Article Text

Abstract
Objective Patients living with HIV infection (PLWH) in sub-Saharan Africa face an important burden of treatment related to everything they do to take care of their health: doctor visits, tests, regular refills, travels, and so on. In this study, we involved PLWH in proposing ideas on how to decrease their burden of treatment and assessed to what extent these propositions could be implemented in care.
Methods Adult PLWH recruited in three HIV care centres in Côte d’Ivoire participated in qualitative interviews starting with ‘What do you believe are the most important things to change in your care to improve your burden of treatment?’ Two independent investigators conducted a thematic analysis to identify and classify patients' propositions to decrease their burden of treatment. A group of experts involving patients, health professionals, hospital leaders and policymakers evaluated each patient proposition to assess its feasibility.
Results Between February and April 2017, 326 participants shared 748 ideas to decrease their burden of treatment. These ideas were grouped into 59 unique patient propositions to improve their personal care and the organisation of their hospital or clinic and/or the health system. Experts considered that 27 (46%), 19 (32%) and 13 (22%) of patients' propositions were easy, moderate and difficult, respectively, to implement. A total of 118 (36%) participants offered at least one proposition considered easily implementable by our experts.
Conclusion Asking PLWH in sub-Saharan Africa about how their care could be improved led to identifying meaningful propositions. According to experts, half of the ideas identified could be implemented easily at low cost for minimally disruptive HIV care.
- burden of treatment
- Sub-Saharan Africa
- patient empowerment
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
Patients living with HIV infection (PLWH) in sub-Saharan Africa face many barriers in their care: out-of-pocket expenses, time spent travelling and attending clinical appointments, stigma and fear of disclosure, drug stock-outs, and so on.1–3 All these barriers contribute to worsening their burden of treatment, defined as the impact of everything they have to do to care for themselves on their quality of life and well-being.4–6 It is critical for health professionals to consider PLWH’s burden of treatment. Indeed, whenever patients’ healthcare tasks compete with other meaningful life demands, patients weigh the expected benefits of pursuing the healthcare against the associated burden of treatment and may intentionally decide not to adhere to care.1 5 7–9 This could lead to viral resistance to antiretroviral therapy (ART),4 10 11 virological failure,12 13 risk for others and increased mortality.
Regardless, patients’ burden of treatment is often underappreciated by health professionals,14 15 whose views, objectives and priorities sometimes conflict with those of patients.16 There is a sharp contrast between the number of interventions designed to improve patients’ retention in care, adherence to therapy and/or quality of life in sub-Saharan Africa (eg, task shifting, home-based services, patient reminders by text messages),17–19 the growing consensus on the importance of leveraging patients’ experiences to improve the quality of care, and the lack of evidence on how patients expect their care to be shaped. Until today, only few studies have explored patients’ ideas to improve their own care. However, these studies focused on patients’ ideas to improve their consultations in Western countries and thus could not be generalised to the sub-Saharan African context.20–22
In this study, we used a qualitative approach to explore PLWH’s propositions for decreasing their burden of treatment and to examine to what extent these ideas could be implemented in care.
Methods
Participants
We invited all patients from the ANRS 12365 MOTUHS-BOT project,4 a cross-sectional study describing the workload of care for PLWH in sub-Saharan Africa, to share their ideas on how to decrease their burden of treatment during a qualitative study. Participants from the MOTUHS-BOT project were consecutive adults (age >18 years old), under ART treatment for at least 1 year, who attended consultation in three care centres in two districts (Treichville and Yopougon) of Abidjan, Côte d’Ivoire. All patients provided written informed consent before participating in the study.
Data collection
Data collection was in two parts. First, patients provided some clinical and demographic information and completed the Treatment Burden Questionnaire (TBQ).15 The TBQ is a validated instrument of 15 items with scores ranging from 0 (not a problem) to 10 (big problem) assessing the burden associated with medication management, self-monitoring, exams, doctor visits, need for organisation, administrative tasks, diet, physical activity and social impact of the treatment.
