Article Text

Abstract
Objectives To develop, implement and evaluate a training programme for senior doctors to become faculty leaders for patient safety training.
Methods Senior doctors were recruited from across 20 hospitals in the North Western Deanery, England, UK. The intervention comprised a half-day course in patient safety theory, root cause analysis and small-group facilitation, following which participants were invited to sign up as faculty for a region-wide patient safety training programme for trainees ‘Lessons Learnt’. Course evaluation comprised a prospective longitudinal study conducted in 2010–2012. Patient safety knowledge, attitudes and skills were evaluated pre and post course and retention further evaluated 8 months post course.
Results 216 senior doctors volunteered as faculty of whom 122 were appointed. Participants reported high levels of satisfaction with the course. Objective scores of patient safety knowledge significantly improved immediately post course (MedianPre course=70%, MedianPost course=80%, p<0.001) and were sustained at 8 months (Median8 month post course=90%). Similarly, measures of attitudes and self-reported safety skills also significantly improved post course and were sustained. Upon completion of the course, 88/122 (72%) participants facilitated 213 ‘Lessons Learnt’ sessions from January 2011 to July 2012 (mean 2, range 1–8 sessions per faculty member). Trainee satisfaction with faculty was high.
Conclusions There is considerable appetite for senior doctors to engage with training in patient safety as teachers and learners. Training senior doctors in patient safety is feasible, acceptable and effective as a means of building capacity and capability for delivering training in this rapidly emerging field.
- Continuing Education, Continuing Professional Development
- Patient Safety
- Safety Culture
Statistics from Altmetric.com
Introduction
Patient safety has gained international importance as a core tenet of high-quality healthcare.1 ,2 Recent years have seen an evolution away from a ‘blame culture’ to an ‘open and learning’ safety culture with a concurrent paradigm shift in error theory from the individual ‘person’ model to the ‘systems-based’ approach.3 ,4 However, there is growing concern that the pendulum may have swung too far and attention is now focusing again on the role and responsibility of the individual clinician in improving quality and safety.5–7
In line with this, recent high-profile reports have called for patient safety to be integrated into the curricula of all healthcare workers. These reports argue that sustainable improvements in patient safety will be difficult to achieve without medical education reform at the undergraduate and postgraduate level.8–10 As a result, there has been a proliferation of published curricula and interventions in patient safety education and training.11 However, there is a paucity of literature involving senior clinicians as the target population.12 ,13 This is a crucial omission: patient safety is a relatively new science and many senior clinicians will not have been exposed to it.6 ,14 Furthermore, despite the growing evidence for quality and safety education and training, the translation and wider adoption of such interventions has been slow. Various factors have been implicated of which lack of an ‘expert faculty’ is key.11 ,15–17
Senior doctors represent an untapped resource in terms of forming this ‘expert faculty’ to drive and support the delivery of educational interventions in patient safety, for a number of reasons. Senior doctors have credibility in relation to their juniors: in contrast to external safety ‘experts’ or ‘trainers’, they are not perceived as ‘outsiders’ to clinical practice.13 The role of senior doctors in workplace learning goes beyond feedback and supervision: they contribute to the ‘hidden curriculum’18 and have a powerful effect (positive and negative) through role modelling in terms of enculturation of professional qualities and safety-related behaviours such as hand hygiene.19 ,20 Moreover, there is the practical consideration of their availability: there are many more senior doctors than patient safety experts to deliver training. At times of financial austerity their costs may also be lower (compared with those of external ‘trainers’) as they can deliver teaching and training as part of their educational responsibilities to the hospital and their juniors. Finally, senior doctors are in a position of relative influence and power: they are well placed to help their juniors navigate the healthcare system and secure essential resources to support focused safety improvement efforts.21 ,22
This study reports the development, implementation and evaluation of a training intervention to develop senior clinical faculty for a regional patient safety training programme in the UK.
