Article Text

Abstract
Introduction Multiple resident-related factors contribute to ‘missed opportunities’ in providing comprehensive preventive care for female patients, including comfort level, knowledge and experience—all of which are compounded by resident turnover rates. Of particular concern among Internal Medicine (IM) residents is their knowledge and comfort level in performing pelvic exams.
Aim To evaluate the impact of a quality improvement project of implementing a Women's Preventive Health Clinic (WPHC) on addressing gaps identified by needs assessments: residents' comfort and knowledge with female preventive care and cervical cancer screening.
Programme description The WPHC, a multidisciplinary weekly clinic, focused on preventive services for women with chronic conditions. The alternating didactic and clinic sessions emphasised women's preventive health topics for IM residents.
Programme evaluation Sixty-three IM residents participated in WPHC between 2002 and 2005. Pre- and post-test design was used to assess resident knowledge and comfort levels. Cervical cancer screening rates of residents' patients were assessed pre- and post-WPHC initiation. There was a significant improvement in general knowledge (64% correct at pretest vs 73% at post-test, p=0.0002), resident comfort level in discussing women's health topics and performing gynaecological exams (p<0.0002). Cervical cancer screening rates among IM residents' patients improved from 54% (pre-WPHC initiation) to 65% (post-WPHC initiation period).
Discussion The results indicate that a focused resident preventive programme can meet gaps identified by education and needs assessments, and simultaneously have a positive impact on cervical cancer screening rates and thus may serve as a model for other residency programmes.
- Continuous quality improvement
- women's health
- graduate medical education
- preventive health services
- chronic disease
- primary care
- PDSA
Statistics from Altmetric.com
- Continuous quality improvement
- women's health
- graduate medical education
- preventive health services
- chronic disease
- primary care
- PDSA
Introduction
Background
Women's health education has become an integral part of curriculums for residency programmes1 to address the reality that internists need to provide preventive health services to women2 ,3 and to meet Accreditation Council of Graduate Medical Education's gender-specific care requirement for a residency programme. However, there is no standard curriculum for training in women's health,4 and an unfortunate gap remains: women receive fewer preventive services than recommended,5 ,6 despite the effectiveness of Pap smear screening: early detection of cervical cancer with Pap smear testing has decreased disease mortality by 75%.7
Adequate opportunities to develop competency and comfort in performing pelvic exams and cervical cancer screening are needed for internal medicine trainees to help close this gap. Yet, one survey of general internists revealed that 48% reported little residency training in common women's health issues including safe sex counselling, cancer screening, training in Pap smear and pelvic exam technique, and osteoporosis.3
To date, examination of the barriers to screening8–10 has focused on patient characteristics associated with a lower screening rate (eg, lower socio-economic status, obesity, lack of health insurance, increased age and chronic medical conditions),11–16 rather than on organisational barriers (eg, time constraints, competing demands, lack of ‘reminders’ and lack of incentives for delivering preventive care), including training-related issues. Given the limited attention to training-related issues, we focused on residency teaching opportunities, recognising that adequate training can help address some systematic barriers. Busy residency training programmes with a rapid turnover rate may lead to ‘missed opportunities’ for providing essential screening services,4 particularly when coupled with an environment where there are many competing demands for limited patient visit time. Trainees in such programmes may devote the entire visit to understanding the patient's overwhelming disease burden, leaving little time to discuss health maintenance procedures even with reminders. In addition, if the comfort level is low for certain topic areas, such as pelvic exams, less interest may prevail for developing comfort and confidence for those areas.
Local problem addressed
Education training needs assessment
Insufficient local residency training related to common women's health issues was confirmed by a sample of Internal Medicine (IM) residents (n=70) who completed a brief training needs assessment survey of women's health topics. Of the 54 residents (77%) responding, the three most frequently listed topic areas requiring increased emphasis in the training programme were: Pap and pelvic techniques (46 residents or 85%), osteoporosis (29 or 53%), sexually transmitted diseases (28 residents or 47%).
