Article Text

Abstract
Background Handoff miscommunications are a leading source of medical errors. Error rates decreased following implementation of the I-PASS handoff program (a bundled intervention using a structured mnemonic, I-PASS, and other initiatives to sustain implementation) in a pediatric research trial. Whether I-PASS can be implemented in settings outside academic pediatric institutions is unknown.
Objectives To implement I-PASS in a variety of hospitals and medical specialties using a mentored process. (2) To measure the association of I-PASS implementation with handoff quality and provider-reported medical error rates.
Methods We implemented I-PASS in 16 hospitals [community (n=5), academic (n=11)] and multiple specialties [internal medicine (n=7), pediatrics (n=3), other (n=6)]. We paired each site with an external mentorship team of I-PASS experts that conducted a site visit and provided ongoing coaching. Site leads participated in program wide webinars and shared data with participating sites. Validated handoff observation tools and a provider survey assessed handoff quality and rates of adverse events.
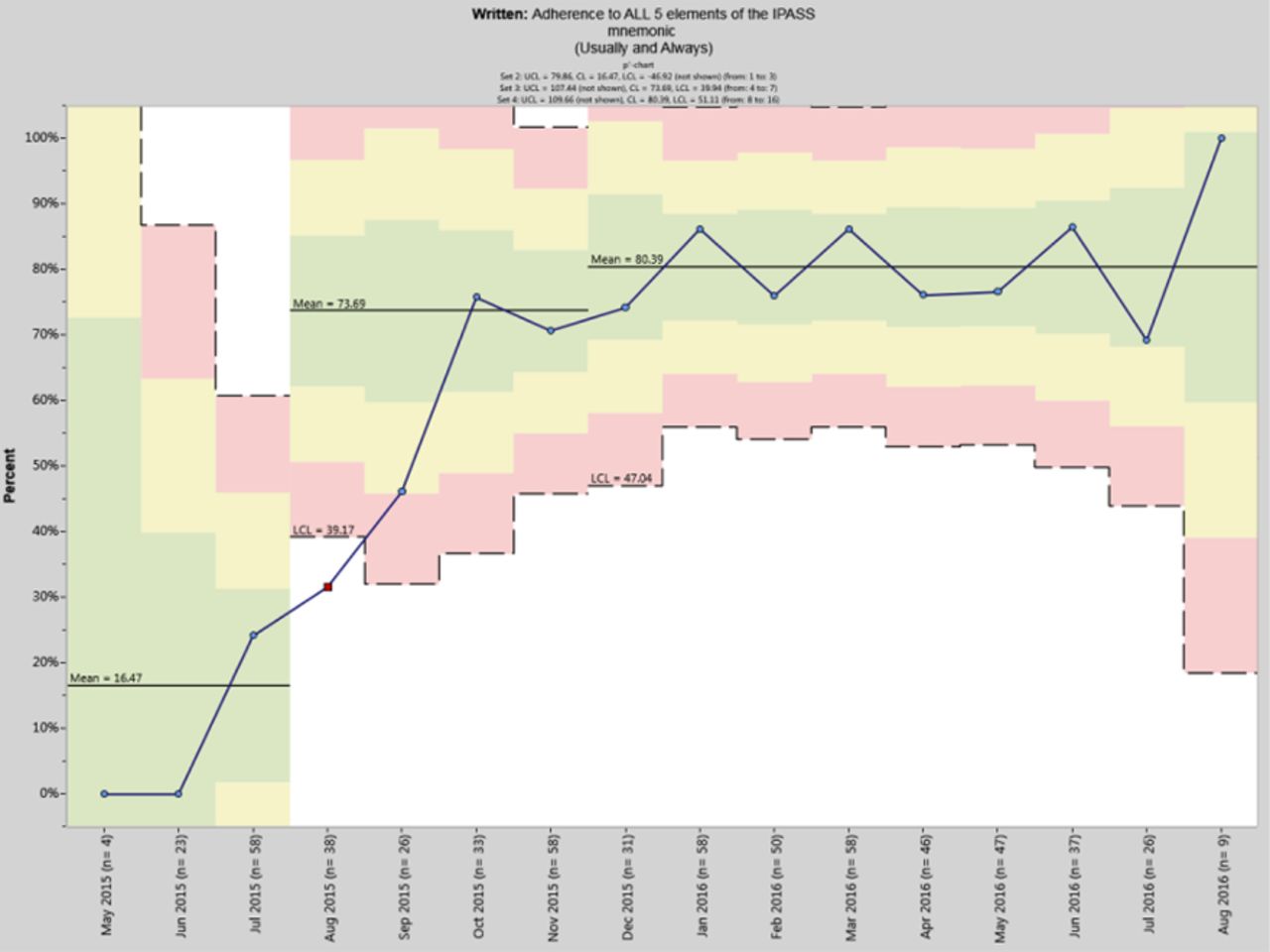
