Article Text

Abstract
Background Our centre's median forced expiratory volume in one second (FEV1) reported in the 2005 Cystic Fibrosis (CF) Foundation Patient Registry was below the national median. The focus of our quality improvement initiative was to improve lung function through re-education of airway clearance techniques (REACT).
Aim The global aim was to improve the median FEV1 in our patients. The specific aim was to encourage adherence to airway clearance techniques (ACT). To achieve these goals we implemented the REACT programme for patients.
Methods Educational sessions introduced the concept of improving clinical outcomes and the importance of airway clearance in achieving optimal lung function. The REACT programme utilised an anonymous survey, in-clinic questionnaire and ACT demonstration to assess knowledge, practices and barriers to ACT. Patients were then categorised as non-adherent or adherent with correct or incorrect technique. Improper techniques were corrected. All patients were re-educated on the rationale for ACT.
Results Our surveys revealed that 43% of patients had barriers to ACT and 53% were non-adherent. Following implementation of REACT, median FEV1 increased from 84% to 92% (national median 91–94%) from 2005 to 2010 for patients aged 6–17. For patients 18 and older, median FEV1 increased from 56% to 64% (national median 62–65%) from 2005 to 2010.
Conclusions By introducing a programme focused on technique and adherence, we were able to improve median FEV1 in patients with CF. Sustained improvement of FEV1 was accomplished by continued use of the REACT programme.
- Quality Improvement
- Clinical Microsystem
- Compliance
Statistics from Altmetric.com
Introduction
Cystic fibrosis (CF) is an autosomal recessive, inherited disorder. It is characterised by respiratory, gastrointestinal and exocrine gland dysfunction. Patients with this condition have thick, viscid mucous secretions that cause airway obstruction and lead to the development of chronic, progressive infection, inflammation, and eventual damage to the airways. Daily pulmonary therapies for CF are important in clearing airway secretions and slowing the decline of lung function. These therapies include inhaled medications, antibiotics and airway clearance techniques (ACT).1 As reported in the literature, adherence to prescribed therapies for CF is sub-optimal.2 Adherence to chest physical therapy was 40–47% in a study by Quittner et al in 2000 and 51% in a study by Modi et al in 2006.3 ,4
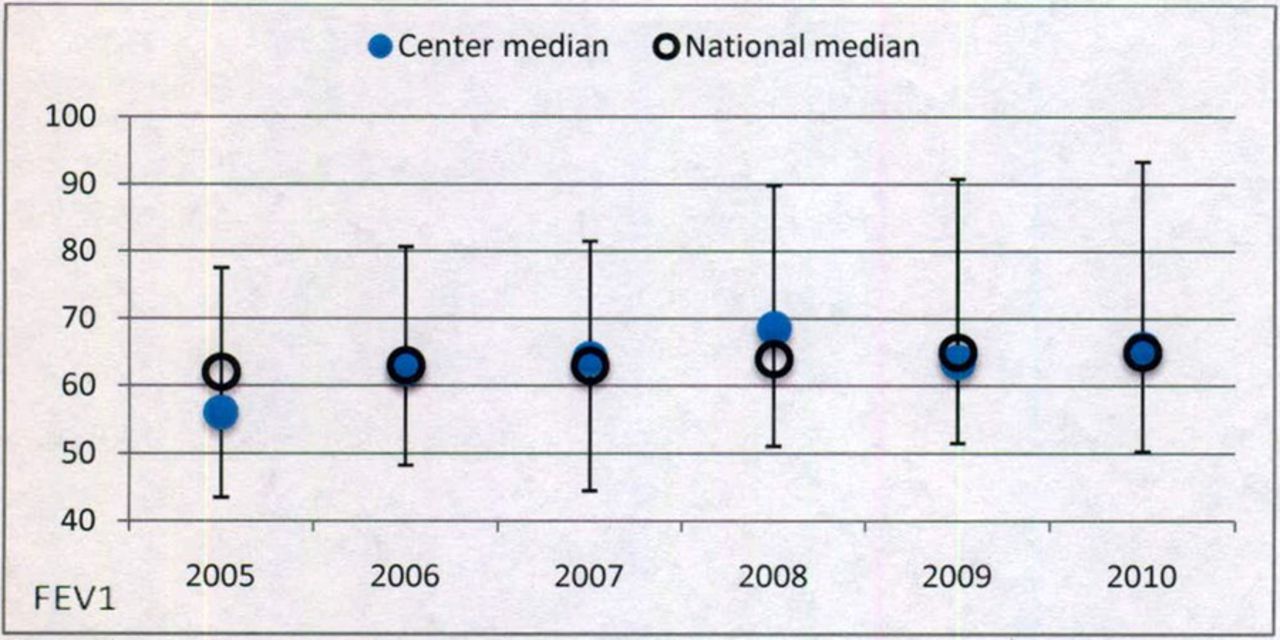