Female clinical screening needs assessment
A concurrent review of our entire resident clinic revealed that only 43% of 4583 eligible women (all female patients aged 18–65 without a hysterectomy seen over the prior 3 years) had a Pap smear documented in Epic electronic medical records system.
Intended improvement
To address these education and quality deficiencies, a multidisciplinary Women's Preventive Health Clinic (WPHC) was developed in collaboration with the Obstetrics and Gynaecology faculty at our institution. The goal was to improve the provision of preventive services for women with chronic medical conditions and provide more comprehensive preventive health education to Internal Medicine (IM) residents. Ideally, we would have addressed a wider-range of obstacles to tackle persistent low screening rates for women, but we recognised the importance of a manageable focus. Accordingly, at the outset we decided to focus on education deficiencies first. Specifically, the WPHC rotation was designed to improve internal medicine residents' knowledge of female preventive services and increase the opportunity to develop comfort in discussing issues and performing procedures related to breast cancer screening, osteoporosis, depression/domestic violence, colon cancer and cervical cancer screening.
Although, ultimately, the goal was to document improvement in all areas of female preventive health services, for the first cycle of change we chose to focus on cervical cancer screening rates for three reasons. First, of the preventive health services, cervical cancer screening is established in the literature to reduce morbidity and mortality associated with the disease by 75%.6 ,7 Second, our needs assessment revealed this was an improvement area as evidenced by gaps both in the clinical care provided and the educational needs of the internal medicine residents. Third, from a documentation stand-point, obtaining data regarding cervical cancer screening rates is more reliable and relies very little on self report (it was retrieved through a billing procedure code) versus doing iterative chart reviews to establish documentation of other screening such as breast exams or osteoporosis screening discussions.
Setting
MetroHealth Medical Center (MHMC) is a 700-bed urban teaching hospital in Cleveland, Ohio, affiliated with the Case Western Reserve University School of Medicine. The primary care population consists mainly of patients from urban Cleveland with about 24% patients on Medicaid, 5% on Medicare and about 50% on self pay (table 1). The demographics highlight the fact that most patients seen in this clinic are under- or uninsured, thereby increasing likelihood of discontinuity of care.
Demographics of study patient population
The IM residency programme has 100 residents total, and each has a weekly half-day ambulatory continuity clinic site and must complete a 1-month ambulatory block yearly. As part of their ambulatory rotation, it was expected that second- and third-year residents would rotate through the WPHC. Prior to our WHPC curriculum, educational topics on women's health (eg, oral contraception, osteoporosis, breast cancer/cervical cancer screening) were delivered via five to six didactic sessions at a general noon conference, there was no formal training sessions for pelvic or breast exam techniques, and emphasis was largely faculty preceptor-dependent.
Programme description
WPHC met weekly for four hours in the morning, alternating between didactic and clinical sessions and was incorporated into an established Medical Care clinic through which second- and third-year IM residents were expected to rotate for 4 weeks each academic year.
Two internists and one gynaecologist faculty member of the Case Western Reserve School of Medicine presented the didactic sessions (table 2) and staffed the WPHC. Alternating Monday mornings, patients were scheduled in the WPHC clinic. Typically, each session had 12–16 women scheduled. Patients were primarily referred from the resident continuity clinics, and a small number of patients were referred from faculty clinics within the Department of IM. A standard handout describing the Clinic was given to the patient upon initial referral from her primary care physician. Additionally, she spoke to a registered nurse prior to leaving her primary care appointment regarding the importance of the WPHC referral and reason. While in the WPHC, she was initially seen by one of the residents. A standard template was used when obtaining a history and performing a physical exam (figure 1) with a focus on discussion and screening of: osteoporosis, colon cancer, cardiovascular risk assessment, breast cancer, cervical cancer and screening for depression and domestic violence. The resident, while supervised by an attending physician, performed breast and pelvic exams along with Pap testing. The residents followed up on all blood work and pathology obtained during clinic and contacted the primary care physician. If needed, patients were asked to return for a second visit to discuss abnormal results.