Second, patients participated in face-to-face semistructured interviews. To avoid imposing on participants any preconceived ideas or themes, all interviews started with the same non-leading question: ‘What do you believe are the most important things to change in your care to improve your burden of treatment?’ If necessary, interviewers (two research associates with experience in qualitative research methods) rephrased the open-ended question to ensure that patients understood the purpose and objective of the study. However, interviewers were encouraged not to guide the patient into specific themes with examples. To put patients’ answers into context, interviewers usually asked them about their perspectives of their burden of treatment, examples of recent burdens they might have experienced or the reasons underlying their propositions, although no specific question or thematic was imposed.
The feasibility of our interviews was assessed during face-to-face cognitive interviews with 11 patients. These interviews allowed us to ascertain the comprehensibility of the starting question and the usability of possible reformulations and explanations. To avoid patients’ concerns about interview recording (mistrust towards the object and/or the interviewer), which may have affected the feasibility of our study, we chose not to record interviews. Instead, notes were taken during the interviews. These notes took the form of both verbatim patient comments and interviewer’s interpretations of participants’ words. These two types of data were clearly distinguished in the notes. At the end of the interview, all notes were read to participants and discussed with them to avoid any discrepancy between what was meant by the patient and what was understood and transcribed by the interviewer.
Analysis
Qualitative analysis of patients’ propositions to decrease their burden of treatment
Qualitative data were analysed by thematic analysis. Two investigators (VTT and AA) independently read all participants’ notes taken during interviews to extract patients’ propositions to decrease their burden of treatment. In this study, the burden of treatment was defined as the workload of healthcare and how it affects patients’ functioning and well-being.6 23 To operationalise this definition, we considered as propositions to decrease the burden of treatment all explicit statements of actions (1) that patients believed could improve their lives; (2) that could be related to health or care (eg, we excluded propositions such as ‘I wish I had my own shop’); and (3) did not directly relate to their condition or symptoms (eg, we excluded propositions such as ‘I wish I had less pain’). Propositions related to ‘I want that people find a cure for HIV’ were dropped from the analysis. In addition, we extrapolated patients’ statements of experienced burden of treatment into propositions (‘There are too many visits’ was classified as ‘I wish there were less visits’). Then, the two investigators independently grouped identified propositions for similarity. For example, ‘Medication refills should be every 3 or 6 months’ and ‘I’d like less frequent visits so that I could travel’ were grouped under the proposition ‘Longer visit/refill intervals’. During meetings, the investigators compared their findings and reached consensus to create a taxonomy of participants’ propositions. Consensus was informed by the investigators’ previous works on the burden of treatment and their clinical experience.4 5 Finally, one investigator (VTT) reread participants’ contributions to assess consistency with the defined taxonomy.
A mathematical model, developed for surveys involving open-ended questions,24 was used to ensure that most of patients’ ideas to improve their care had been elicited and that data saturation was reached. This model uses the data collected by the first participants in a qualitative study to infer the total number of themes (here propositions) that may be found in the study.24 Analyses involved use of R V.3.3 (http://www.R-project.org, the R Foundation for Statistical Computing, Vienna, Austria).
Assessment of the feasibility of patients’ propositions
A group of six experts independently evaluated all propositions from patients. The expert group aimed to represent all different stakeholders involved in the improvement of HIV care, with each person involved providing a specific expertise on possible changes at a consultation level, at organisational level or a health system level. The group included the director of a large HIV clinic in West Africa, a professor in Public Health in sub-Saharan Africa, a decision maker from the Global Fund Coordinating Mechanism in Côte d’Ivoire, a physician with experience in clinical research, a social worker and a patient from the association ‘Réseau Ivoirien des Personnes Infectées par le VIH’. Members’ qualifications are described in online supplementary appendix 1. During individual in-person meetings, an investigator (VTT) presented to each expert all patient propositions, each illustrated with selected examples. Experts were asked to classify them as ‘Very difficult and/or costly to implement’, ‘May be possible to implement but not without costs or effort’ or ‘Easy to implement at low cost’. We defined the propositions’ global feasibility by considering the most answered option. If an equal number of experts gave different options, we considered the global feasibility as the least feasible option. To further describe the consensus between experts, we calculated the number of propositions for which four of six experts agreed on their feasibility assessment.