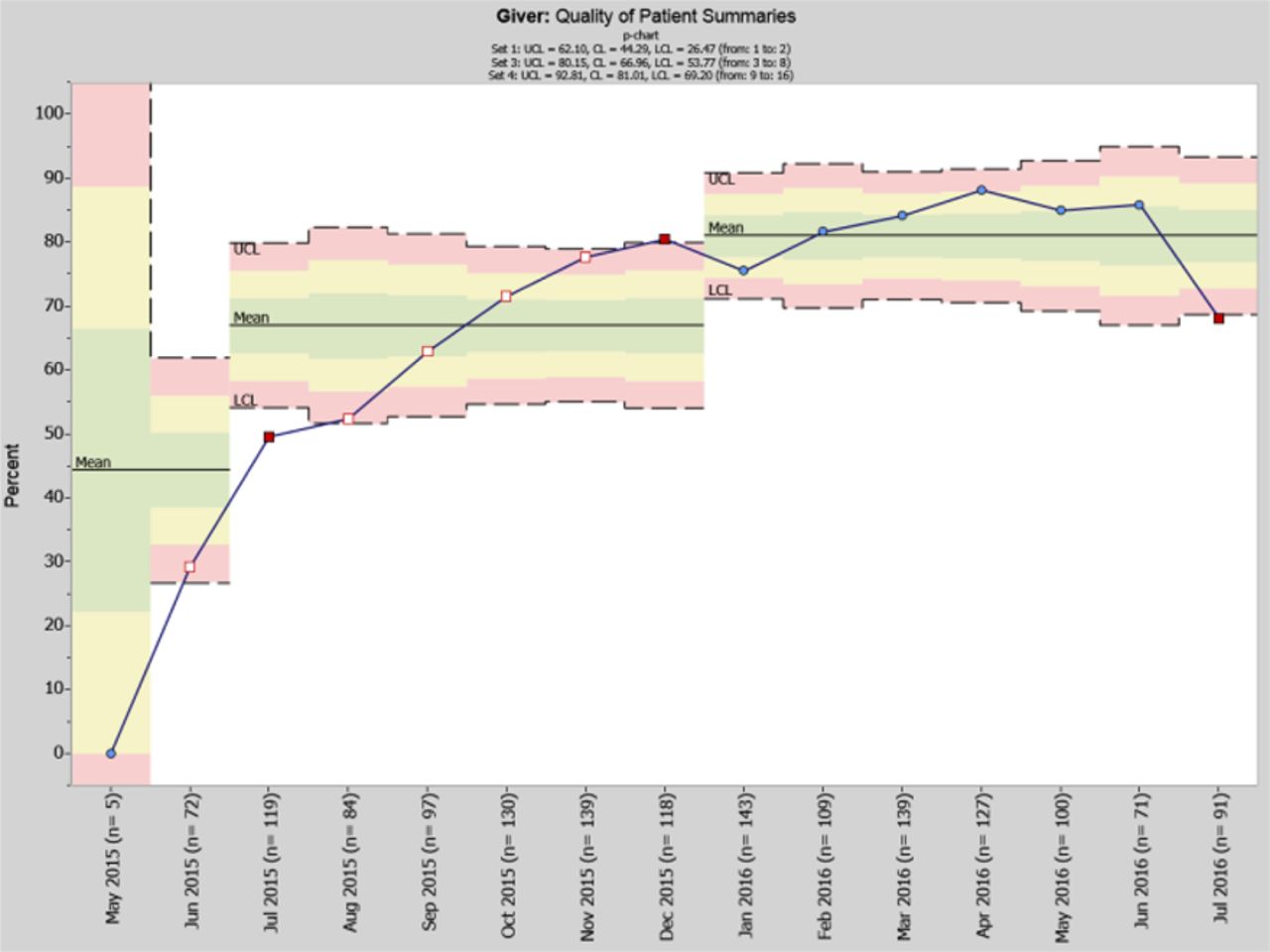
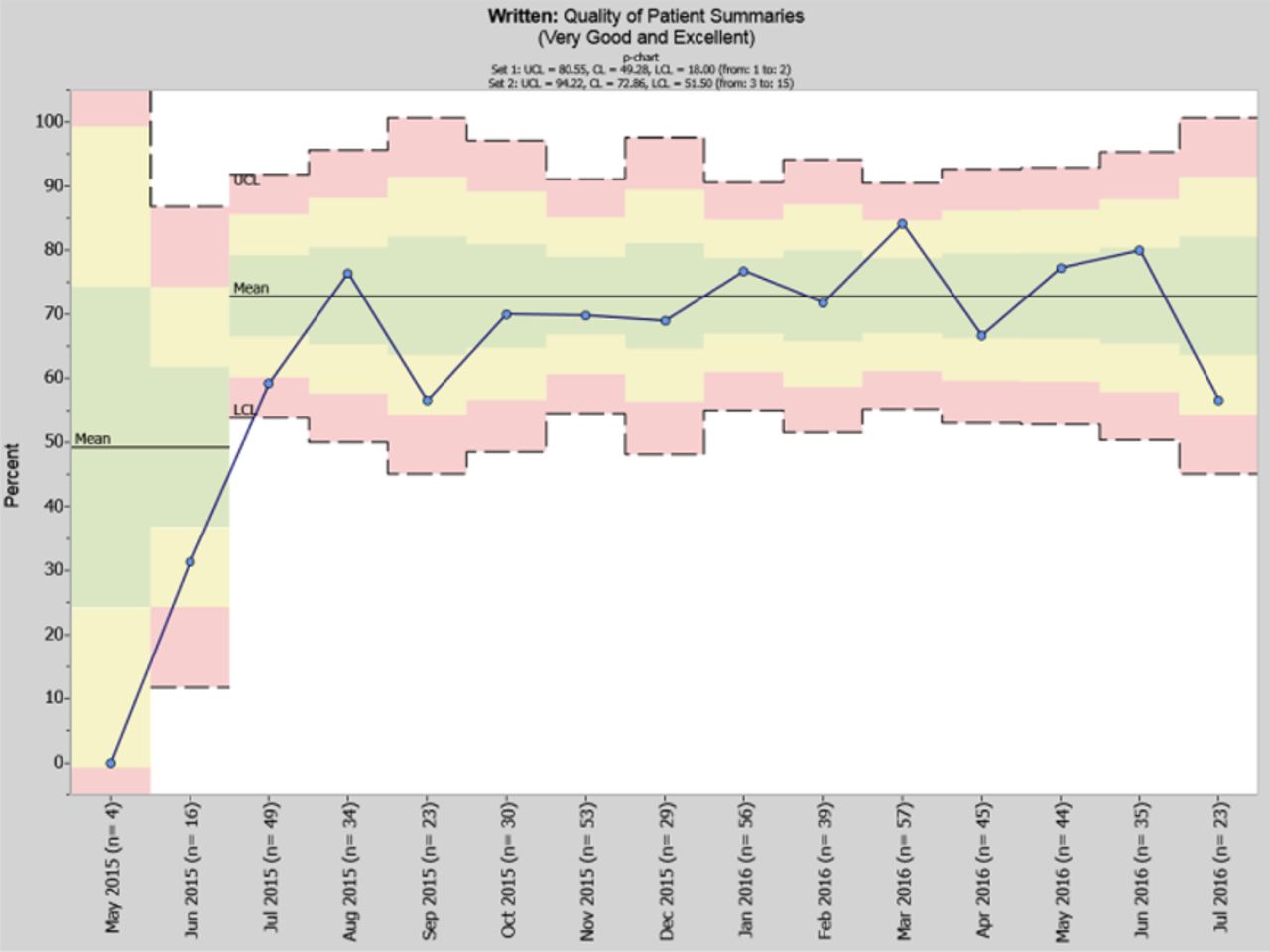
Results Implementation was associated with increased inclusion of all 5 I-PASS mnemonic elements for both verbal (14% vs 70%) and written (0% vs 81%) handoffs. Additionally, increases were noted in the frequency of high quality verbal (44% vs 81%) and written (49% vs 73%) patient summaries, verbal (22% vs 82%) and written (44% vs 72%) contingency plans, and verbal receiver syntheses (4% vs 81%). Adverse events decreased by 27%. All changes statistically significant. Improvements were similar across provider types and settings.