Curriculum topics and activities

Women's preventive health clinic standard patient care template.
Programme evaluation
Resident knowledge and comfort level
To assess changes in knowledge of preventive guidelines, we used a test with 23 multiple-choice and true/false questions covering core topics discussed during the WPHC didactic sessions. A total knowledge score was calculated, and differences in the pre- and post-WPHC knowledge levels were evaluated using the t test.
Changes in comfort in performing women's health topics and procedures were assessed using 10 items on a scale of 0 (not at all comfortable) to 3 (extremely comfortable). Relevant items assessed the performance of pelvic exams, interpretation of Pap smears, obtaining/interpreting vaginal cultures, discussion of osteoporosis screening, performance of breast exams and cardiovascular risk assessment. We analysed these items separately to obtain specific information about where the curriculum was successful and where future curricular emphasis needed to be added given the importance of increasing comfort with these specific clinical exams and screening procedures. Differences in the pre- and post-WPHC comfort levels were evaluated using the Wilcoxon rank sum test.
Feedback about the clinic was obtained from residents after completing their WHPC modules via two open-ended items: ‘What was the most important thing you gained from these sessions?’ and ‘What suggestions do you have to improve this clinic?’ Responses were used to identify themes.
Clinical measure
The primary patient care outcome was ordering Pap tests for cervical cancer screening. We measured the rate of Pap test orders for women aged 18–63 years during two consecutive 2.5-year periods before and after establishment of the WHPC. For the pre-WPHC measure, we identified a cohort of women with a first visit (ie, no visit in the prior 3 years) to the IM resident clinic between 1 June 2000 and 31 December 2001. We searched the electronic medical record for any Pap order between the first visit and 31 December 2002. To measure the rate of Pap ordering post-WPHC, we identified a similar cohort of women with a first visit between 1 January 2003 and 30 June 2004 and searched for the first Pap order between the first visit and 30 June 2005. Women with documentation in the electronic medical record of prior hysterectomy and those with only one visit during the observation period were excluded from the analysis. We analysed the time until first Pap order for women in both cohorts using the Kaplan–Meier method and Cox proportional hazards regression method with time to first Pap order as the dependent variable adjusting for the total number of clinic visits per patient, age and race. All analyses were performed using SAS software (V.9.1.3, SAS Institute, Cary, North Carolina, 2005).
Results
Participants
Not all second- and third-year residents participated due to scheduling challenges (eg, post-call schedule conflicts, covering inpatient services and vacation schedules). Specifically, from July 2002 to July 2005, 63 residents rotated through the WPHC. Of those 63 residents, 54 were available for the baseline and/or pretest, and 40 of the 54 completed the post-test. Clinical outcomes information was available for all residents.
During the same time period, a total of 702 patients were referred to the WPHC with 378 patients (54%) completing their visits. Of those completing their visits, 204 (54%) were referred from the resident clinic. The average age of women referred from resident clinic was 48 years, 48% white, 33% African–American and more than half uninsured (table 1).
Resident knowledge and comfort level
The average pretest score (n=53 of the 63) was 64% correct, and the average post-test score (n=40 of the 53) was 73% (p=0.0002).
Fifty-four residents completed the baseline evaluation for level of comfort items, and 39 completed the post-clinic evaluation: the level of comfort increased in all areas after participation in the WPHC (table 3).
Comparison of pre- and post-Women's Preventive Health Clinic (WPHC) evaluation scores
Overall feedback from the residents was positive (table 4). One common suggestion was to focus more on contraceptive therapy for women.