Lung function in CF is assessed by monitoring forced expiratory volume in the first second (FEV1), which is a reliable and reproducible measurement. The pulmonary goal in CF care is to maintain normal lung function as long as possible. In a study by Kerem et al, patients with an FEV1 less than 30% of predicted have a 50% chance of dying within 2 years.5 Our 2005 Cystic Fibrosis Foundation (CFF) centre specific data revealed that the median FEV1 expressed as percentage predicted for our patients was below the national median.6 For patients 6–17 years of age the median FEV1 percentage predicted was reported as 84%, while the national median was 91%. Our centre's median FEV1 for patients 18 and older was 56% of predicted as compared to the national median of 62%. Having identified lung function as the target for improvement, we hypothesised that one of the causes for our centre's FEV1 being below the national median might be due to poor adherence to ACT.
The global aim of this quality improvement (QI) initiative was to increase our median FEV1 to reach the national median. To accomplish this we needed to assess to what degree our patients were non-adherent to ACT and what barriers they encountered in performing ACT. Our specific aim was to encourage adherence to ACT as a way to increase median FEV1. To achieve these goals we implemented a programme entitled Re-Education of Airway Clearance Techniques (REACT).
Methods
Setting
The setting of this QI project was at the Cystic Fibrosis Center at Monmouth Medical Center, an affiliate of Barnabas Health Care System located in Long Branch, New Jersey.
Ethics
This QI project did not require individual consent from our Institutional Research Review Board (IRB) because all patients had signed consent for inclusion in the CFF Registry. According to the policy activities that constitute research at Monmouth Medical Center, this work met the criteria for operational improvement activities exempt from ethics review.
Planning the intervention
This project began with the formation of a Family Advisory Board (FAB) and QI lead team. Our advisory board consists of 11 people: 5 couples who have children with CF and 1 adult patient. The mission of the FAB is to assist and support the CF centre to provide superior family-centred care by promoting family involvement to strengthen the collaboration between patients and the care team. The QI lead team included 6 CF centre staff members (2 physicians, 2 nurses, 1 respiratory therapist and 1 physical therapist) and representatives from the FAB (4 parents and 1 adult patient). The purpose of the QI lead team was to plan and implement the project. The QI lead team met weekly throughout the entire process. Parent and patient input was invaluable in identifying barriers to ACT adherence. A cause and effect diagram displaying many of the barriers that were identified from the meetings is shown in figure 1.
