Article Text

Statistics from Altmetric.com
All parents want the same for their child
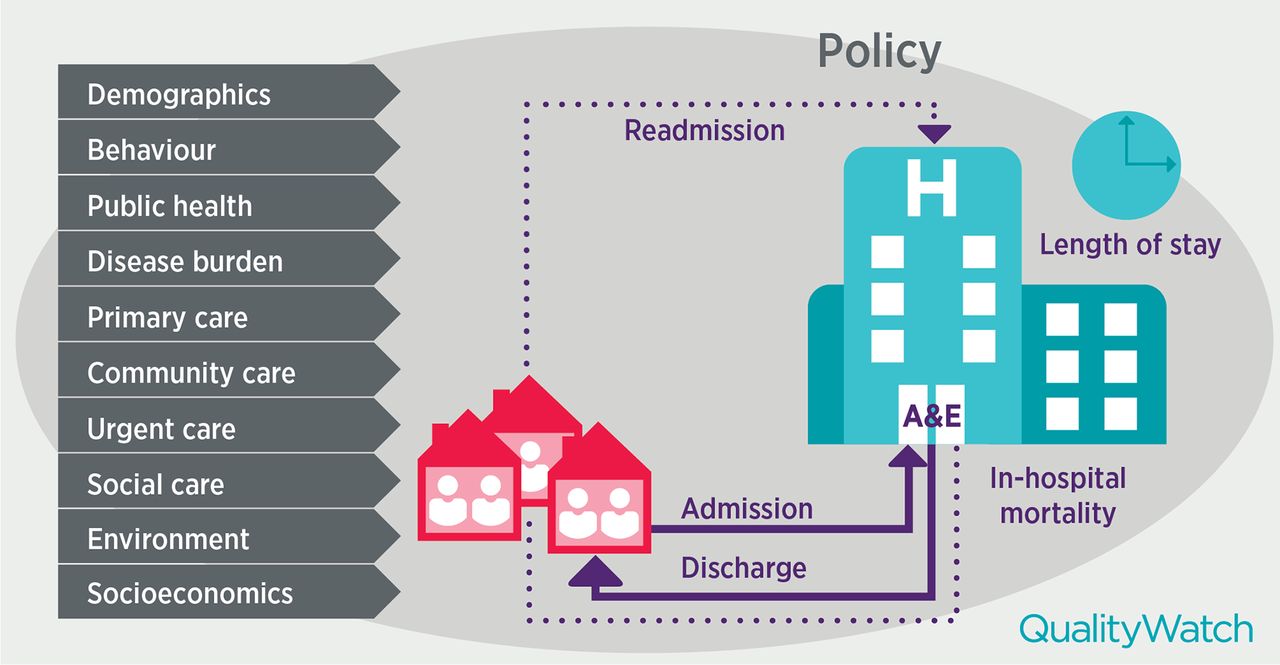
Emergency department (ED) visits and hospital admissions are often monitored to get an understanding of urgent hospital activity, but are also used as an indicator of the accessibility and quality of services outside the hospital. The factors determining whether or not a family will seek care in the ED and be admitted are complex (figure 1), and this picture becomes even more complex when comparing between areas or countries. One thing that can be counted on, however, is that regardless of country, nationality, health system or personal preferences, all parents are likely to want the same for their child: for them to receive the best care possible—care that is easily accessible, safe, effective, most appropriate for their needs and provided in a caring environment.

{kind=link}
Factors influencing the use of emergency hospital care by children and young people (A&E: Accident and Emergency Department).
When a parent becomes concerned about their child’s health, they need reassurance and advice which may or may not lead to a hospital stay. Where they seek care will depend on a number of factors: how unwell the child seems to them, how knowledgeable and empowered they feel to help their child without medical advice, the time of the day and other responsibilities they may have (eg, work, another child and others), as well as what health professional is accessible to them and how much they trust their advice. Any previous experience with the healthcare system will also be an important factor in deciding what to do and where to seek help—be it at the ED of the hospital, an urgent care centre, the local general practitioner, paediatrician or nurse.
