sulphate (7.1%) and long-acting benzodiazepines (6.7%) were the three most commonly prescribed PIMs among patients aged 65–99 years in Tayside (table 4). The authors identified statistically significant differences by place of residence for certain drug-specific PIMs. Psychotropic PIMs such as long-acting benzodiazepines, and fluoxetine as well as muscle relaxants, (methocarbomol and oxybutynin) nitrofurantoin and dipyridamole were prescribed more frequently to patients living in care while amitriptyline, nonsteroidal anti-inflammatory drugs (NSAIDs), gastrointestinal antispasmodics doxazosin and cimetidine were prescribed more often to patients living at home (table 4). The ORs generally reduced after adjusting for other risk factors, but independent effects of place of residence were still evident.
Beers' Criteria for specific PIMs by place of residence
Beers' Criteria and all cause mortality
After adjusting for place of residence, age, sex and polypharmacy by means of logistic regression, receiving at least one Beers' Criteria PIM did not lead to an increased risk of mortality, with an OR of 0.98 (95% CI 0.92 to 1.05). As anticipated, patients living in care, older patients and patients with additional polypharmacy were more likely to die, with ORs of 3.48 (95% CI 3.24 to 3.75), 1.10 (95% CI 1.10 to 1.10) and 1.03 (95% CI 1.02 to 1.03), respectively. Women were less likely to die compared with men, with an OR of 0.63 (95% CI 0.60 to 0.67).
Discussion
Statement of principal findings
This study shows that use of prescription medicines is high in older patients in Tayside, who receive on average 70 prescriptions over 2 years, with almost 70% of patients receiving prescriptions from six or more drug classes. Beers' Criteria PIMs occur for over a third of the >65 population; and this level of PIM is consistent across all Tayside practices (figure 1). Patients are at increased risk for receiving a Beers' Criteria PIM if they are younger, female and have increased polypharmacy. No evidence was found to suggest that place of residence influences the overall risk of receiving a Beers' Criteria PIM, however cumulative risk of PIMs is associated with place of residence (table 2). A pattern emerges in relation to drug-specific PIMs with psychotropic drugs being more commonly prescribed in residential/nursing home care settings (aside from amitriptyline). All cause mortality is not independently associated with the 13 UK relevant Beers' PIMs.
Strengths and weaknesses of the study
The strengths of this study are that it allows a complete assessment of PIM in a defined geographical population enhancing external validity, and describes PIM at the individual and practice level. It also helps in assessing the type of PIM according to drug class in relation to place of residence. Record-linkage enables assessment of PIM in relation to all-cause mortality.
There are some shortcomings to this study. The encashed prescribing information only had completed dosage instructions for the population members who were diabetic. For Beers' Criteria PIMs, which required dosage information, the reported prevalence was measured in diabetic patients where dosing information was available and then the number of all patients estimated by using this prevalence and the known number of patients receiving that medication. For the remainder of the analysis if dosage information was unknown relating to an individual Beers' Criterion it was assumed the patient did not fail that criterion, so estimates of PIM in relation to dosing are necessarily conservative. In terms of prescribing responsibility, all drugs were prescribed in the community by GPs. However, a proportion of drugs will have been initiated by hospital physicians, and it is not possible to know which drugs were hospital initiated and continued by GPs.
Adjustment for socio-economic status is not made as patients in care homes would not have been accurately characterised. The last address for patients prior to moving into a nursing or residential care home would be required to allow for accurate measurement of socio-economic status and this information was not available. As has been observed in studies of PIM in the UK, Beers' Criteria do not apply to the majority of drugs used in UK settings (not available or low level of usage). However, use of these criteria is the most widely used explicit process measure of PIM and does enable between-country comparison.16 The authors did not have access to morbidity diagnoses and used number of medications as a proxy measure. Last, as patients were followed-up for a 2-year period only, the lack of association between PIM and all cause mortality should be treated with caution.
Context of other studies
The findings from this study are broadly consistent with previous research into PIMs in elderly people, confirming a high prevalence, despite the recognition and ongoing concerns about the iatrogenic harms associated with PIMs.2 16 In addition, specific drugs that are known to increase risk in older patients continue to be prescribed at relatively high rates, for instance, amitriptyline and long-acting benzodiazepines.17 18 This study also suggests that younger age, being female and polypharmacy were the biggest predictors for receiving PIMs. These results are partly consistent (association of PIMs with female gender and polypharmacy) and partly at odds (not associated with advancing age) with a recent English study.19 The most consistent finding relates to polypharmacy, which in itself is likely to be a marker for multi-morbidity.