Compilation of themes related to resident feedback on post-clinic evaluations
Clinical outcome
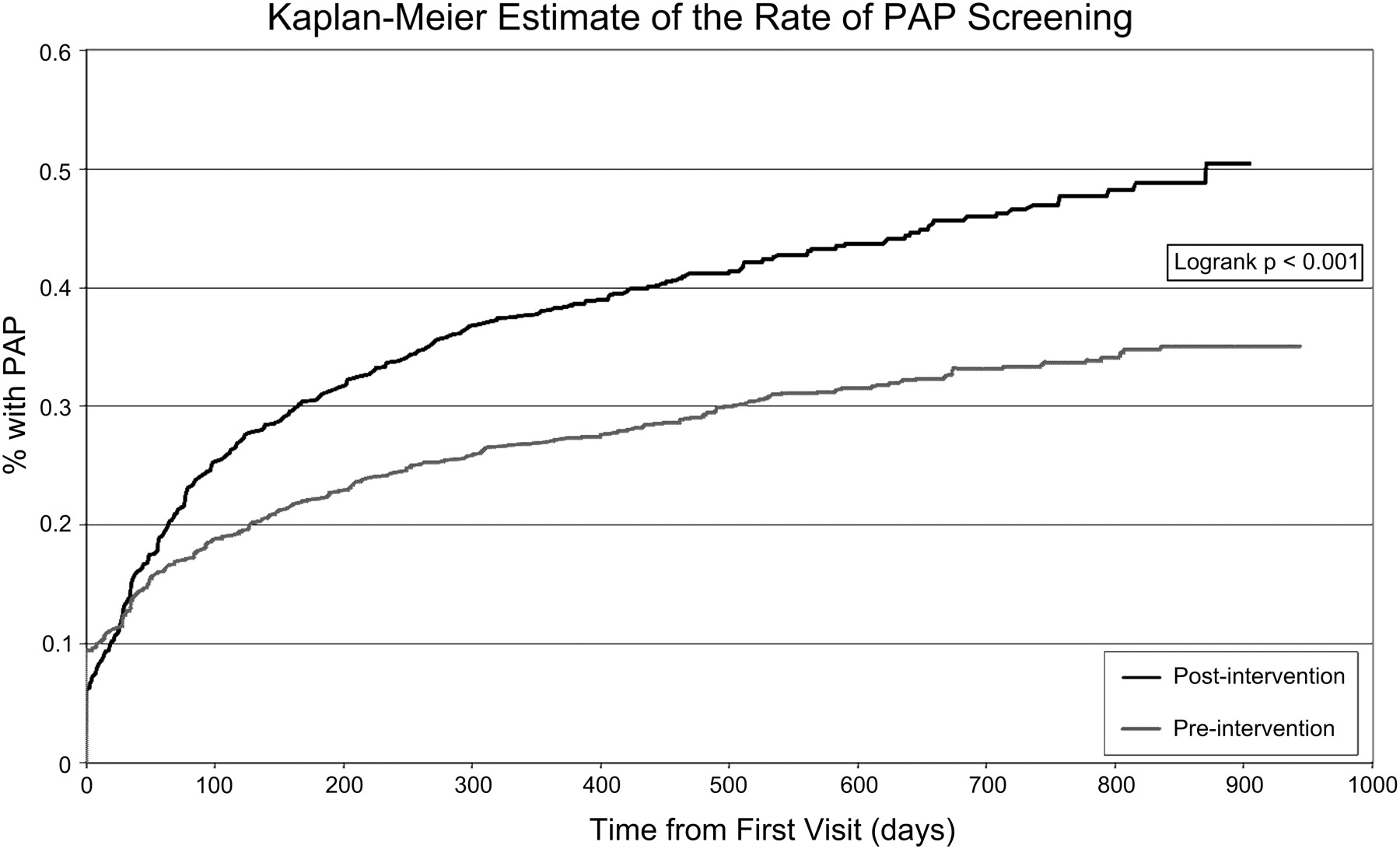
Cervical screening ordering rates among IM resident patients increased significantly following initiation of the WPHC. For women in the pre-WPHC cohort (prior to initiation of the clinic), during the 2.5 years after the WPHC started, the cumulative incidence of Pap orders was 54%. For the post-WPHC clinic cohort, the cumulative incidence was 65%, p=0.004 (figure 2). After adjusting for age, race and total number of visits, women in the post-WPHC period were 35% more likely to receive an order for Pap testing (HR=1.35, 95% CI 1.18 to 1.53, p<0.001).