Supplementary file 1
Results
Among the 476 patients who participated in the MOTHUS-BOT project, we recruited 326 (230 (70.5%) female) between February and April 2017 for this study (response rate: 68.5%; 110 were unreachable because they had changed their telephone contact, 24 were unavailable, 15 refused to participate and 1 died). Mean age was 45.1 years (SD=9.4) (table 1). Participants were receiving ART for a mean of 7.4 years (SD=3.6). A total of 283 (87%) participants had an HIV-1 viral load <100 cp/mL and were considered virologically suppressed. One-third of patients (n=120, 36.8%) reported at least one other chronic condition not related to HIV, such as gastric ulcer or gastro-oesophageal reflux disease (n=48), high blood pressure (n=20) or diabetes (n=8). Sex ratio, duration of ART treatment and CD4 count at initiation were globally similar to those from large HIV registries in sub-Saharan Africa.25 Respondents and non-respondents differed only in ART duration (mean 7.4 (SD=3.6) vs 6.6 (SD=3.5) years, p=0.02). Details are in online supplementary appendix 2.
Characteristics of participants (n=326)
In our sample, mean score on the TBQ was 33.3 (SD=19.6), which indicates a medium burden of treatment.15 The three areas most frequently reported as a burden for participants were (1) the financial burden of treatment, (2) the number of and time spent in doctor visits and (3) the fact that medical healthcare on a regular basis reminded patients of their condition.
Qualitative analysis of patients’ propositions to decrease their burden of treatment
Patients’ answers represented a total of 748 quotes on how their burden of treatment could be mitigated, which were further grouped into 59 unique patient propositions related to (1) their personal care, (2) improving the clinic organisation and (3) improving the health system (figure 1). Using mathematical modelling, we estimated that 91% (95% CI 89% to 92%) of potential unique propositions had been identified.

Patients’ propositions to improve their burden of treatment and their feasibility according to experts. ART, antiretroviral therapy.
Propositions involving personal care
Changes in the pharmacological treatment
Overall, 127 (39%) participants asked for at least one change to their pharmacological treatment to alleviate their burden of treatment (change their regimen with smaller pills, pills with a better taste, medications requiring a less strict dosage schedule, and so on). The most frequent request (n=58; 18%) was to reduce the number of pills per day: ‘I’m tired to have to ingest so many pills per day. I’ve taken too many medications for the last seven years’ (59-year-old man taking five pills per day).
Changes in the tests and visits schedule
A total of 53 (16%) participants suggested at least one change in their tests and visits schedule, because frequently imposed health-related activities required them to take days off work or limited their travels. For example, patients suggested longer visit intervals for patients with stable disease (n=44, 13%), leaving the choice of date of visits and tests to patients, or implementing a system to enable patients to obtain refills without having to visit their doctors: ‘If tests are OK, I’d like to go less frequently to the hospital’ (47-year-old man with a median visit rhythm of 90 days).
Changes in the consultation content
In all, 35 (11%) participants considered that at least one change in the consultation content would lighten their burden of treatment. Most patients believed that clinicians could and should provide more information on their care, the likely evolution of the condition, the risks of transmission and/or adverse effects of treatments. Four patients wished for a more supportive attitude from health professionals (n=4). Finally, two patients asked for more involvement in therapeutic decisions as a way to improve the quality of care.
Propositions involving the local organisation of care
Structural improvements for clinics and hospitals
In our sample, 104 (32%) participants suggested at least one structural change in their clinic or hospital to smooth the movement of the patient through the structure and reduce waiting times (n=82, 25%). For example, ‘Pharmacy is the slowest service. I’d wish that there were two cash desks (to improve the flow of patients)’ (42-year-old woman who reported spending a mean of 9 hours/month in waiting rooms) or ‘Why don’t you implement specific consultation hours for patients who are stable and well and only come for medication refills? Everything would be faster’ (51-year-old woman who reported spending a mean of 1 hour/month in waiting rooms). If faster service was not possible, patients proposed solutions to ease their lives during waiting times such as more seats in waiting rooms (n=1) or food distribution (n=14).