The options available to parents vary by country (or even by region), and these differences may lead to different outcomes, but not always. There can be different clinical interventions and organisational reforms that will lead to improvement in health outcomes. Evidence-based guidelines are available to help clinicians deliver the best possible care to patients. But we know that their implementation nationally and internationally varies. However, there is less clarity on how services should be organised to deliver the best care to patients. For example, while there is gatekeeping in the UK and other countries have been setting up their primary healthcare systems based on the UK’s, there is little evidence that gatekeeping helps improve health outcomes and contain costs.1 Therefore, careful review and comparisons of different systems and outcomes, such as the large European Union project looking at primary care systems for children and young people across 30 countries,2 are essential for gaining more clarity about the types of system, or instead design principles3 that may help deliver the desired health outcomes for children and young people.
The study by Harron et al 4 in this issue of BMJ Quality and Safety makes a valuable contribution to this body of evidence, as it examines similarities and differences in emergency hospital use by infants in England and Ontario, Canada, and how these could be explained. The study focused on understanding hospital care use in the 12 months following postnatal discharge for a cohort of infants. Infants were identified from linked administrative hospital data, taking the birth record associated with the mother and linking to subsequent admissions for the baby.4 Risk factors relating to birth such as gestational age and maternal risk factors such as deprivation could, therefore, be accounted for.
Rising emergency hospital admissions in England and Ontario…but forms of emergency care use differ
In a recent study,5 we found that emergency hospital admissions for children and young people in England, and infants in particular, have continued to increase in the recent decade. Given other available evidence, we hypothesised that this increase may be due to accessibility and quality of services outside the emergency hospital care setting, but also the quality and accessibility of services provided in the hospitals.
In this new study, Harron and colleagues4 identified similar trends in emergency hospital use for infants in England and Ontario, Canada. The authors found that the proportions of infants with emergency hospital contacts—ED visits or unplanned admissions—were similar in Ontario and England (42.9% and 41.6%, respectively); however, the composition of these contacts varied. Infants in England were more likely to be admitted if they attended an ED, and linked to this were more likely to have more than one admission. Once admitted infants in England were less likely to stay overnight than infants admitted in Ontario. Despite lower admission rates overall, the proportion of infants readmitted with neonatal jaundice was substantially higher in Ontario than England. Gestational age and maternal age were the most important risk factors for an unplanned admission, and so was deprivation, particularly for ED visits. The two countries differ on certain aspects of healthcare, including access to midwives and health visitors (more accessible in England), the presence of consultant paediatricians in the ED (more accessible in Ontario), and ED waiting time targets with more pressure to admit in England. Overall, however, the healthcare systems are thought to be similar enough to offer meaningful comparisons.
How are these international comparisons useful?
An additional lens and source of inspiration
International comparisons are an essential component of understanding and improving quality of care, as they provide an additional lens to time series and regional variations. For example, national infant mortality rates may seem low in the UK (3.9 per 1000 live births in 2014), but relative to Sweden (2.2 per 1000 live births in 2014) the UK has almost double the rate.6 At the same time, the most deprived in the UK have higher and increasing infant mortality rates relative to the least deprived,7 and there is variation between and within the four countries,6 equivalent to some of the best and worst performing countries of the Organisation for Economic Co-operation and Development (OECD).8
International comparisons provide an additional lens on how countries perform on given quality of care indicators and provide the basis for asking and initiating debate—why are we observing these differences? Is it just a data artefact or a true difference in the quality of care provided? Are other factors driving these differences? The more data from different sources, levels of detail and methodologies (qualitative and quantitative) that can be triangulated to answer these questions, the better. While there is no doubt that international comparisons have many challenges, especially around data quality and comparability,9 10 if done carefully, they also have the ability to bring attention to areas where countries excel or could learn from each other.10
Different routes to the same outcome
The findings of Harron et al highlight how two countries that have generally very similar healthcare systems still have different healthcare seeking behaviours and provision of care that result in different patterns of emergency care utilisation. The devil is in the detail.
As the authors suggest, a proportion of emergency care use in the hospital for infants, in particular hospital admissions, could be avoided. Hence the patterns of emergency care use are considered the health outcome of interest for children and young people. However, looking at some of these findings more carefully, we learn that an ‘ED visit’ or an ‘admission’ may not be the same in the two countries. While it may only seem a definitional challenge, it has important implications for what decisions can be drawn from these kinds of comparisons.