Methods
Setting: the ‘Lessons Learnt’ programme for UK trainees
In 2010–2012, we developed, implemented and evaluated a regional training programme in patient safety ‘Lessons Learnt: Building a Safer Foundation’ for all Foundation trainees (trainees in their first 2 years of clinical practice, n=500+ per cohort) in the North Western Deanery of England.23 ‘Lessons Learnt’ promotes shared peer-group learning from patient safety incidents that the foundation trainees are involved in or aware of within their own clinical areas. The learning occurs within a safe, facilitated forum that comprises a dedicated 60 min monthly session embedded within the existing teaching programme. The session is facilitated by a senior doctor (consultant or specialty registrar) and involves a peer-group analysis and discussion of a safety incident or error encountered by the trainee in the workplace using a validated incident analysis protocol.24
The role of the ‘Lessons Learnt’ faculty includes the following:
-
Attend a half-day training course in patient safety theory and incident analysis.
-
Facilitate one ‘Lessons Learnt’ session per month between January and July 2011 for trainees at their hospital (January–July 2012 for second faculty cohort).
-
Facilitate a ‘year-end’ evaluation of the ‘Lessons Learnt’ programme as implemented locally (ie, within their own hospital) at the end of the academic year (July 2011/2012).
Participants
Senior doctors from across all 20 hospitals in the North Western Deanery (England) were invited to participate in this study by means of a recruitment flyer disseminated via trainee teaching administrators (see supplementary web appendix 1). The following inclusion criteria were used to recruit faculty:
-
Consultant, general practitioner (GP) or specialty registrar: the aim was to recruit senior doctors (predominantly consultant level) to ensure credibility in delivering ‘Lessons Learnt’ to trainees and to promote sustainability of the intervention for subsequent cohorts of trainees.
-
Any clinical specialty: patient safety incidents occur in all healthcare specialties and furthermore trainees rotate through diverse specialties as part of their clinical training so it was important to ensure representation of senior doctors across all clinical disciplines.
-
Interest in patient safety: this criterion was kept deliberately simple, with doctors self-reporting their interest. This was done to maximise response among busy senior doctors by avoiding a complex application process.
-
Experience in facilitating group learning (eg, problem-based learning, communication skills training).
Course development and delivery
Course content and structure
The course content was mapped onto clearly defined learning objectives (box 1) which were in turn mapped to the requirements of the faculty role as part of the broader ‘Lessons Learnt’ project. Core content included Patient safety essentials, Root cause analysis of patient safety incidents, and The ‘Lessons Learnt’ project and faculty role and responsibility. Further information regarding course content and the educational modalities employed are summarised in table 1. The first two core content items were based on a previously developed and validated course.25
Lessons Learnt faculty course learning objectives
Patient safety knowledge
At the end of this course, participants will be able to:
-
Define a patient safety incident (PSI)
-
Describe the rates and types of PSIs in healthcare
-
Understand the nature of human error and the importance of systems factors in relation to patient safety
-
Understand the contributing factors to PSIs
-
Understand the mechanisms for learning from error
-
Review the principles of effective facilitation
Patient safety skills
At the end of this course, participants will be able to:
-
Recognise a patient safety incident
-
Analyse a PSI using a London protocol-driven approach
-
Facilitate group reflection and learning from error
Patient safety attitudes
At the end of this course, participants will acknowledge the need to:
-
Foster an open and learning culture to improve patient safety
-
Create opportunities for trainees to learn effectively from things that go wrong
-
Support trainees to engage in initiatives that aim to improve the quality of care
Lessons Learnt faculty course content and delivery
Course delivery
The course was delivered by expert faculty from the Imperial Centre for Patient Safety and Service Quality (http://www.cpssq.org). Two identical half-day courses were delivered during November 2010 in preparation for roll-out of the main ‘Lessons Learnt’ programme in January 2011. In line with educational theory, a combination of didactic and experiential teaching methods was employed to achieve Bloom's higher levels of application, analysis and synthesis.26 A comprehensive Facilitator Handbook containing course content and further resources was provided to all participants. The course was formally accredited with the UK's Royal College of Physicians. Recruitment and course delivery was repeated again to develop a second cohort of faculty commencing January–July 2012.