Propositions for more interaction between patients
Seven participants (2%) proposed to create formalised groups to meet and discuss with other patients (n=6) to share their tips and methods to live with the disease and its care. One patient wished that older and more expert patients could share their experiences with newly diagnosed ones to reduce their burden of treatment. For example, ‘I’d like to meet with other patients to talk about my condition’ (36-year-old woman living with two other people).
New services that could be offered by clinics
Six participants (2%) asked for new services in their clinics, such as having refills sent to their homes, allowing their families to consult in HIV clinics for general healthcare, or improving the continuity of care with 7/7 medical permanencies in HIV clinics, for instance. For example, ‘I’d like all clinics call me or text me the day before appointments, so that it is easier to remember’ (44-year-old woman with two chronic conditions other than HIV).
Propositions involving health system changes
Reduction of the fragmentation of care
Eleven participants (3.3%) proposed changes in the coordination between the multiple care structures to reduce fragmentation, such as the creation of integrated structures involving doctors from different specialties for less geographic fragmentation of care (n=6) or the implementation of methods for better communication between doctors (systematic doctor letters, shared electronic health records, and so on) (n=5). For example, ‘I wish that [HIV] clinics had all [specialist] doctors in only one place. For example, I have to see the ophthalmologist in another hospital’ (45-year-old man who regularly visited three different doctors).
Social help
In our sample, 62 (19%) participants proposed the creation of social measures to help them maintain their family and professional lives, such as financial aids (n=40), specific job opportunities for patients with HIV (n=22), or help for one of their informal caregivers (n=3). For example, ‘They [the government] should help my daughter since I’m ill, she can’t work anymore’ (63-year-old woman with monthly household income of US$<99 per month).
Reimbursement of health expenses
In all, 115 (35%) participants proposed reimbursement for transportation fees (n=52), visits and tests (n=68) or non-ART drugs (n=32) to ease their burden of treatment. Indeed, in Côte d’Ivoire, ART and CD4 count tests are free of charge,26 27 but patients still need to pay for other medications, tests, visits and transportation. For example, ‘I’d like a financial help to pay for the tests. I can’t afford the scan [computed tomography] asked by the doctors. They asked it for a long time, but it is too expensive. At the university hospital, it costs 117 US dollars’ (50-year-old man with a monthly household income between US$99 and US$166 per month) or ‘Times are difficult. I’d like a reimbursement for transportation fees. If not, there is a risk I stop coming regularly to take the medications, because of the costs’ (36-year-old woman with monthly household income of US$99–US$166 per month). One patient proposed that health costs should be adapted to patients’ revenue.
Other changes at the health system level
Finally, 30 (9%) participants suggested at least one other change to mitigate their burden of treatment. These changes involved the creation of more HIV clinics closer to their homes and ones that were less crowded (n=4), performing research more focused on their daily problems (n=1), keeping patients informed of research results on their condition (n=2), finding solutions to reduce drug shortages (which usually resulted in changes to their ART regimen) (n=6) and/or improving the public’s understanding of HIV to reduce the stigma (n=12). For example, ‘I want to stop hiding when I’m going to the (HIV) clinic. I want more awareness campaigns so that patients would no longer be alienated’ (45-year-old woman).