The study findings show no association between Beers' Criteria and mortality, which is in contrast to the findings of two earlier papers.20 21 However both of these papers were in populations of nursing home residents only and one had a significantly smaller population. The present study adjusted for place of residence along with polypharmacy, gender and age and found no effect.
Last, the findings concerning prescription of long-acting benzodiazepines have been a consistent cause for concern in terms of patients in care homes and remains one of the most common PIMs with a significantly higher prevalence in care home patients (table 3).
A recent review of appropriate prescribing in older patients suggested that the criteria for medicine safety should ‘constitute a floor of quality below which no patient should go’. From the study data it can be seen that every practice is exposing a minimum of 20% of patients at risk to these medicines so there is clearly unanimous disagreement that the Beers' Criteria do constitute a floor of quality.16 Controversy exists over some of the medications considered by Beers to be inappropriate, the latest update suggests that cost containment has been a major driver, and it has also been argued that the Beers' Criteria do not address all aspects of PIMs in older people.18 22 23 Despite this, the Beers' Criteria remain one of the more commonly used tools for assessing PIMs in older patients although whether or not the criteria act as good indicators for adverse drug events remains unclear. Definitions concerning medication error have also been described, with categorisation into serious, life-threatening or fatal events.24 Modification of these types of criteria has been used successfully in the measurement of care in nursing/residential homes in the UK.13 Finally, more research is needed from European-based PIP criteria that encompass representative drugs prescribed in a European context.16 25–27 Future studies should also focus on the clinical context of prescribing, linking the clinical indication to the drug prescribed. These studies should also incorporate follow-up details that relate to important patient-centred outcomes such as quality of life and self-reported adverse effects.
This analysis should be viewed as a screening study that highlights potential problems and avoidable consequences of PIMs, for instance, diminished quality of life and admission to hospital as a consequence of an adverse drug reaction. All prescribing decisions have an element of risk and benefit and what may be classified as a PIM may actually be in the patient's best interest in some circumstances. However the high level of use of PIMs and the consistent pattern emerging from this and other studies show that an almost inevitable consequence of polypharmacy in an individual patient is likely to be the prescription of a PIM.19 Further research is needed to develop European-specific prescribing indicators that link to important patient outcomes in terms of quality of life and avoidance of adverse drug reactions.
Implications for practice and future research
Adverse drug reactions in older patients are recognised as a substantial cause of preventable illness and features as a priority for health research in terms of improving patient care into the 21st century. With an ageing population that is at increasing risk of developing multiple morbidities as they grow older, a strategy is needed to screen and select those individuals at greatest risk of adverse drug reactions. It seems that age alone is not likely to be an independent risk factor: multiple morbidity requiring polypharmacy is emerging as the single largest factor associated with PIMs with a consequent risk of adverse drug reactions.28 Utilising strategies to enhance suitable point of care prescribing in hospital and community settings, and alerting prescribers to the risk of PIMs either through computerised decision support systems, education and training programmes or the enhanced role of pharmacists to support improvements in the quality of prescribing are initiatives that will require ongoing investment and assessment.29
Conclusion
This population-based study shows that older patients continue to receive high levels of PIMs. Polypharmacy emerges as a consistent risk factor associated with such medicines. Further research is needed to ensure a coordinated approach, at the policy and individual level, so that PIMs in older patients can be avoided and contained.
Acknowledgments
The authors thank Alison Bell and Duncan Heather of the Health Informatics Centre, University of Dundee, for anonymisation, record linkage and other procedural assistance in preparing the dataset; Peter Donnan, Bruce Guthrie, Dougie McPhail, Marie Pitkethley, Clare Stubbings and Frank Sullivan for advice throughout the project in their roles as steering group members.
References
Footnotes
Funding EastRen Project Grant 141-07, Scottish School of Primary Care, Mackenzie Building, University of Dundee, Kirsty Semple Way, Dundee, DD2 4BF.
Competing interests None.
Ethics approval This study was conducted with the approval of the Tayside Research Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.