Course evaluation
Course evaluation comprised a prospective longitudinal study conducted over 2 years with testing conducted pre and immediately post intervention and retention tested with a further evaluation 8 months post intervention (‘year end’ for first faculty cohort). The study was approved as a training intervention evaluation from our local ethical review committee.
The evaluation was conducted based on Kirkpatrick's recommendations for complex training interventions:27
▸ Level 1(participants’ reaction/satisfaction): a course satisfaction questionnaire was developed and administered immediately post course. Participants used a five-point Likert scale to rate course delivery, how well the learning objectives were met, and overall satisfaction with the course.
▸ Level 2 (participants’ learning—knowledge, attitudes and skills): these were assessed immediately pre and post course. Knowledge was assessed objectively through multiple-choice questions mapped on to course content and also subjectively through a validated scale.28 Patient safety attitudes were assessed through a validated questionnaire.28 Confidence in facilitation skills was assessed through a self-report questionnaire. Items included confidence in ‘Analysing a patient safety incident’, ‘Facilitating group reflection on patient safety incidents’ and ‘Supporting and advising trainees on how to respond to a patient safety incident (PSI)’ assessed on a five-point Likert scale (1=very low confidence to 5=very high confidence).
▸ Level 3 (behavioural change): in the context of the ‘Lessons Learnt’ programme behavioural change was assessed by subsequent engagement in the programme as faculty and by trainee assessment of facilitation skills. Trainee ‘Leads’ at each site were asked to complete a faculty assessment at the end of every ‘Lessons Learnt’ session. Items were assessed on five-point Likert scales and mapped to the faculty role description to include general approach to facilitation, for example, putting trainees at ease; discussion and analysis of incident, for example, encouraging discussion around aetiology and preventive actions; and summary and next steps, for example, reinforcing lessons learnt and formulating an action plan.
Retention survey
At the close of the first year of roll-out of the ‘Lessons Learnt’ project in July 2011 (approximately 8 months post course) a further evaluation was administered to the faculty cohort via an online survey (a similar evaluation in the second year of the project was not feasible due to financial limitations). This included repeat evaluation of patient safety knowledge, attitudes and skills as conducted pre and immediately post course. Items relating to engagement in the ‘Lessons Learnt’ project were also included (eg, number of sessions facilitated, desire to continue, etc) and rated on five-point Likert scales. The survey was administered electronically using SurveyMonkey software. An email invitation to complete the survey online was sent directly to participants with a reminder sent every 2 weeks to non-responders.
Analysis
SPSS V.19.0 was used for all analyses. Descriptive statistics were reported for demographics, pre and post course and 8 months post course/retention scores and course satisfaction. The non-parametric Wilcoxon signed rank test was used to conduct matched pair-wise comparisons of knowledge, skills and attitudes pre and immediately post course and again to compare post course with scores at 8 months post course (first cohort only). Cronbach's α was used to assess the internal consistency (scale reliability) of survey subscales (self-report knowledge, self-report skills and attitudes).
