Article Text

Statistics from Altmetric.com
Compassion has historically been defined as an underpinning principle of work conducted by health professionals, especially nurses.1 Numerous definitions of compassionate care exist, incorporating a range of elements. Most include a cognitive element: understanding what is important to the other by exploring their perspective; a volitional element: choosing to act to try and alleviate the other’s disquiet; an affective element: actively imagining what the other is going through; an altruistic element: reacting to the other’s needs selflessly; and a moral element: to not show compassion may compound any pain or distress already being experienced by the other.2 3 Appeals for more compassionate care have become common within international discourses, through initiatives such as Schwartz Rounds established in America, Hearts in Healthcare in New Zealand, and the Asia Pacific Healthcare Hub of Charter for Compassion. In the UK, a policy document called Compassion in Practice outlined 6 ‘Cs’ associated with compassionate care (care, compassion, courage, communication, commitment and competence). It was written in the wake of high profile accounts of negative health services experiences, including the 2013 Francis Report (http://webarchive.nationalarchives.gov.uk/20150407084231/http://www.midstaffspublicinquiry.com/report), which detailed the dehumanising treatment of patients at Mid Staffordshire NHS Trust. Positioned as a solution to neglect and unsafe treatment, contemporary debate around practice and policy often paints compassionate care as an easy, cost-neutral fix for entrenched problems in modern health services. Yet delivering compassionate care is not without costs. First, staff may have to engage in emotionally charged interactions, which can leave them feeling psychologically exhausted and at risk of burnout.4 Furthermore, for health professionals to be able to connect with patients and understand their unique situation, while also addressing fundamental needs (eg, hygiene, feeding) in a non-mechanistic manner, an appropriately resourced workplace is required.5
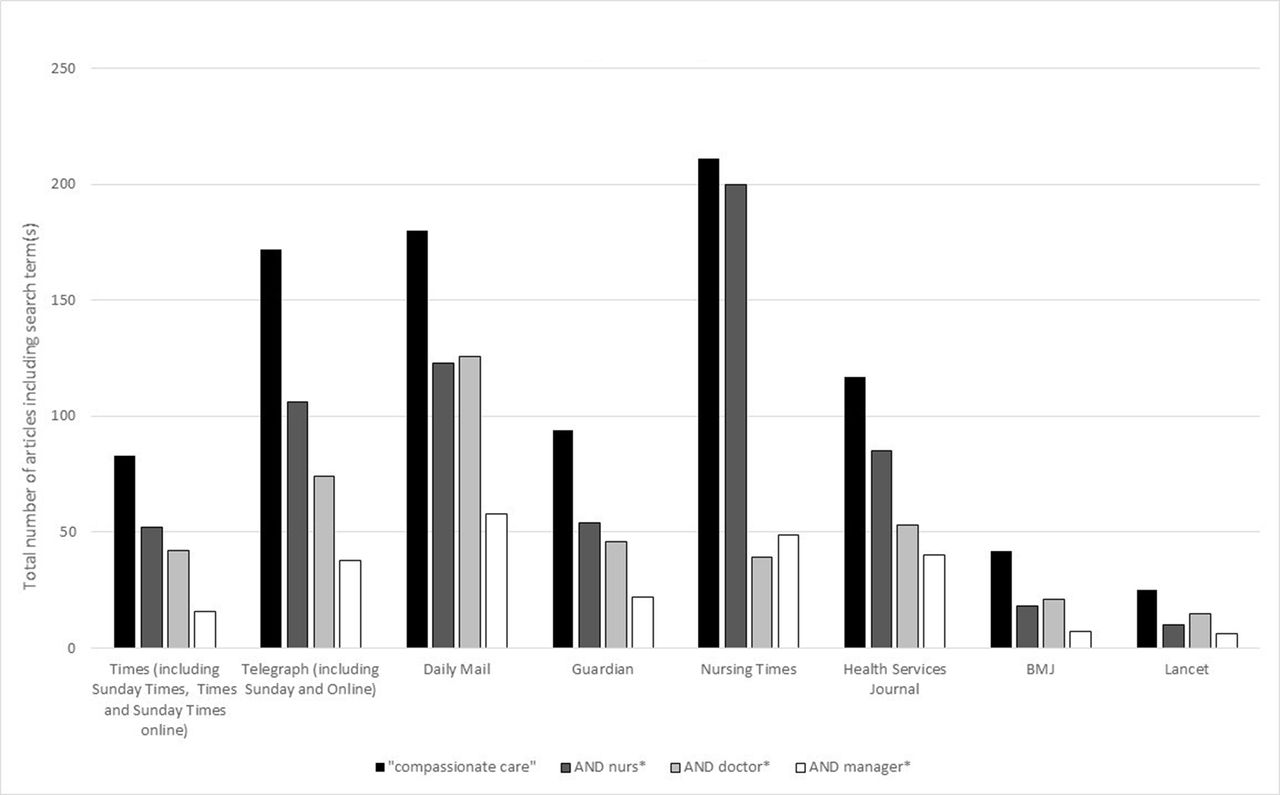
Nursing, in particular, has been linked to contemporary discussions of compassionate care.6 We surveyed UK coverage of ‘compassionate care’ using keyword searches for this exact phrase both alone and in conjunction with additional search terms (nurse*, doctor*, manager*) across the full-text digitised content of a mix of professional and lay periodicals available through Scopus, Factiva and on individual journals, between 2007 and 2017. We included unique articles only, eliminated content categories unrelated to current debates (eg, obituaries) and hand-searched a sample of texts from each periodical to ensure that our search parameters successfully identified relevant content. The results are displayed in figure 1. Notably, compassionate care received far greater attention from the nursing and health services press than from medical journals. In the medical journals, compassionate care discourse focused, unsurprisingly, on doctors’ roles in commissioning and ensuring a compassionate environment for patients. However, closer scrutiny reveals that nurses remained providers of that care at the bedside. In the popular press, too, discussions of compassionate care (largely critical) were generally associated with nursing. In the sole UK newspaper in which discussions of compassionate care did mention doctors marginally more often than nurses, coverage reflected the trend visible in the medical press to position nurses as its direct providers. Perhaps most revealingly, none of these outlets gave significant attention to senior managers as key agents facilitating the provision of compassionate care.