Assessment of the feasibility of propositions
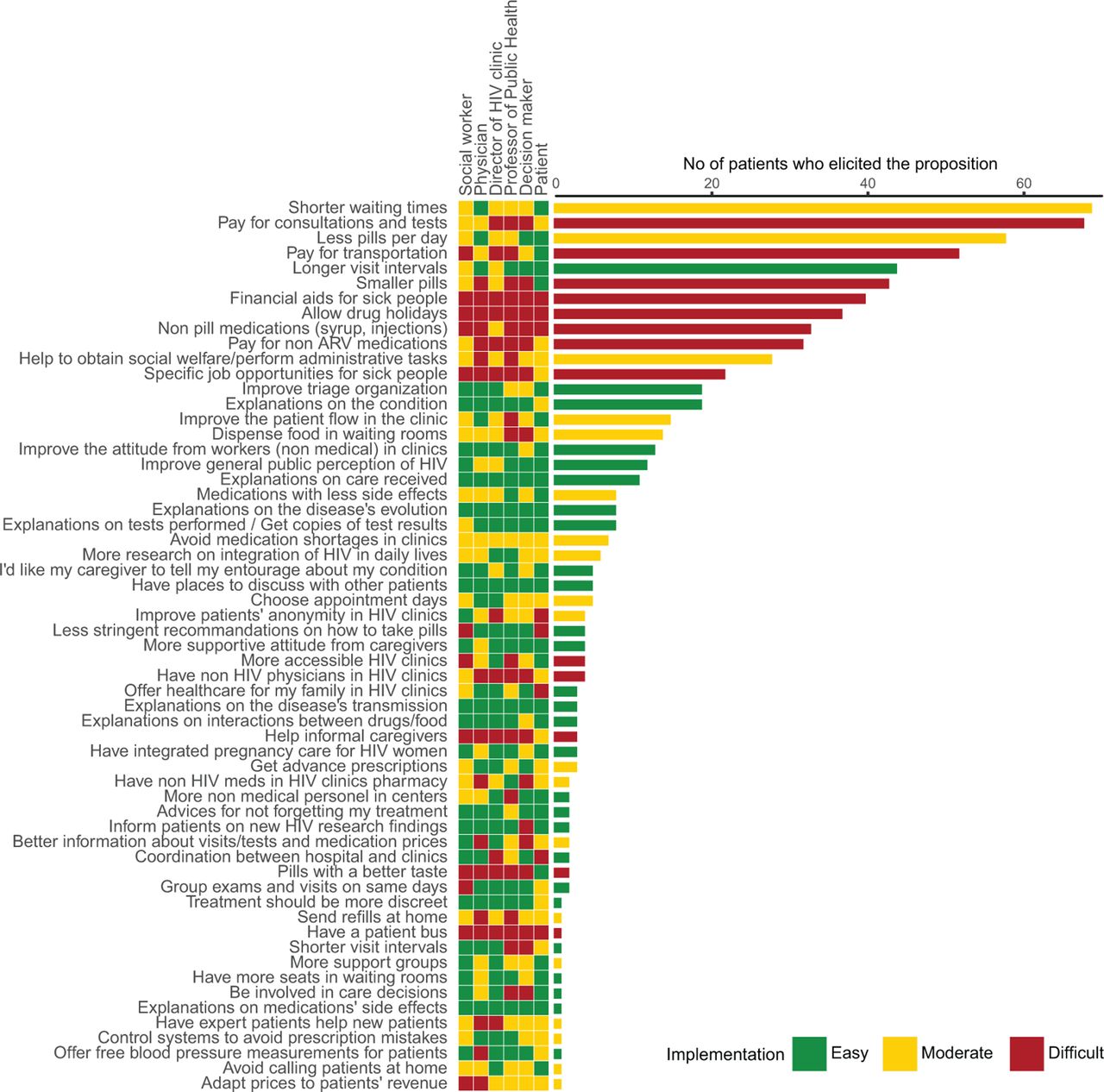
Among the 59 unique propositions, our expert panel considered that 27 (180 patient quotes), 19 (227 patient quotes) and 13 (341 patient quotes) were easy, moderate and difficult to implement, respectively (figure 2). Expert opinions were globally concordant because for 41 (70%) propositions, at least four of six experts agreed on the feasibility assessment.

{kind=link}
{kind=link}
Number of occurrences of each patient proposition to decrease their burden of treatment (histogram) and expert assessments of the feasibility of propositions (heatmap). ARV, antiretrovirals.