Results
Demographics
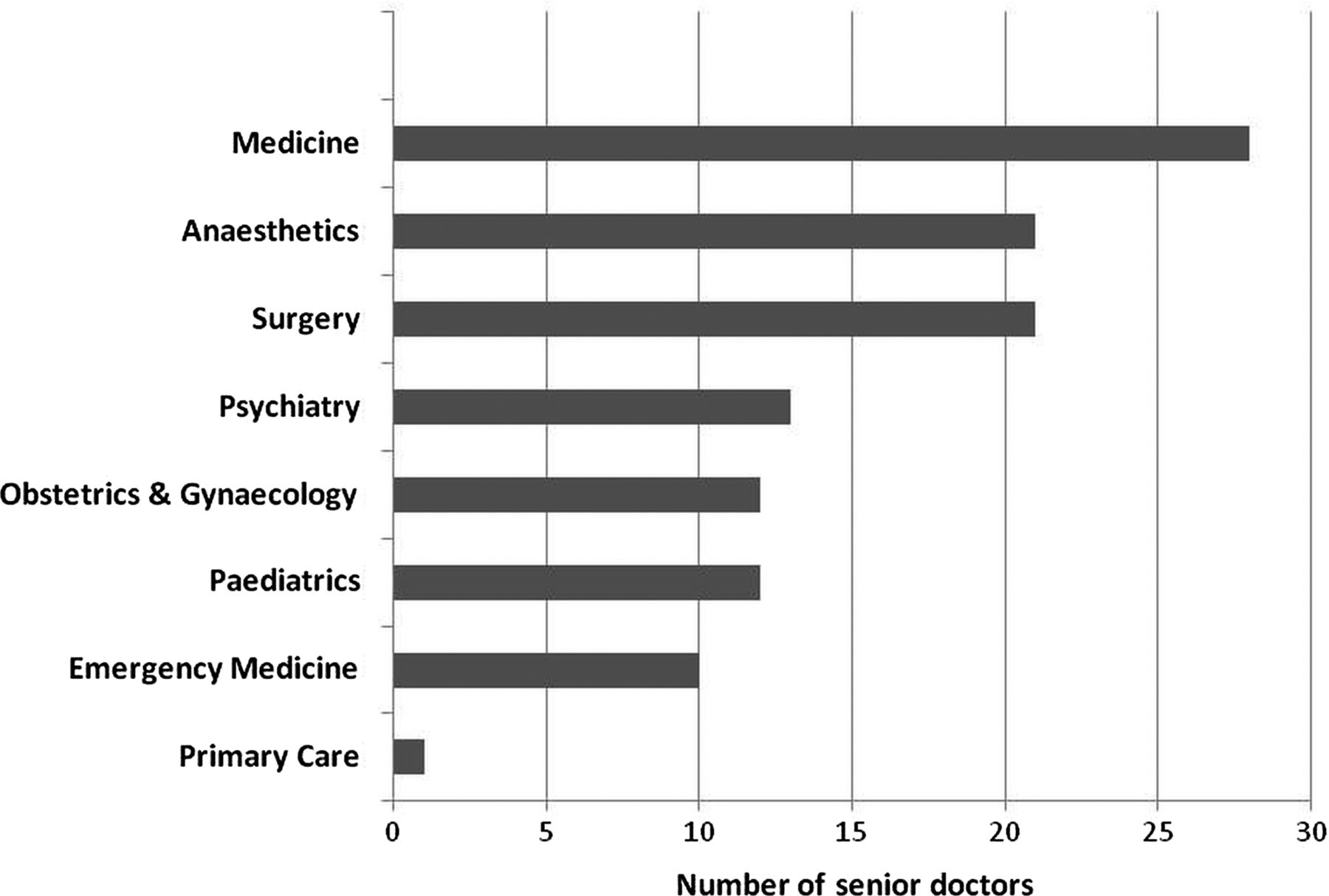
Over the 2-year study a total of 216 senior doctors across 20 hospitals volunteered to enrol as ‘Lessons Learnt’ faculty. One hundred and twenty-two doctors were appointed based on the inclusion criteria and course capacity (figure 1). In the majority of cases non-attendance at the course following invitation was attributed to last-minute clinical commitments. The majority of faculty were consultant grade (84%) followed by specialty registrars (16%). Of the consultant grade faculty, the majority (52%) had been in post for 5 years or less; 20% had been in post for 6–10 years and a further 28% for over 10 years (determined via the General Medical Council's list of registered medical practitioners). The most common specialties of appointed faculty were anaesthesia, medicine and surgery and the least common was primary care (figure 2).