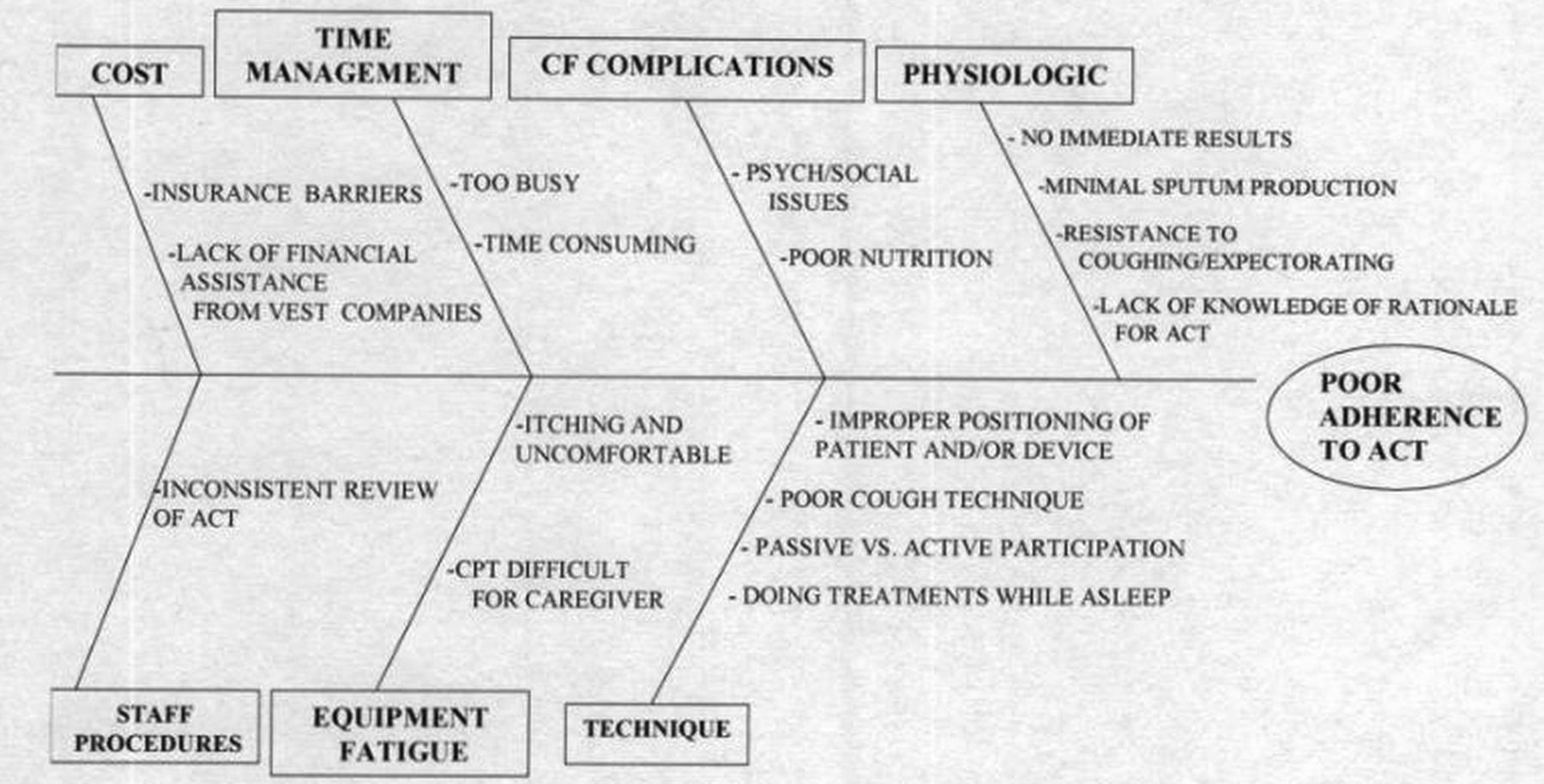
Barriers to airway clearance techniques (ACT).
