Article Text

Abstract
Background ‘Organisational governance’—the systems, processes, behaviours and cultures by which an organisation leads and controls its functions to achieve its objectives—is seen as an important influence on patient safety. The features of ‘good’ governance remain to be established, partly because the relationship between governance and safety requires more investigation.
Aims To describe external governance systems—for example, national targets and regulatory bodies—and an NHS Trust's formal governance systems for Health Care Associated Infections (HCAIs) and medication errors; to consider the relationships between these systems.
Methods External governance systems and formal internal governance systems for both medication errors and HCAIs were analysed based on documentary analysis and interviews with relevant hospital staff.
Results Nationally, HCAIs appeared to be a higher priority than medication errors, reflected in national targets and the focus of regulatory bodies. Locally, HCAIs were found to be the focus of committees at all levels of the organisation and, unlike medication errors, a central component of the Trust's performance management system; medication errors were discussed in appropriate governance committees, but most governance of medication errors took place at divisional or ward level.
Discussion The data suggest a relationship between national and local prioritisation of the safety issues examined: national targets on HCAIs influence the behaviour of regulators and professional organisations; and these, in turn, have a significant impact on Trust activity. A contributory factor might be that HCAIs are more amenable to measurement than medication errors, meaning HCAIs lend themselves better to target-setting.
- Organisational governance
- governance
- patient safety
- healthcare associated infections
- medication errors
Statistics from Altmetric.com
Introduction
Organisational governance in healthcare has been described as ‘the process of steering the overall functioning and effective performance of a hospital's mission, setting its objectives, and supporting and monitoring their realisation at the operational level.’1 Many of the developments in healthcare governance reflect those occurring in private sector governance.2–4 In both settings, recommendations on governance have been driven by scandals that have threatened to reduce trust.4 ,5 However, in healthcare there is a stronger focus on the needs of the wider public,6–8 with issues of quality and safety increasingly central.3 ,6 ,7 ,9
Growing attention is paid to healthcare governance in UK policy and guidance,3 ,6 ,9–12 reflecting UK and international recommendations,13 ,14 detailing how strategy, control systems, leadership and staff and patient engagement may support improved quality and safety. Several academic commentators support this position, but suggest that these relationships require greater study.15–18
This paper aims to increase understanding of the relationship between healthcare governance (hereafter referred to as ‘governance’) and patient safety, by mapping the formal governance arrangements for two patient safety issues—healthcare associated infections (HCAIs) and medication errors—in an acute NHS Foundation Trust, and their equivalent external governance systems, such as policy and regulation.
Research investigating the relationship between organisational governance and patient safety
While much research on patient safety focuses on ‘micro’ level processes, for example, clinical aspects of safe care,16 investigations of high-profile safety and quality failures in the UK19 ,20 and internationally21 have highlighted the importance of governance to patient safety. Much of the literature on governance focuses on composition and effectiveness at board level. This work highlights the importance of such features as accountability, board culture, decision-making and information sharing, clarity of authority and responsibility, and ‘workable’ board size.22–27 While some research has explored governance in terms of factors such as lines of communication, quality assurance structures and professional cultures, our understanding of how these elements of governance interact to influence quality and safety is still developing.28–31 The relationship between complex and potentially contradictory external and internal governance systems, for example, in terms of ‘meta-regulation,’ where organisations' self-regulation processes are in turn externally regulated, also requires greater exploration.15
In terms of the specific patient safety issues investigated here—HCAIs and medication errors—there is a dearth of empirical studies on governance arrangements.