{kind=link}
{kind=link}
Kaplan–Meier estimate of the rate of Pap screening. WPHC, Women's Preventive Health Clinic.
Discussion
Women seen in our clinic after the initiation of the WPHC were 35% more likely to have Pap smears ordered. Since the total number of women seen in WPHC itself was relatively small, the increase in Pap ordering for the entire clinic population suggests that the WPHC may influence how residents practice in their own continuity clinic. Most residents felt the WPHC was educational, and expressed the belief that such training should be mandatory.
Due to scheduling conflicts and coverage issues, not all second- and third-year residents completed the consecutive 4-week curriculum. Reasons for not attending or participating in all sessions were not individual resident-based factors but organisational level factors (ie, post-call schedules, getting pulled to cover inpatient services and vacation schedules). While this does not eliminate the concern about differences between responders and non-responders, it does lessen the impact. Additionally, we may have stumbled upon another organisational barrier contributing to inadequate preventive care training in resident clinics: we met challenges with residents completing an entire 4-week session since ambulatory training time took a back seat to covering inpatient services. This underscores how training environments may be sending inadvertent messages when it comes to the importance of preventive care.
A multidisciplinary clinic with faculty from two departments, while desirable to help ensure long-term sustainability, can be resource-intensive. One adjustment for the future is to address the need for all faculty members to be present at a given time, including determining the best mix for training. It is important to determine the best methods to sustaining specialty clinics, particularly if they hinge on one particular individual or champion. Support and resources from the organisational level and training programme level are more likely if the clinic can demonstrate improvement in education and resident comfort levels while improving key screening services for patients.
Another challenging aspect was the limited show rate of patients referred to our clinic. The poor show rate is probably due to many factors (eg, lack of understanding of the clinic's purpose and importance of screening, transportation, insurance coverage, lack of regular sources of care, patient populations with chronic disease burden demands which limited time to address preventive care issues, etc). While we cannot directly compare those who showed versus no-shows, the demographics (table 1) suggest that no major biases were present.
Other limitations include limited generalisability, since only one site and programme were studied. In addition, our use of before and after cohorts to measure the change in Pap test ordering cannot discern changes due to temporal trends.
Despite the limitations, our quality improvement intervention (WPHC), while only a first step, improved resident comfort level in performing cervical cancer screening as measured by feedback and increased the likelihood of residents performing Pap smears regardless of setting. As a first step, we chose to focus on cervical cancer screening rates. Demonstrating improvement of other measures, such as breast cancer screening, colon cancer screening discussions or osteoporosis discussions would be a logical next step. Within cervical cancer screening, the next steps for continued improvement would be to understand ways to better integrate the curriculum into the programme so all residents would complete it, and examine no-show reasons for WPHC patients. If one were to apply the framework that preventive care barriers fall into three categories, ‘awareness, agreement and ability’,17 ,18 then the ultimate goal is to improve ‘awareness, agreement and ability’18 of patients, physicians and organisations regarding the importance of cervical cancer screening, eventually making this an intrinsic part of the residents' continuity clinic experience.
Acknowledgments
The authors would like to gratefully acknowledge S Goldsberry, Department of Internal Medicine, and J Rohl, Department of Obstetrics and Gynaecology, for their vision in establishing the Women's Preventive Health Clinic.
References
Footnotes
Funding VA HSRD (Renee Lawrence's Salary Support).
Competing interests None.
Ethics approval Ethics approval was provided by the MetroHealth Medical Center IRB.
Provenance and peer review Not commissioned; externally peer reviewed.