{kind=link}
UK coverage of ‘compassionate care’ from 2007-2017.
This linkage between nurses and delivery of compassionate care is not new. Going back to the work of Florence Nightingale, nursing was associated with an idea of doing God’s work through attending to those in need,7 highlighting a strong religious undercurrent as the profession was established. It also reflects early understandings of the ‘nursing character’, depicted by Nightingale and those who followed her in terms of qualities such as gentleness, kindness and courtesy.1 As nursing evolved from the mid-19th century onwards into a more regulated, professional activity, fundamentally different from the untrained or familial care that preceded it,8 the cultural expectation that nurses would have a selfless calling to care persisted.1 By binding responsibility for direct compassion in modern healthcare so tightly to the nursing workforce, this discourse has uncritically adopted a set of assumptions with a deep and highly problematic history.9
The emergence of nursing as a profession was facilitated by now-discarded views of caring as a form of labour to which women were uniquely adapted by their domesticity.8 Sympathy as much as skill initially sanctioned the professional nurse’s entry into homes and hospital wards to replace the stereotypically coarse, uncaring and untrained ‘Sarah Gamp’ depicted in Dickens’ Martin Chuzzlewit.10 ‘Nursing’ and ‘caring’ remained largely synonymous even as late 19th-century and 20th-century nurse training programmes and literatures demanded ever-increasing levels of knowledge and specialised skills.11 These changes accelerated with the growing use of complex biomedical and technological interventions, driving up levels of educational and specialist attainment required by employers and regulatory bodies, and displacing the earlier dominance both in training and in practice on bedside or ‘direct’ nursing.12 By the 1960s, the nursing literature documented unease with what was perceived as a growing dichotomy at the heart of nursing between the ‘supportive, affective’ work of the bedside ‘mother surrogate’ and the ‘business-like’ efficiency of a ‘dispassionate healer’.13
In postwar Britain, international trends towards division in the nursing role were further shaped by the distinctive context of a universal comprehensive health service, funded from general taxation, and subject to both national and local control mechanisms. Under these circumstances, and particularly in the past quarter century, political and economic expediency have acted on understandings of nursing. Synchronistically, changes in educational models and pathways to professional advancement have largely demanded and rewarded nurses for specialisation and management roles, while ‘skilled bedside nursing’ only rarely attracted similar support.14 However, senior nurses with a more limited bedside role continued to be key in engendering a compassionate culture in terms of role modelling and through philosophical, theoretical and educational support.15
Internal markets, managerialism and the corresponding drive to define and then achieve quantifiable levels of quality and efficiency across the health service have promoted greater interest in metricised markers of adequacy and excellence, including in the provision of compassion in nursing.16 Yet calls to measure compassionate care remain contentious, not least because what this constitutes is ambiguous and dynamic.5 Moreover, compassion inheres to human interactions, which forms a key part of influential models from nursing, such as Watson’s theory of human caring17; assessing this relies on subjective experiences of patients and carers, making conventional measurement strategies problematic.