HCAIs, such as methicillin-resistant Staphylococcus aureus (MRSA) and Clostridium difficile (C diff), have had a high profile in healthcare systems for a number of years.32 In 2008, MRSA was mentioned as a contributory factor on 1230 death certificates and C. diff on 5931.33 There has been a concerted effort throughout the NHS to reduce cases of HCAIs (initially MRSA, then C diff) over the past 5 years. Reported cases have fallen significantly: between 2003/2004 and 2008/2009, reports of MRSA bacteraemia fell by 62%; and reported cases of C diff in people aged 65 or over fell by 35.5%.34
Several recent national initiatives have promoted a greater focus on governance arrangements to reduce HCAIs.32 Board to Ward (9: 4), for example, emphasises the need to create a ‘culture of infection control and prevention’ throughout NHS organisations. Reviews of the literature32 ,35 suggest that the empirical evidence for the influence of organisational factors on infection control is limited. These reviews indicate that the majority of infection control research addresses ‘micro’ factors, for example, hand washing techniques and the accessibility of alcohol rub. Several organisational factors are identified as supporting improved infection control behaviour, including effective audit and regular feedback to staff; positive leadership from ward level up; strong, well-supported middle management; and sufficient infection control information, training and support. The authors note weaknesses in the evidence base in terms of the small number of relevant studies and poor reporting of methods and analysis, and suggest that additional research is required.32 ,35
Medication errors can occur at many stages of treatment, including prescribing, dispensing, administration and monitoring of drugs.36 Estimates suggest 9% of hospital inpatients suffer severe harm from medication errors; and preventable harm to inpatients caused by medicines might cost the English NHS £411 million.13 ,36 ,37
As with HCAIs, recent policy documents state the importance of good governance of medication errors in ensuring patient safety;36 yet evidence supporting this relationship is sparse. Systematic reviews covering acute care, nursing and mental health38–41 suggest that most studies investigating organisational factors' influence on medication errors are weak, citing poor documentation and failure to operationalise variables clearly. Given the weak evidence base, the reviews cannot draw strong conclusions on the relationship between organisational factors and medication errors. Some research indicates that components of governance can influence safety: training, for example, can increase nurses' awareness of medication errors,42 and feedback can influence the degree to which personnel report medication errors.42–46 Much research echoes policy, urging healthcare organisations to achieve ‘culture change’47 following other industries, such as aviation.48–50 Overall, however, the evidence base for the influence of governance arrangements on medication errors remains limited.
In summary, while policy initiatives increasingly prioritise governance, there is little empirical evidence on the relationship between governance and patient safety or the aspects of governance that are most important to safety.
This paper presents the initial stages of a research programme that aims to address these gaps by:
analysing how NHS organisations govern two patient safety issues—HCAIs and medication errors; and
developing interventions based on this analysis to improve governance of these patient safety issues.
Here, we present the external governance systems and an NHS Foundation Trust's formal governance systems for HCAIs and medication errors. Based on these findings, we discuss the relationship between external and internal governance systems.
Method
Mapping tool
A ‘mapping tool’ to analyse governance of safety issues in terms of ‘contexts and contents’ was used. This tool (summarised in appendix A) was adapted from a comprehensive framework used for analysing risk regulation regimes.51 In assessing ‘contexts,’ the tool examines a range of factors that might influence governance of safety issues. It addresses the characteristics of the safety issue itself, how it is addressed in national policy, regulation, academic research and the media.51
Drawing on discussions with healthcare staff and a framework for empirical analysis of governance,31 the research team added sections to the tool to collect data on a wide range of organisational factors, including its history and recent developments, such as key events and significant improvement interventions. In assessing local governance, the tool examines formal structures and processes that make up a hospital's governance system (eg, standard setting, data collection and analysis, behaviour modification). The tool addresses the organisation's strategic direction, committee structure and assurance systems, informed by a governance self-assessment matrix produced by the Department of Health.3 In addition, the tool examines the people, groups and resources that support governance of the issue (eg, the roles and responsibilities of patients, nurses, doctors, management and the board); and other ‘informal’ governance factors, such as the relationships between professional cultures, local champions and the importance of the safety issue to local leadership.31 Finally, the research team added a section covering the organisation's ‘future developments and plans’—for example, long-term strategic direction and preparation for new national targets.
This article focuses on just two of the factors addressed by the tool: external governance systems and local formal governance arrangements. Future work will analyse other factors, such as resource use and ‘informal governance.’
Data collection
The study took place in an acute NHS Foundation Trust based in London, England. The data were collected during the period June–December 2008 and reflect the external and local formal governance systems at that time.
The mapping tool was populated based on documentary analysis and interviews with key personnel. Documents were drawn from:
the participating Trust (eg, annual reports, policies and committee minutes); and
national bodies (eg, DH, National Patient Safety Agency).
Participants
Twenty-one Trust personnel (10 for HCAIs and 11 for medication errors) were interviewed. Participants comprised clinicians, board members and representatives of the Trust's risk, governance, infection control, pharmacy and legal departments. Interviewees were selected purposively based on their knowledge of the safety issues studied and the Trust's organisational structures.