When asked about the most important things to do to mitigate their burden of treatment, 118 (36%) participants offered at least one proposition considered easily implementable by our experts. For 13 propositions, experts strongly agreed (≥5/6 experts) that implementation would be easy and low cost. These propositions were related to (1) systematically sharing test results with patients (one proposition); (2) implementing places of exchange for patients to share their care experiences (one proposition); (3) providing patients with more explanations on the condition or treatment (eight propositions); (4) providing patients with more information on HIV research results (one proposition); (5) supporting what patients were doing right rather than criticising their failures (one proposition); and (6) loosening the specific precautions of drug intakes (one proposition). These 13 easily feasible propositions were elicited by a total of 54 (16%) participants (box 1).
Patient propositions to decrease their burden of treatment for which experts strongly agreed that implementation would be easy and at low cost (ie, all or five of six experts deemed the proposition easy to implement)
Patient propositions that could be easily implemented in care:
Health professionals should provide more explanations on my condition.
Non-medical workers should have a better attitude towards patients.
Health professionals should provide more explanations on the care received.
Health professionals should provide more explanations on the disease evolution.
Patients should systematically get copies of test results.
Implementation of places for patients to discuss and share their experiences.
Health professionals should support what patients are doing right rather than criticise their failures.
Health professionals should provide more explanations on the disease transmission.
Health professionals should provide more explanations on interactions between drugs/food.
Health professionals should provide advices on methods not to forget taking medications.
Patients should be informed of the results of HIV research (and especially those they participated in).
Adaptation of the specific time and precautions of drug intakes so that it would be easier to hide them.
Health professionals should provide more explanations on my treatment side effects.
Propositions involving personal care
Propositions involving personal care were globally considered easy to implement, with 67%, 17% and 17% of propositions considered easy, moderate and difficult to implement, respectively, by experts. Four of seven propositions to change patients’ treatment regimens were considered difficult to implement because they could be considered only on a patient-by-patient basis. Changes in visit intervals and grouping of visits and tests on the same days were considered easily feasible at low cost. However, experts’ views were divided on advance prescriptions and allowing patients to choose their appointment days. All patient propositions (11/11) related to changes in the consultation content were considered easy to implement.
Propositions involving the local organisation of care
Propositions involving changes in the local organisation of care were globally considered moderately difficult to implement, with 37%, 58% and 5% of propositions considered easy, moderate and difficult to implement, respectively, by experts.
Propositions involving health system changes
Propositions involving changes in the health system were globally considered difficult to implement, with 25%, 25% and 50% of propositions considered easy, moderate and difficult to implement, respectively, by experts. Especially, six of eight propositions regarding reimbursement of care and specific social help for PLWH were considered nearly impossible to implement.
Discussion
Statement of principal findings
In this study, we revealed unique propositions by PLWH in sub-Saharan Africa to decrease their burden of treatment and the feasibility of the propositions. Slightly less than half of these propositions were considered easy to implement at low cost by experts, and 22% were considered difficult and/or costly to implement.
Our study highlights the universal nature of the concept of burden of treatment. Regardless of their country of residence, patients with chronic conditions may experience complex, fragmented and uncompassionate care. Indeed, issues pointed out by patients in our study were the same as those described by patients in richer Western countries.5 However, in low/middle-income countries, the impact of these issues on patients’ lives may greatly differ in magnitude. As an example, the financial burden of treatment affects many patients throughout the world,28 but in African contexts, it may be unbearable. In Côte d’Ivoire, more than 12% of PLWH face ‘catastrophic’ health expenditures (≥40% of the household’s capacity to pay) that may put their household in peril.27 Nonetheless, PLWH in our study did not solely focus on reducing care costs. They also elicited a wide range of propositions illustrating the complexity of their issues, expectations and goals.29 We identified 13 propositions that were consensually considered easy to implement at low cost by experts. Their implementation could potentially lead to improved quality of care for PLWH without important investment of additional resources.
Our study demonstrates that PLWH in sub-Saharan Africa are ready to partner with health professionals to provide ideas to transform their healthcare environment. The diversity of patients’ propositions also underlined the absence of a ‘one-size-fits-all’ approach to solve the burden of treatment and the need for tailored care fit to each patient’s context.