The results suggest that the way care is provided in the community and in the ED in the two countries does differ—on the one hand, the proportion of infants seeking care in EDs being smaller in England than in Ontario may suggest that families have more options outside the ED setting in England, or that the greater availability of trained emergency paediatricians in the ED in Ontario acts as a ‘pull factor’. (The authors acknowledge that they could not directly measure this availability, but point out that Canada has far more established training in paediatric emergency medicine than does England.) On the other hand, more infants being admitted in England but staying shorter periods in the hospital again raises questions about how EDs and wards are run in the two countries. The authors discussed a range of factors that could have an influence on the higher proportion of children admitted as an emergency in England—differences in the population, hospital staffing, skills of staff, hospital factors such as number of beds and incentives, patient factors (eg, deprivation, ability to cope), or disease severity, among others. For example, Harron et al hypothesise that the presence of paediatric expertise in EDs in Ontario and targets to admit within 4 hours in England may be linked to a lower proportion of children and young people being admitted in Ontario. We also learnt that the percentage of infants in England who are discharged on the same day as admission is significantly higher than in Ontario—could this difference simply be because infants stay longer for observation in the ED in Ontario while in England they are admitted (due to the targets), but with short stay admissions in England more common, overall infants are spending the same amount of time in hospital?
So what’s next?
The results of this study point to some more specific questions, and possibly actions. For example, we could:
Remove targets in England so there is more time to observe the child/infant in the ED and decide whether admission is appropriate. That may (or may not) reduce emergency admissions, and may (or may not) improve the quality of care provided to infants. However, the more important question here may be: where do infants at present receive the most appropriate observation and advice? Does it matter if they are observed in the ED or admitted to the ward? What is the role of the new paediatric short stay units and how is the observation of a child in these units coded in the data?
Have more senior paediatricians in the ED in England. Would these paediatricians help reduce emergency admissions or are other hospital factors (ie, targets, bed capacity) or the care available in the community more important? Would strengthening of capacity and skills in the ED act as a further ‘pull factor’ to EDs and possibly lead to more admissions? Also, where would these senior paediatricians come from in the short term? Should they instead provide emergency care outside the hospital emergency care setting? How similar/different are the qualifications/skills of paediatricians in Ontario versus England?
Start by asking why does a higher proportion of infants end up in the ED in Ontario than in England rather than focusing on reducing the proportion of children who get admitted and discharged on the same day? Could we simply increase the numbers of health visitors and midwives in Ontario? Or would other support for deprived families be more appropriate to reduce the number of times they seek care in the ED? What could Ontario do differently? Given all the evidence available for England and desire to reduce ED attendance rates and emergency admissions, it may be wise to carry out a similar analysis with a handful of countries that have different primary care systems as those findings may reveal entirely different solutions.
International comparisons help us consider these types of questions. Ultimately, we need to know what we are trying to achieve, with what resources and over what period of time, as any small change in the pathway of care will have a knock-on effect on other bits of the system, and while feasible in one setting may be impossible in another. The Harron et al study is a very valuable addition to the research evidence as it has already compared different parts of the emergency care seeking route. Can we say at this stage whether infants in England or Ontario receive better quality care and have better outcomes? Without the next level of in-depth review of the specifics of care along the full pathway in both countries, and a strong focus on outcomes, we cannot. We need a better understanding of what service change may or may not work, and under what circumstances and the relationship between structure and processes of care, but especially general design principles that are likely to lead to improved outcomes.3 For example, the new models of care emerging in England that aim to reduce emergency care activity11 may all be doing it slightly differently, but all have a strong preventative approach as a key design principle that helps them achieve their goal. These need to be carefully evaluated.
There may be different routes to the same outcome, but there may be some preferred ones. National and international comparisons help us learn what these are. They do not provide definitive answers, but help us raise the right questions.
Footnotes
Handling editor Kaveh G Shojania
Competing interests None declared.
Provenance and peer review Commissioned; internally peer reviewed.