Interviews focused on completing the mapping tool. Data were recorded as field notes and transferred to an electronic version of the mapping tool. Data on external and local formal governance systems for HCAIs and medication errors were then analysed.
Diagrams illustrating the external governance systems and the Trust's formal governance arrangements for the selected safety issues were produced. These were shared with interviewees for validation during the data-collection phase.
Results
In this section, we compare governance of HCAIs and medication errors in terms of external and local formal governance systems.
External contexts
Figures 1, 2 show external influences on governance of HCAIs and medication errors respectively. Table 1 compares how key external actors (as identified by respondents) influence local formal governance.

External governance system for HCAI (June-December, 2008).

External governance system for medication errors (June-December, 2008).
Comparison of key influences on governance of Health Care Associated Infections (HCAIs) and medication errors
Figures 1, 2, and table 1, show some overlap in external influences on governance of medication errors and HCAIs, but also some significant differences. Principal among these was the approach taken by the DH to setting performance targets. There were time-limited targets to reduce MRSA and C diff, and while the DH stated an aim to reduce serious medication errors by 40%,11 ,54 this did not become a target assessed by regulators in the same way as targets set for MRSA (although not C diff). Both HCAIs and medication errors are ‘core standards’ within the Annual Health Check (carried out by the Healthcare Commission/Care Quality Commission).
There was a stronger focus on outcomes in HCAIs than in medication errors. Several bodies focused on MRSA and C diff counts and rates, while medication errors were measured based on incidents reported to the National Reporting and Learning System. While both medication errors and HCAIs were referred to in core Standards for Better Health, only the HCAI standard referred to improving outcomes.
In terms of behaviour modification, HCAI control was assessed on environment and governance systems, and there have been several national infection control campaigns in recent years. By comparison, less attention was paid to medication errors, providing guidance, but only limited assessment of systems and processes. A further key difference in the map of external influences was respondents' identification of the media as significant to governance of HCAIs, but not medication errors.
Internal governance arrangements
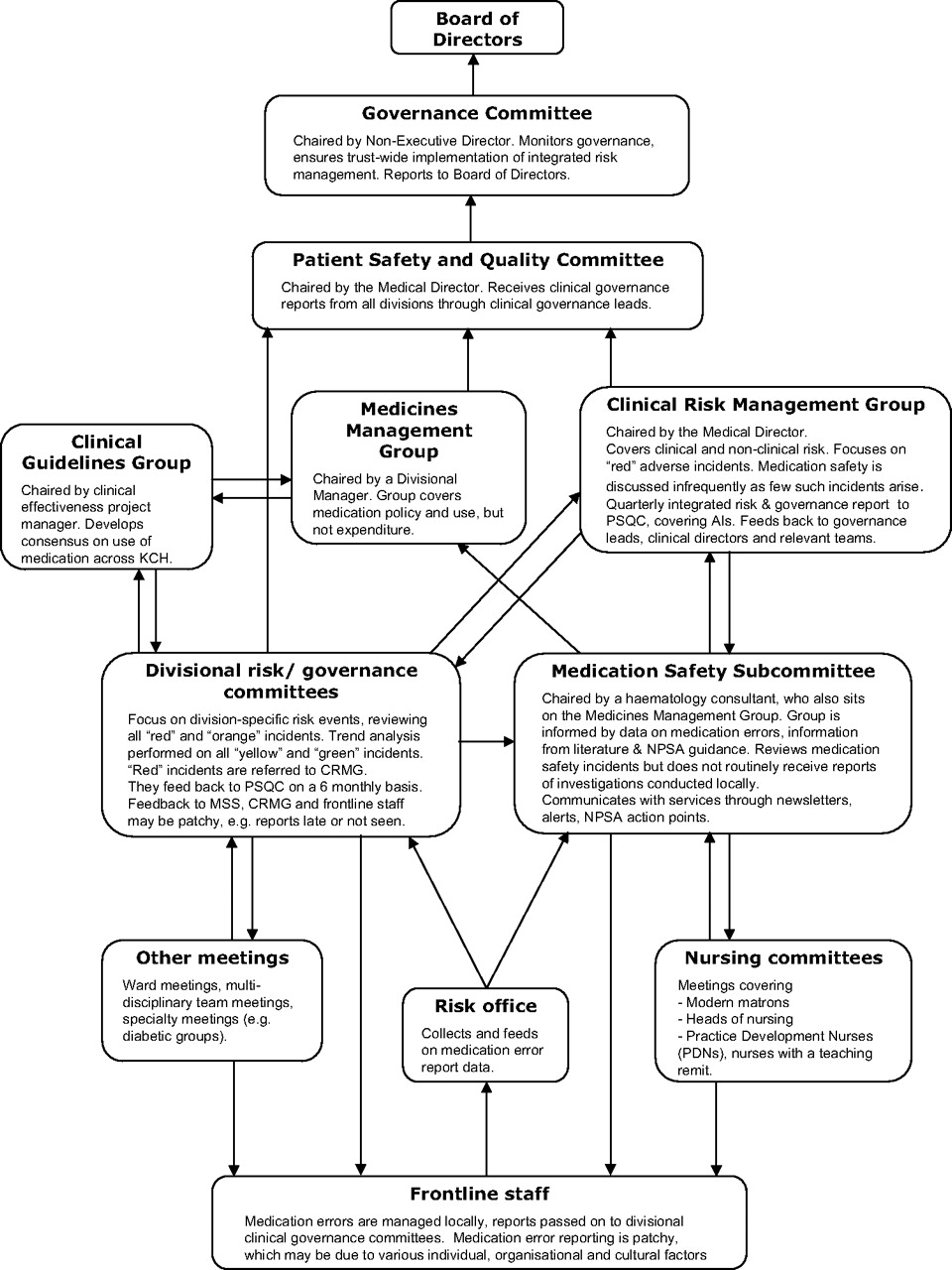
This section presents our findings on how the participating Trust governed HCAIs and medication errors, as detailed in figures 3, 4

Local formal governance system for HCAI (June-December, 2008).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Local formal governance system for medication errors (June-December, 2008).