Conclusions The I-PASS Handoff program is associated with improved handoff communication in a variety of settings and provider types.⇓⇓⇓⇓⇓⇓⇓⇓

Verbal Handoff Assessments: adherence to all 5 mnemonic elements.

Written Handoff Assessments: adherence to all 5 mnemonic elements.

Verbal Handoff Assessments: quality of patient summaries.

Written Handoff Assessments: quality of patient summaries.

Verbal Handoff Assessments: quality of contigency plans.
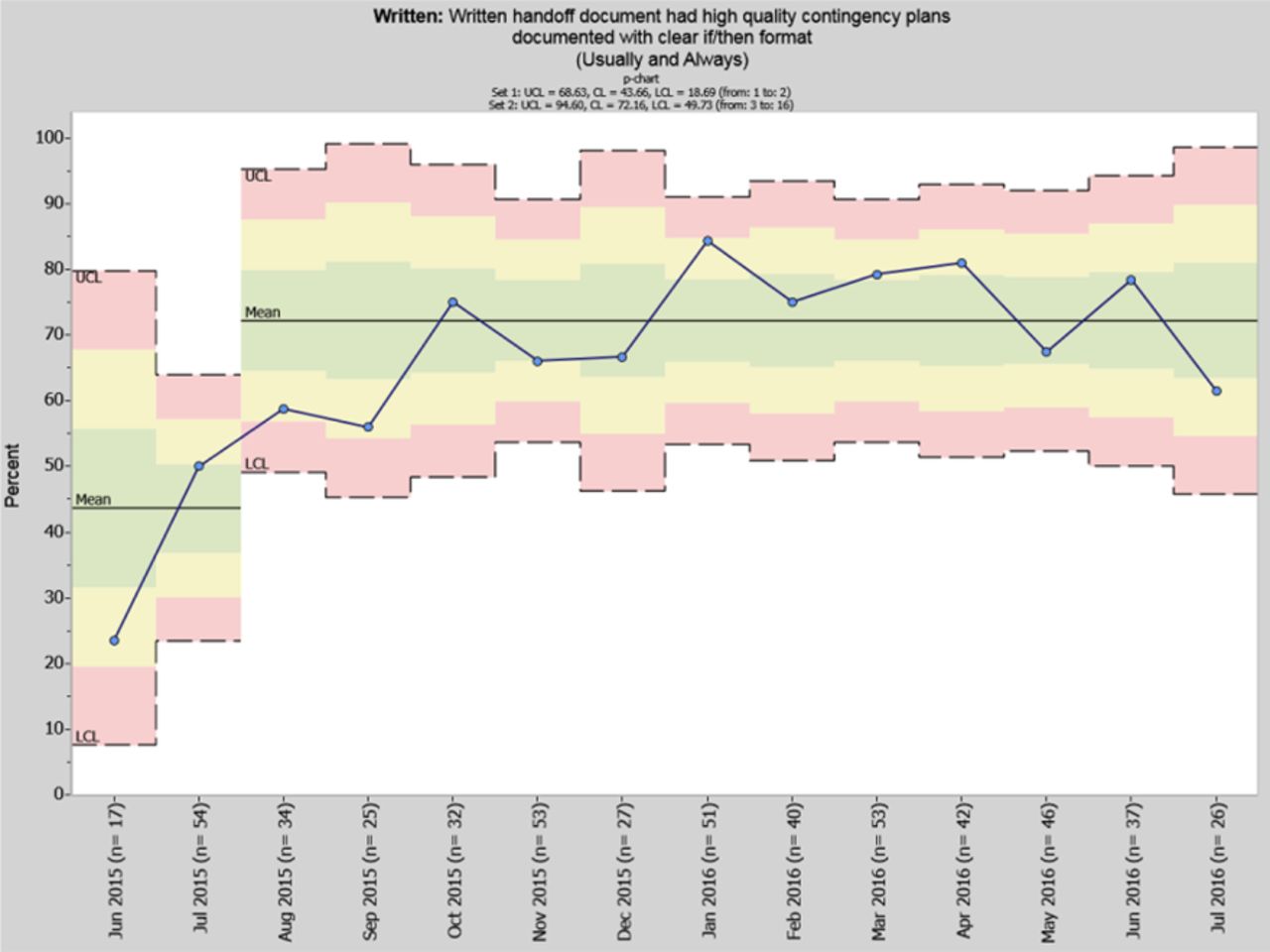
Written Handoff Assessments: quality of contigency plans.