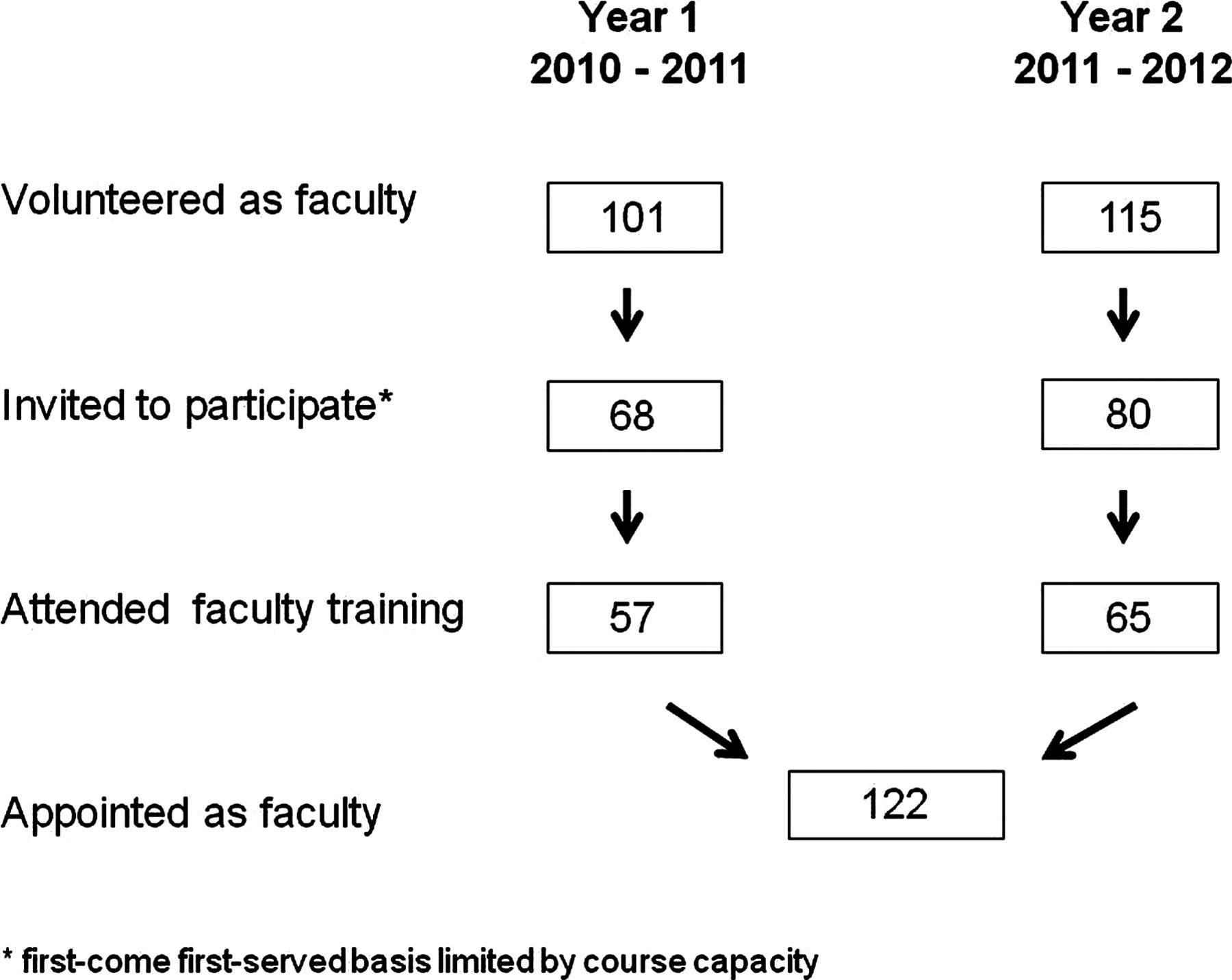
Faculty recruitment flowchart.