Figure 3 suggests that local governance of HCAIs was heavily data-driven. Local management of HCAIs was supported by microbiology personnel and the infection control team. Infection data were fed back to frontline staff and into scorecards capturing the number and rate of infections; these scorecards fed into the organisation's performance management structure, which focused on ensuring Trust compliance with external targets and local Key Performance Indicators (KPI). This indicated that HCAIs were a key component of the organisation's strategy and a significant means by which it assessed the safety and quality of its services. Scorecard data offered a view of the organisation as a whole, but also allowed division and ward-specific analysis and feedback. Such a system ensures that Trust leadership can guide and support focused responses to variations in local performance, for example, through ward-specific audits and training initiatives.
Three high-level committees addressed HCAIs. Respondents' opinions on the effectiveness of this structure differed: some regarded duplication of messages and potential overlapping responsibilities among groups and committees as confusing and ineffective, suggesting it had led to mistakes in reporting; others suggested duplication of key messages is necessary to get staff ‘on board’ and sustain engagement and change in the long term.
Data on medication errors took the form of incident reports, the majority of which were recorded by Pharmacy personnel. These reports were fed to the risk office, which then distributed them to committees as shown in figure 4. Lines of communication existed, supporting communication of error data from the ward and divisional level up to board level. Progress reports (eg, on local policy and outcomes of external reviews) were presented to the Patient Safety and Quality Committee on a 6-monthly basis for information; the Clinical Risk Management Group covered ‘Red’ events (which occur rarely) and events requiring changes in behaviour; actions were fed back down the organisation via (identified) relevant governance leads and clinical directors. Respondents stated concerns that there was substantial under-reporting of medication errors and that some lines of communication might not operate reliably, thus limiting potential for learning within the organisation.15
The responsibility for governing medication errors was predominantly devolved to the divisional level. Respondents viewed this structure positively, feeling it supported direct, well-informed leadership; yet this would obstruct Trust leadership's awareness of how (and how well) this devolved governance operated. At the ward level, medication errors were addressed by various professions: key among these ‘local supports’ was pharmacists ‘green-penning’ drug charts—correcting errors and offering supplementary advice—acting as a ‘helping hand’ or ‘safety net.’ In contrast with governance of HCAIs, these local data were not used as a governance tool more widely within the organisation.