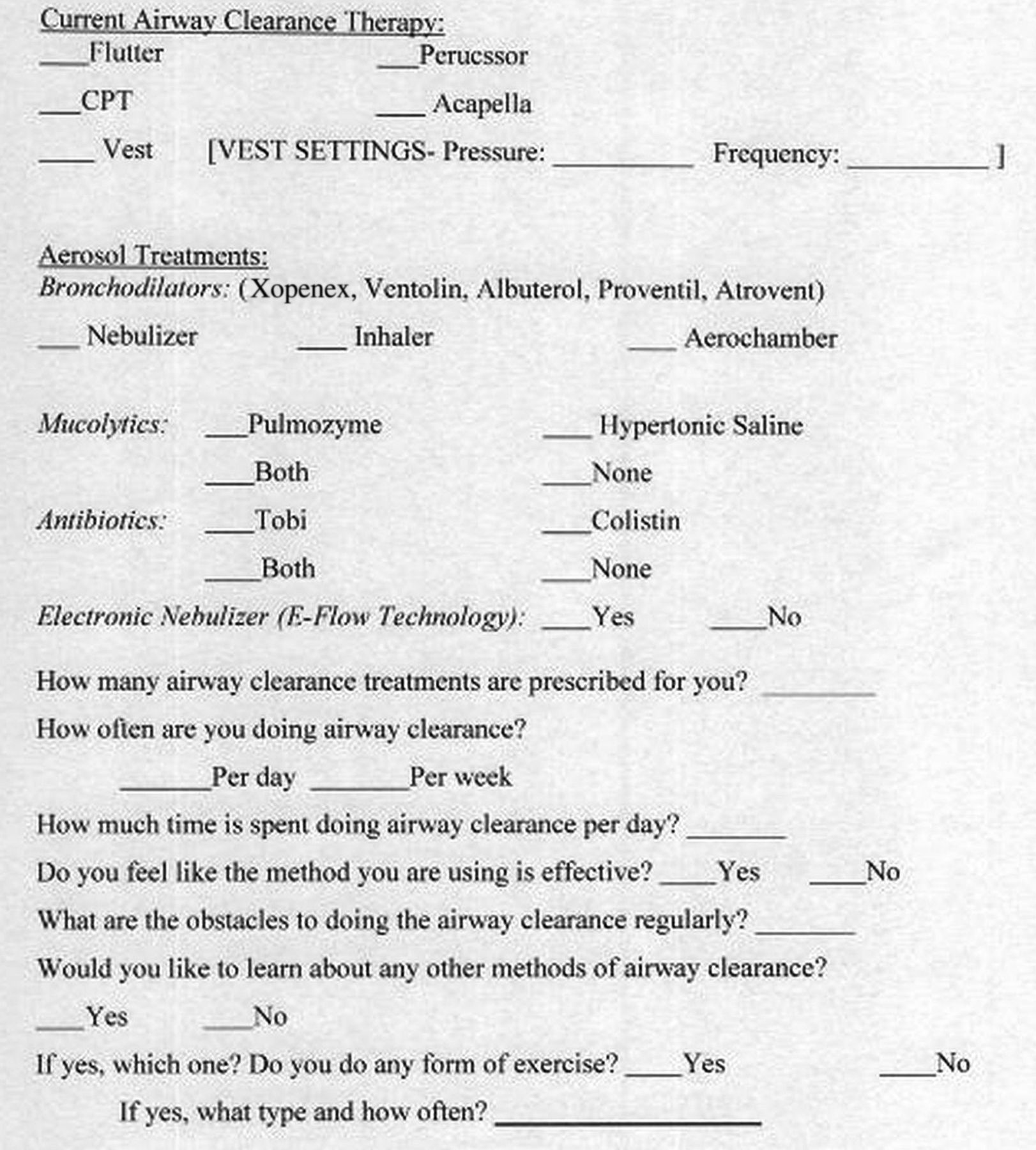
An educational session was held in the spring of 2006 for patients and families. The purpose of this session was to introduce the concept of improving quality of care and the CFF's commitment to assisting care centres in the process. In the summer of 2006 the QI lead team developed an anonymous survey to help us understand common practices, equipment used by patients and barriers that may affect adherence to therapies (figure 2). The survey also included assessment of the knowledge of the rationale for performing ACT. The anonymous survey was mailed home to patients and families with a self addressed stamped return envelope. We opted for anonymity of the survey in order to ascertain an uninhibited reporting of their knowledge and practice of ACT. To ensure a greater return of the survey, we sent out a second mailing of the survey 1 month after the initial mailing.

Anonymous survey.
During this time the QI lead team also developed the components of the REACT programme which was aimed at identifying patients who were non-adherent to their therapies, correcting poor ACT techniques, and assisting patients to overcome barriers to adherence.
After collating the results of the anonymous survey, a letter outlining the REACT programme was sent to all patients and families to introduce the programme and to invite them to attend another educational session scheduled in the fall. This session focused on the rationale for ACT in CF and the available modalities used to maintain optimal lung health. Participation in REACT was encouraged during this event. Subsequently, patients were reminded prior to their regular appointment to bring in their personal airway clearance equipment if they were interested in participating. The equipment included nebuliser compressors, valve holding chambers, inhalers, high frequency chest wall oscillation vest equipment and any other airway therapy devices utilised by the individual.