Strengths and weaknesses of the study
To our knowledge, this is the first study to systematically ask PLWH their ideas and propositions to improve their experiences. Using a combination of a qualitative survey and methods to estimate point of data saturation, we were able to describe the diversity of patients’ ideas in a broad population of PLWH seeking care in various health settings in a large urban city in sub-Saharan Africa and ascertain that most of potential patients’ ideas had been covered.
This study has some limitations. First, the number of times an idea appeared in our data must be generalised with caution. Indeed, this figure depended on the fact that patients elicited the idea. As an example, patients could have endorsed propositions from other participants but not expressed them during interviews. Frequently elicited ideas are not necessarily those most ‘desired’ by participants but those that are the most evident to them. Nonetheless, our study provides an overview of both the diversity of patients’ propositions and of what comes first to mind for patients when asked about how to improve their care. Second, our study was conducted in three centres, all located in the same city in Côte d’Ivoire. This situation affects the transferability of both propositions and their feasibility in other settings. Especially, generalisation should be careful in rural contexts or in other sub-Saharan countries where health and care systems could be organised differently. Third, assessment of the point of data saturation in our study was guided by the use of a mathematical model developed in surveys involving open-ended questions. This model uses the data collected by the first participants to infer the total number of themes that may be found in the study. This method may improve the transparency and credibility of statements indicating that data saturation was reached. Regardless, we used the model in a context different from the one in which it was created and validated. We believe that such extrapolation was acceptable because all hypotheses of the model were respected in our study (finite number of themes; no change in the coding granularity and independence of themes).24 Finally, we defined a global feasibility variable from the different expert opinions, which did not take into account the different expertise of respondents. For example, the director and health professionals working in an HIV clinic may be in a better position to judge the feasibility of propositions involving the reorganisation of the clinic. Regardless, we opted not to seek consensus among experts because of hierarchical relationships that could exist between them and the strong influence of leaders’ opinions in African culture, which would have biased their opinions. In addition, subjective assessments of the potential costs and feasibility of patients’ ideas may not reflect their actual costs. Evaluations from experts may be strongly influenced by their context and setting. Thus, careful evaluation of the efficacy, safety and cost-effectiveness of all interventions arising from patients’ ideas should be undertaken before implementation in practice.
Difference with other studies
It is usual for care organisations to assess patients’ experiences with some feedback surveys. Numerous data collection methods have been used for this, from multiple-choice questionnaires, to narratives, to the use of tweets or Facebook comments. However, as pointed out by Coulter et al, ‘stories trump data for capturing the interest of staff (…) and help them view their services through patients’ eyes.’30 With open-ended questions, patients’ feedback comments are not generic items thought of by people who designed the survey but rather real stories adapted to their context. These stories make more sense to stakeholders involved in improving the quality of healthcare. In addition, our study went beyond the patient feedback survey. Indeed, patients proposed ideas to improve their care rather than commenting on what they found adequate or not in their care. This participatory approach emphasised that patients are experts of their own care. They know very well the bottlenecks of the system in which they seek care. This empowerment might also be a powerful tool to increase patients’ motivation in care. In addition, inviting health professionals and decision makers to assess the feasibility of patients’ propositions might reinforce their awareness of potential problems and solutions to improve care. This does not mean that all suggestions from patients should be implemented in care: rigorous evaluation of their efficacy, potential drawbacks, unintended consequences and cost-effectiveness are still required. Rather, the participative research model we propose is intended to identify ‘out-of-the-box’ ideas from patients, which may be adapted and refined into implementable and assessable interventions.