Verbal Handoff Assessments: quality of synthesis by receiver.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
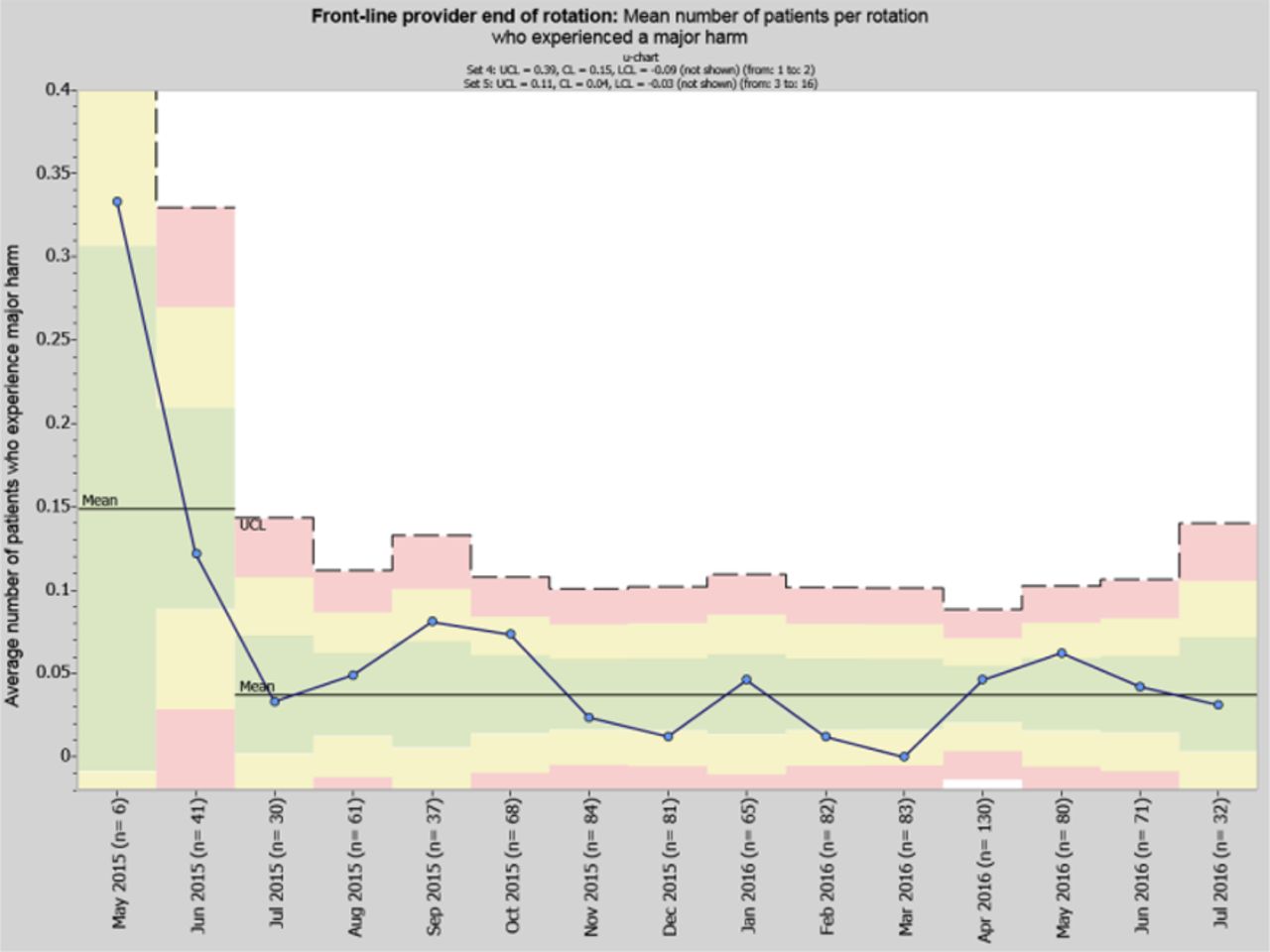
Provider-reported adverse event rate.
- Accreditation
- Anaesthesia
- Attitudes