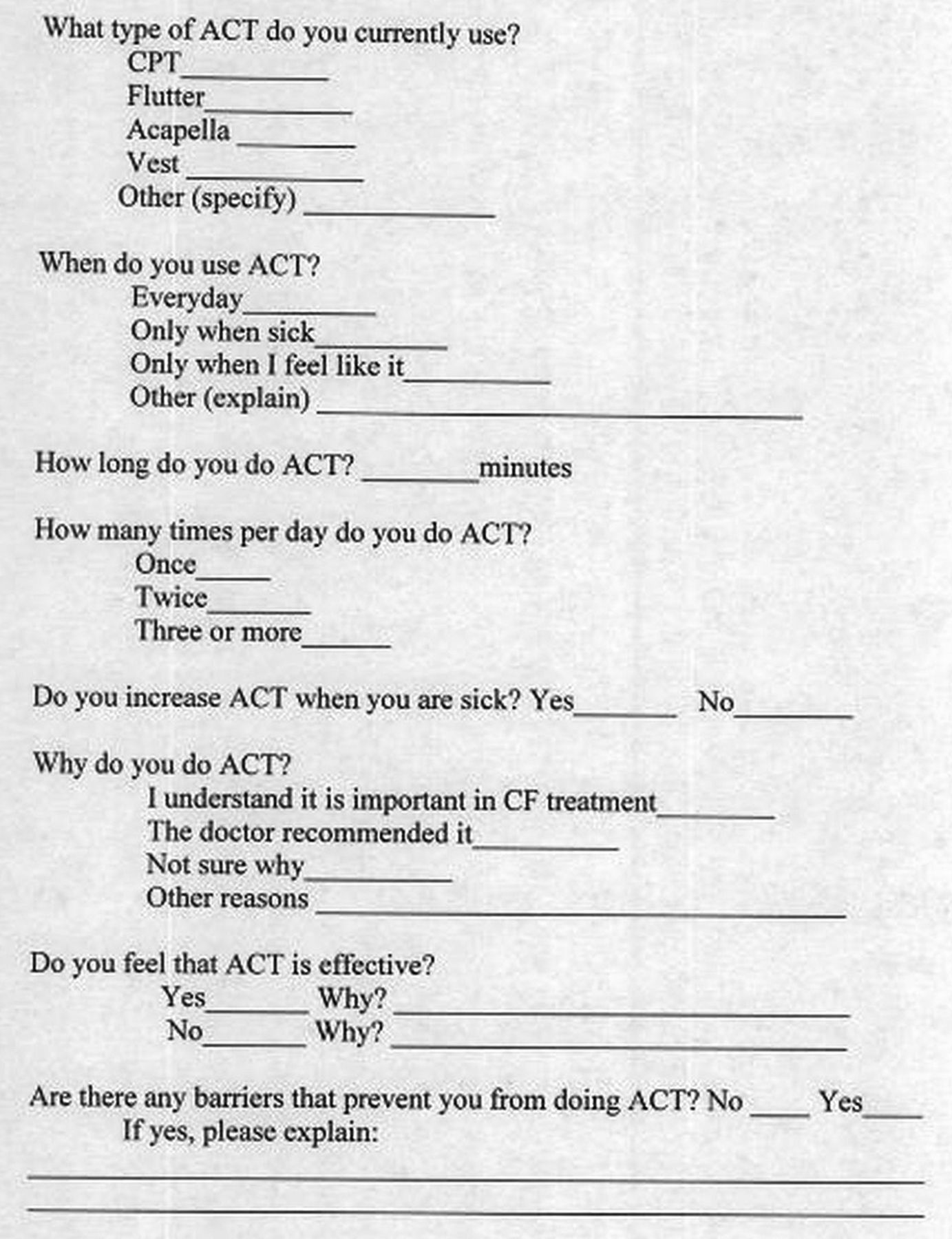
The process consisted of three key steps performed during one clinic visit: (1) an in-clinic ACT questionnaire; (2) patient demonstration of ACT; and (3) a face to face educational discussion. In the first step, patients were asked to complete an ACT questionnaire (figure 3). The questions focused on daily ACT practices, barriers to adherence and satisfaction with current treatment. Patients were encouraged to answer the questionnaire honestly. They were assured that the process was a non-judgemental assessment of their daily routine. Based on the responses to the in-clinic ACT questionnaire, patients were classified as being adherent or non-adherent to their therapies. For the purpose of this project a patient was defined as being adherent to routine therapy if they consistently performed ACT as prescribed by the healthcare provider. This was usually one to two times per day.