Setting aside the challenges inherent to assessing levels of personal compassion, whether by examination or interview, a focus on individuals’ behaviour overlooks the integrated nature of modern healthcare,5 which represents a delicate and multifaceted ecosystem. As Dutton and colleagues18 show, organisations do not become compassionate by hiring caring people. Rather, practising compassion requires a facilitating social architecture promoting norms of trust, concern and empathy, in which compassion is treated as a collective responsibility, rooted in well-defined practices across the whole range of staff roles. Hence, although compassionate care calls for specific skills and knowledge, which can be exhibited by individual nurses and other healthcare professionals, it must also be facilitated through an environment that provides required structural resources (eg, staffing levels, training in things like culturally congruent care) and transformative leadership.5
Creating a compassionate workplace can have a positive impact on people’s commitment to an organisation and how they view their colleagues, alongside helping them to deal with suffering and distress they face in their job.18 Perceptions of one’s organisation can be shaped by experiencing compassion first-hand, and from seeing others receive such treatment,19 which promotes staff resiliency. Leaders can play a central role in this respect, both by actively demonstrating the importance of noticing, feeling and responding to suffering,20 and by expressing emotions themselves as an acceptable way of working.19 This can help organisations to institutionalise compassion so it becomes self-sustaining.19
In the complex environment of modern health services, caring—for patients, for staff and for the organisations that enfold them—must be a shared responsibility, since no single individual or professional group can ensure the delivery of compassionate care. It is all too easy for society to blame a single profession (in this case nursing) rather than tackling the challenges of system-level change. Correspondingly, the knee-jerk clamour for restored or increased levels of compassion in nursing in response to each episode of bad care is conditioned by our long and uncomfortable history of delegating the low status, unpaid emotional labour of caring to nurses, initially as women, then as subordinated professionals.
Only latterly—and still gradually—has the clinical environment moved towards mutual respect for each discipline’s contributions. Healthcare systems have traditionally undervalued both the work and the providers of compassion economically, relying instead on cultural and social norms that have placed this work at the centre of one particular professional identity—that of the nurse—to ensure that it gets done. In today’s target-driven and economically stretched systems, where ‘what is counted counts’, efforts to promote compassionate care have too often been framed in terms of developing metrics to assess proxies for individual compassion; these have specifically targeted nurses despite the system-level constraints that shape their work. We propose instead that while nursing leaders and the profession as a whole have important roles to play as advocates for compassionate care, they cannot be its sole guardians. Nurses do have enormous experience to call on in shaping empathetic, resilient organisations, in which compassionate care will continue to be the norm—but they cannot do it alone, or on the cheap.
Footnotes
Contributors All contributors were involved in planning and writing this paper.
Funding RB holds a Wellcome Trust Senior Investigator Award, grant number 104837/Z/14/Z (title ’The Cultural History of the NHS').
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.