In the literature, patient involvement in care is often a synonym for empowering patients to make informed decisions about their care and treatment.31 In this regard, we showed that expectations from PLWH in sub-Saharan Africa to improve their personal care were very similar to those collected in studies conducted in Western countries.20 32 However, our study also went further than previous works by describing patients’ suggestions to tackle structural and systemic problems they encountered in their care. This approach was similar to that of a recent study by Berwick et al, asking patients, their entourage and clinicians from North American hospitals ‘If you could break or change any rule in service of a better care experience for patients or staff, what would it be?’33 Again, despite the stark difference in contexts, we highlight that patients in sub-Saharan Africa and those in North America share common burdens and strive for common goals. Tailored care fit for patients’ contexts should not be limited to patients in rich Western countries. For those living in resource-limited countries, the competition between living their lives and the demands from a healthcare system with scarce resources can be daunting,1 and so a minimally disruptive medicine approach is even more necessary.34
Implications for patients, clinicians and policymakers
Empowering patients to participate in the improvement of their own healthcare management contributed to identifying potential solutions to problems patients encountered in their care, of which some solutions seemed feasible. The untapped resource of patients’ knowledge and experience can improve the quality of care, and physicians should be encouraged to ask their patients about their problems and suggestions for better care.
Beyond our results, this study provided a proof of concept for a method to involve patients in improving their quality of care, which could be replicated in different settings and contexts. This method could help decision makers evaluate which interventions to implement by providing information on desired changes and their feasibility. We believe that these studies could be replicated locally to guide discussions on how to improve local care organisations and that pooling multiple similar studies could inform and serve as a framework for changes at the larger level. Such process would help in moving from a paternalistic approach of care, where power is mainly owned by physicians, to a more democratised system recognising the value and expertise of patients in their care.35 However, it also challenges traditional patient–provider hierarchies. To mitigate potential resistance from care providers to this ‘loss of power’, the contours of each stakeholder’s ‘power’ must be clearly defined in the processes to improve the quality improvement of care. Patients have a role in generating ideas, from their daily experience and observations with the condition and treatment, whereas care professionals and decision makers contribute by moderating these ideas in terms of their feasibility, cost, potential benefit or harm.
Finally, our results call for new research and care for HIV and the need to move beyond the concept of viral suppression, still considered the central indicator for quality of HIV care.29 Despite having achieved viral suppression, half of the PLWH in our study reported a high burden of treatment and all expected improvements in their care. As of today, HIV care and research in sub-Saharan Africa is still centred on the disease rather than the needs of individuals and communities. It is necessary to listen to patients to create meaningful kind and careful patient-centred care.
Conclusion
Asking PLWH in sub-Saharan Africa about how their care could be improved helped identify meaningful propositions. According to experts, half of the propositions could be easily implemented with low cost. Listening to patients and involving them in improving their care opens the path for minimally disruptive HIV care, which has the potential to improve patients’ retention in care, adherence to therapy and quality of life.
Acknowledgments
The authors thank MelianeLorng and Daniel Balfong for data collection; Jean Baptiste N’takpe, Jean MarieMasumbuko (The Global Fund to Fight AIDS, Tuberculosis and Malaria), SuzanneKouadio and Sidjé Léontine Gaty (RéseauIvoirien des Personnes Infectées par le VIH) for their participation in theexpert group; Laura Smales(BioMedEditing) for editing; and the French National Agency for Research on HIVand viral hepatitis (Agence Nationale de Recherche sur le Sida et les HépatitesVirales – ANRS) for logistic support.
References
Footnotes
Contributors Generated the idea: VTT. Conceived and designed the study: VTT, EM, MMD, PR and DKE. Collected the data: Meliane Lorng and Daniel Balfong under the supervision of VTT and EM. Analysed the data: VTT, Alexandra Anderson. Wrote the first draft of the manuscript: VTT and PR. Contributed to the writing of the manuscript: VTT, PR and DKE. ICMJE criteria for authorship read and met: VTT, EM, MMD, PR and DKE. Agree with manuscript results and conclusions: VTT, EM, MMD, PR and DKE. DKE is the guarantor, had full access to the data in the study, and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Funding This work was supported by the French National Agency for Research on HIV and Viral Hepatitis (Agence Nationale de Recherche sur le Sida et les Hépatites Virales–ANRS) (Grant No 12365) and the "Fondation pour la Recherche Médicale" (Grant No 40284).
Disclaimer The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Competing interests None declared.
Patient consent Obtained.
Ethics approval National Ethics Committee from the Ministry of Health of Côte d’Ivoire.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data from the study are available upon request to the authors.