Airway clearance techniques (ACT) questionnaire.
The second step of the programme was the patient demonstration of ACT. This included performing aerosol therapies, using inhalers, setting up equipment and utilising airway clearance modalities. Correct or incorrect ACT techniques were determined by our trained CF staff members (respiratory therapist, physical therapist or CF nurses). Prior to the onset of this project, the four staff members assigned to observe the patients reviewed ACT techniques and standardised the assessment. Observed examples of incorrect techniques included: poor posture, talking or singing while taking aerosolised medications, ending treatments before completion, taking inhaled medications out of recommended order, and shortening cycles of high frequency chest wall oscillations.
The third step was the face to face educational discussion. The purpose of this step was to review the rationale for performing ACT and assist patients in overcoming barriers through problem solving. Alternative methods of ACT were offered if they expressed interest. All participants were re-educated on the rationale for performing ACT utilising our educational tool (figure 4). This tool was created by the QI lead team as a hand held flip chart.

Educational tool.
Assessment/implementation of the intervention
Figure 5 shows the algorithm for the work flow of the REACT programme. Based on patients’ responses and ACT performance, patients were further classified as: adherent with correct technique, adherent with incorrect technique, or non-adherent.

Algorithm.
Patients who were classified as adherent with correct technique were reassessed every 2–3 months. Those who were classified as adherent with incorrect technique were shown the correct technique and were asked to return in 1 month for reassessment. The non-adherent patients were shown correct techniques and re-educated about prescribed therapies. Barriers to performing ACT were discussed, and problem solving was used to overcome the barriers.7 Non-adherent individuals were also asked to return in 1 month for reassessment. The purpose of the more frequent follow-up visits was to reinforce the newly corrected techniques. Reassessment was obtained through dialogue and patient demonstration only.
The initial evaluation of the patients occurred during regularly scheduled clinic appointments and added approximately 45 min to the visit. Patients and families were informed in advance that the assessment would extend their clinic time. The staff assessed 2–3 patients per clinic session. No revisions of the algorithm were made throughout the duration of the project. The evaluation process was a 1-year endeavour. Subsequently all participants underwent an annual REACT assessment between 2007 and 2010 which focused on the second and third steps of the programme.
Methods of evaluation/analysis
We utilised the median FEV1 from our CFF centre specific report (2006–2010) as the primary outcome measure. A one sample t test was used to compare our centres’ median FEV1 to the national median FEV1.
Results
At the start of this initiative, our total patient census was 112 combined paediatric and adult patients. Of the 112 patients, 91 were eligible and 83 (91%) participated in the REACT programme. Excluded in this process were six patients who had undergone lung transplantation and eight patients who were not seen in the CF centre during the period of time that REACT was being offered. Fifteen patients under 6 years of age were excluded in the analysis because FEV1 data would not be available due to their age. The parents of these patients were offered the opportunity to complete the questionnaire and demonstrate ACT on their child so corrections could be made as appropriate. All 15 agreed to participate.
We had a 30% return from the in-home anonymous survey. Results revealed that 43% of the responders reported barriers to adherence. Time management, cost, equipment fatigue, medical complications and discomfort were the most common reasons cited. Additional results also revealed that our patients performed ACT less than medically prescribed. We also learned that not all patients understood the rationale for ACT nor did they feel it was effective. The information collected from this survey was used to support our hypothesis that poor adherence to ACT was an issue in our patient population.