Discussion and conclusions
While governance at the organisational level may be an important influence on patient safety, there are few studies on how formal processes of governance relate to safety. Indeed, the nature of organisational governance itself remains to be described satisfactorily, with much previous research failing to look beyond board level. This paper compares the external and formal internal governance systems for HCAIs and medication errors, and suggests a relationship between the two, with the external context influencing internal arrangements. The ‘stronger,’ more numerous external influences on HCAIs were reflected in the Trust's respective formal governance systems for HCAIs and medication errors. However, we cannot say whether ‘stronger’ external governance resulted in more ‘effective’ local governance. Further research, examining governance of other patient safety issues internationally recognised as important matters to be addressed through governance—such as patient falls, pressure ulcers and appropriate use of clinical blood products15—may support a clearer understanding of this relationship.
The differences we report might derive from HCAIs lending themselves more readily to measurement and benchmarking, and thus more amenable to ‘meta-regulation.’15 Such tasks as target setting and intervention design are more straightforward when a measure and its meaning are agreed upon.56 ,57 Whereas medication error data are based on incident reports and thus dependent on individual interpretation (and generally suffer from substantial under-reporting15), HCAI data are based on less ambiguous measures such as MRSA and C diff rates. One attempt to make medication errors more amenable to measurement is reviewing cases in which ‘trigger drugs’ have been prescribed.58 The Patient Safety First initiative features this as a key intervention (see table 1); evaluation of its impact on safety might establish the benefits of this approach.
Board members' understanding of patient safety and quality issues (eg, risk factors and how best to interpret related data)17 ,18 and the style of leadership they provide29 ,30 may be important influences on safety and quality provided at the front line. While we interviewed director-level personnel, the fact that we did not analyse the organisation's Board as a whole may be considered a limitation to this paper, but it is one that future research will aim to address.
In addition to formal governance arrangements, informal local governance systems—such as professional cultures, local champions and individuals' willingness to accept accountability (summarised in appendix A)—are likely to play a significant role in patient safety. The work reported here forms part of a research programme that will investigate this broader picture, with the aim of improving our understanding of how these factors relate to one another and to patient safety.
Acknowledgments
We extend our thanks to all Trust personnel who participated in this research. We also thank other members of King's PSSQ for their contributions to the work and the paper. In particular, we thank J Chamberlain for her contribution to the development of the mapping tool. We are also grateful to A Dodds, J Higginson, C Humphrey, N Kodate, J Sandall, J Filochowski and two anonymous referees, who commented on earlier drafts. This article presents independent research commissioned by the National Institute for Health Research (NIHR). The views expressed in this publication are those of the author(s) and not necessarily those of the NHS, NIHR or the Department of Health. Any errors or omissions are ours.
Appendix A Summary of ‘mapping tool’
| Contextual factor | Defining characteristics | Internal—the trust | External—policy, literature |
| 1. History of regime/recent developments | How have issues developed/changed in last 2–5 years? | ||
| 2. Type of risk (inherent features of the risk) | Source; how well-established; how easily quantified; probability of occurrence; severity of consequences | ||
| 3. Public preferences and attitudes | Media reporting/cover; public attitudes; political agenda | ||
| 4. Relevant groups | Regulatory bodies; unions; pressure groups; partner organisations (eg, primary care trusts, local authorities, voluntary sector) | ||
| 5. Stakeholders | Professions (eg, doctors, nurses, pharmacists), managerial hierarchy (eg, board, middle management, front line staff), service users and carers |
Summary of Contexts matrix
| Governance activities | ||||
| Standard setting and information dissemination | Information gathering and analysis | Behaviour modification (strategies and activities) | Future developments and plans | |
| Policy reach (eg, acceptable levels of non-compliance, spread of governance activities) | ||||
| Physical investments and resources (eg, money and time spent on governance activities) | ||||
| People/accountability (eg, personnel accountable for governance activities) | ||||
| Information/groups (eg, number and type of committees involved in governance activities) | ||||
| Rule orientation (eg, how mandatory is engagement in governance activities?) | ||||
| Culture and leadership (eg, attitudes of leadership and professional cultures to governance activities) | ||||
Summary of Contents matrix
References
Footnotes
Funding National Institute for Health Research (http://www.nihr.ac.uk).
Competing interests None.
Ethics approval Ethics approval was provided by King's College London Education and Management Research Ethics Panel (Health Care Associated Infections—ref REM(EM)0708-84; medication errors—ref REPSSPP(W)-0708-207, June 2008).
Provenance and peer review Not commissioned; externally peer reviewed.