{kind=link}
{kind=link}
Specialty of senior doctors appointed as Lessons Learnt faculty.
Pre–post course evaluation
In year one (2010–2011) 50 faculty (88%) completed the baseline evaluation, 49 (86%) completed the immediate post-course evaluation permitting 45 (79%) matched pair-wise analyses. In year two (2011–2012) 59 faculty (91%) completed the baseline evaluation, 53 (82%) completed the immediate post-course evaluation permitting 47 (72%) matched pair-wise analyses. Therefore there was a total of 92 matched pair-wise comparisons pre–post course on these measures.
Course satisfaction
Across both cohorts, participants reported very high levels of satisfaction with the course in terms of content (eg, 92% agreed or strongly agreed that the course ‘Improved my understanding of how to analyse a patient safety incident’), course delivery (93% agreed or strongly agreed that ‘The information was provided in a way which was easy to understand’) and overall satisfaction (eg, 89% would strongly recommend the course to a colleague). Free-text strengths of the course included ‘well organised’, ‘explicit objectives set and achieved’ and ‘interactive small-group work’. Suggestions for improvement mainly related to extending the time available to allow for more group discussion.
Patient safety knowledge
Across both cohorts there was a significant improvement in objective scores of patient safety knowledge from a pre-course median of 70% (range 10–100%) to a post-course median of 80% (40–100%; p<0.001). Self-report scores of knowledge also improved significantly post course: pre-course median 3.43 (1.86–4.71), post-course median 4.00 (3.14–5.00; p<0.001). Reliability in the form of internal consistency of this scale was very high (Cronbach αPre course=0.878, Cronbach αPost course=0.924).
Patient safety attitudes
Across both cohorts there was a significant improvement in patient safety attitudes post course, including the domains of ‘feelings’, ‘ability to influence’ and ‘intentions’ (table 2). Internal consistency for the various attitude scales ranged from 0.516 to 0.934 (see supplementary web appendix 2).
Participant patient safety attitudes pre and post course
Patient safety skills
Across both cohorts self-reported confidence in patient safety skills (eg, ability to analyse a PSI) significantly improved immediately post course (MedianPre course=3.38, range 1.75–5.00; MedianPost course=4.13, range: 3.00–5.00; p<0.001). Internal consistency for this scale was excellent (Cronbach αPre course=0.915, Cronbach αPost course=0.903).
Retention survey results (first faculty cohort only)
Twenty-nine (51%) participants completed the retention evaluation at 8 months post intervention, permitting 28 matched pair-wise analyses. Objective scores of patient safety knowledge 8 months post intervention were sustained without significant loss (in fact, there was an improvement in the scores, albeit non-significant), from 80% (60–100%) immediately post course to 90% (60–100%) at 8 months (p=0.28). Similarly, self-reported knowledge was sustained: median 4.00 (3.15–5.00) immediately post course to median 4.00 (3.00–5.00; p=0.19). Improvements in patient safety attitudes were also sustained (table 2). Finally, post-course improvement in self-reported patient safety skills was also evident without any significant skill loss at year end: median 4.13 (3.25–5.00) immediately post course to median 4.00 (3.00–5.00) at 8 months post course (p=0.19). Internal consistency for scales was excellent at retention for self-reported knowledge (Cronbach α=0.924), skills (Cronbach α=0.910) and attitudes (web appendix 2).
Engagement in the ‘Lessons Learnt’ programme
Through combined analysis of trainee assessments and participant self-report, 88 (72%) faculty facilitated a total of 213 ‘Lessons Learnt’ sessions between January 2011 and July 2012, an average of two sessions per faculty member (range 1–8). Trainees rated faculty highly across all domains of facilitation skills: general approach to facilitation (median=4.20, range 2.40–5.00); discussion and analysis of incident (median=4.25, range 2.50–5.00); and summary and next steps (median=4.00, range 2.00–5.00). Of the first faculty cohort surveyed 8 months post course, 25 (89%) participants agreed/strongly agreed to stay on the programme as faculty and 19 (68%) agreed/strongly agreed to support training of subsequent cohorts of faculty. The most commonly cited barrier/challenge to facilitating ‘Lessons Learnt’ sessions was clinical commitments clashing with scheduled sessions. The most commonly cited enablers to participation were enthusiastic trainees and supportive administrative staff.