Results of the in-clinic questionnaire and patient demonstrations revealed: 37% of patients (31/83) were adherent with correct technique, 10% (8/83) were adherent with incorrect technique, and 53% (44/83) were non-adherent. Additional findings from the in-clinic questionnaire showed that 90% (35/39) of adherent patients and 80% (35/44) of non-adherent patients reported treatments as being effective. Barriers to ACT were reported in 56% (22/39) of adherent patients and 75% (33/44) of non-adherent patients. The most common barrier was finding the time to perform treatments (49%, 41/83). Equipment fatigue was reported in 37% (31/83) of patients.
Our centre median FEV1 for patients 6–17 years in 2005 was 84% (national median 91%) (p=0.029). By the end of 2006 our centre's median FEV1 increased to 93% (national median 92%). In 2007, 2008, 2009 and 2010, the median FEV1 measurements were 91%, 92%, 92% and 92%, respectively (figure 6). These were close to the national median of 93%, 93%, 94% and 94% during those years.

Centre median forced expiratory volume in one second (FEV1) with IQR 6–17 years old.
For our patients 18 years and older, the median FEV1 in 2005 was 56% (national median 62%) (p=0.584). In 2006, this increased to 63% (national median 63%). Our median FEV1 for 2007 was 64% (national median 63%) while the 2008, 2009 and 2010 measurements were 69%, 64% and 66%, respectively. This compared to the national medians of 64%, 65% and 65% for the respective years (figure 7).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Centre median forced expiratory volume in one second (FEV1) with IQR 18 years or older.
Discussion
The REACT programme is an organised approach designed to reinforce the importance of ACT in the daily routine of CF care. The programme follows a simple algorithm, focused on patient assessment and education. An essential component of the REACT programme was the reinforcement of knowledge on an individualised basis. The combination of discussion of responses to the in-clinic questionnaire, observation of airway clearance, identification and correction of incorrect technique as well as utilisation of the educational tool, contributed to the success of the programme.
As stated in our global and specific aims, our ultimate goal was to improve median FEV1 by encouraging adherence to ACT. This was achieved in both our adult and paediatric patients. Our median FEV1 was near or above the CFF national median throughout this project.
Although the median FEV1 for patients 18 years and older was near or above the national median following the REACT programme, the small sample size may be the reason for lack of statistical significance. Further study utilising this programme with a larger number of patients would be helpful to address the impact of such an intervention.
The REACT programme has become an integral part of CF care in our centre. As the treatment burden increases with age we continue to struggle with the issue of adherence. Since there is no single formula to directly measure adherence, we used the median FEV1 as an indirect measurement of adherence. The REACT programme addresses the importance of knowledge and technical skills and encourages adherence but it does not completely solve this complex problem. This may be one of the limitations as to why our centre's median FEV1 has not exceeded the national median.
Several lessons were learned from this endeavour. First, we realised that the perception of adherence varies between patients, families and healthcare providers. Second, the direct involvement of patients and families during the planning phase of this project allowed us to address the social and medical barriers to adherence. Their input was invaluable since they live with the treatment burden that is a daily part of CF care. Third, more frequent clinic visits allowed for closer observation, early detection of pulmonary exacerbations, assessment of their nutritional status and ongoing re-education. Fourth, the in-clinic patient demonstration gave staff the ability to upgrade or replace equipment that was not functioning. Finally, we found that following a simple algorithm helped to maintain consistency in our programme. We believe that clinical outcomes can be sustained with repetition and standardisation of the process.
Conclusion
By implementing REACT, a programme that encourages adherence, provides education and corrects ACT skills we were able to improve and sustain the median FEV1 in our CF patients. The simplicity of this programme makes it easily incorporated into routine CF clinic visits. The standardisation of REACT as an annual review of ACT could prove valuable in improving and maintaining lung function in CF patients.
Footnotes
-
Contributors RLZ EUS, DTD, BM and RB were directly responsible for the conception and design of this quality improvement project. The same team members were responsible for the acquisition, analysis and interpretation of the data. They were all actively involved in the writing, revision and editing of the paper.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.