Discussion
There are increasing calls for clinicians to actively take on leadership roles to drive safety and quality improvement efforts.6 ,7 With over 200 applicants for the ‘Lessons Learnt’ faculty role, our study shows that there is considerable appetite for senior doctors to engage in patient safety training as learners and teachers. Our short course in patient safety and incident analysis was well received by senior doctors and led to significant improvements in safety knowledge, self-reported skills and attitudes. These improvements were sustained 8 months after the course, which we interpret as due to the faculty training course itself but also the ongoing ‘exposure’ to this subject and systematic application of learning through facilitation of ‘Lessons Learnt’ sessions.
Our training course has been oversubscribed for two consecutive years, thereby developing faculty to deliver patient safety training to two successive cohorts of 1500+ trainees from 2010 to 2012. We believe that our approach in particular has an inclusive person specification, provides a free accredited course, and the explicit role description together with perceived benefits serve to promote recruitment and engagement of senior doctors as core faculty (interested readers may refer to supplementary web appendix 1: recruitment flyer). The majority of appointed faculty (72%) went on to facilitate ‘Lessons Learnt’ sessions. Trainees rated faculty highly. Not surprisingly, the most commonly cited barrier to attending the training course and going on to facilitate ‘Lessons Learnt’ sessions was clinical commitments. Importantly, trainee enthusiasm and administrative support were enablers to facilitation, as noted elsewhere.11 Previous efforts to administer quality and safety training to senior clinicians have not focused on doctors but on nursing staff, among whom recruitment has proved less challenging.12 When doctors have been targeted, evaluation of the training intervention has been lacking.13
The majority of faculty came from the specialties of medicine, surgery and anaesthetics. The greater engagement of medical and surgical senior doctors may reflect their historical contribution to teaching programmes as part of early postgraduate medical training (which now forms the Foundation Programme). The high recruitment among anaesthetists supports the view of anaesthesia as the ‘leading medical specialty in addressing patient safety’.29 Conversely, recruitment among primary care doctors (GPs) was poor. This may be partly due to issues of service configuration and remuneration whereby GPs are independently contracted to the National Health Service. Indeed, given that clinical rotations in primary care account for one-sixth of the Foundation Programme in our Deanery, we plan to launch targeted recruitment for GPs in subsequent cohorts of the ‘Lessons Learnt’ programme. Moreover, the majority of faculty were ‘junior’ consultants, having been in the post for 5 years or less. This may reflect the naturally high enthusiasm among this cohort in wishing to expand their portfolio of work to include involvement in teaching and patient safety. Finally, while 89% of our first faculty cohort agreed to continue in their role, only 68% agreed to support the training of subsequent cohorts. We believe that perceived lack of time may explain this finding. This requires further exploration as we aim for faculty ownership and the wider sustainability of the ‘Lessons Learnt’ programme.
In terms of limitations, our sample size was confined within a single health region of the UK and therefore the generalisability of our findings could be questioned. However, participants were recruited from a wide geographical area across a diverse range of clinical specialties so we are confident that our results are transferable to other settings. Our approach to recruitment deliberately targeted senior doctors with an interest in patient safety so selection bias cannot be excluded. Notably, the effect size of pre–post course improvements in knowledge, self-reported skills and attitudes were small yet significant. It may be that in the ‘general’ senior clinical population the pre-course scores would be lower yielding larger effects post course. Ultimately our aim was to recruit a cohort of senior doctors who would go on to act as ‘Lessons Learnt’ faculty so we believe our inclusion criteria were justified. The first faculty cohort response rate at 8 months was only 51% so we can be less certain in our results. However, the response rate is comparable to other internet-based surveys of clinicians.30 We suspect that our lengthy survey affected completion at year end, nevertheless it is reassuring that the majority of participants wish to continue in their role as ‘Lessons Learnt’ faculty.
In summary, we have succeeded in developing a stable cohort of enthusiastic senior faculty in patient safety. It is crucial not only to develop and deliver quality and safety training to senior clinicians but also to carve out opportunities to apply this learning, be it as a facilitator of incident analysis (as with ‘Lessons Learnt’) or as a facilitator of quality improvement projects as published elsewhere.17 ,31 Political incentives in the form of alignment to professional regulatory standards and reference to the wider health policy landscape are also powerful levers in promoting clinical engagement in quality and safety.7 ,15 ,32 ,33 Further work should seek to develop and evaluate more advanced team-based courses for senior healthcare professionals to foster skills in quality improvement and capitalise on health policy incentives (such as Quality, Innovation, Productivity and Prevention (QIPP) in the UK)33 to help bridge the gap between safety training and quality improvement on the ground. Finally, there needs to be clear recognition and reward for senior doctors engaging in quality and safety training activities with protected time for them to do so.6 ,14
Conclusion
There is considerable appetite for senior doctors to engage with training in patient safety as teachers and learners. We developed and evaluated in detail a short course, which was well received by senior doctors and resulted in significant improvements in safety knowledge, self-reported skills and attitudes. Training senior doctors in patient safety is feasible, acceptable and efficacious as a means of building capacity and capability for delivering training in this rapidly emerging field. All course materials are available to interested readers for implementation within their own institutions (via the corresponding author).
Acknowledgments
The authors wish to thank Fizza Ahmed for her assistance with data input, Matthew Kirkman and Stephenie Tiew for their support with course administration and Ana Wheelock for the Facilitator Handbook design. We also wish to thank all participants in this study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online appendix 1
- Data supplement 2 - Online appendix 2
Footnotes
-
Contributors MA conceived and designed the study, analysed and interpreted the data and drafted the manuscript. SA, NS and CV designed the study, interpreted the data, and revised the manuscript for important intellectual content. PB and JH acquired and interpreted the data and revised the manuscript for important intellectual content. MA and NS had full access to all of the data in the study and can take responsibility for the integrity of the data and the accuracy of the data analysis. All authors approved the final version to be published. MA is guarantor.
-
Funding This study was funded through the ‘NHS North West Junior Doctor Innovation Award in Education and Training’ and the National Institute for Health Research (NIHR) via the Imperial Centre for Patient Safety and Service Quality (http://www.cpssq.org). Additional event sponsorship for course delivery and materials was provided by the Medical Protection Society (MPS).
-
Competing interests All authors have completed the ICMJE uniform disclosure form at http://www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author). MA, SA, NS and CV are affiliated with the Imperial Centre for Patient Safety and Service Quality which is funded by the National Institute for Health Research, UK. MA, SA and NS received consultancy fees for this project from NHS North West via Central Manchester Foundation Trust. MA and JH are Education Associates at the General Medical Council. JH is Dean of Postgraduate Medical Studies, North Western Deanery. MA is a member of the Strategic Advisory Board, BMJ Quality and has previously undertaken consultancy work for Medical Education England. CV conducts occasional consultancy work as part of Vincent Burnett and receives book royalties from Wiley-Blackwell. This study is part of the ‘Lessons Learnt: Building a Safer Foundation’ programme which won the BMJ Group Excellence in Healthcare Education Award, 2012.
-
Patient consent Obtained.
-
Ethics approval Deemed not necessary by North West 7 Research Ethics Committee, Greater Manchester Central.
-
Provenance and peer review Not commissioned; internally peer reviewed.