Differences in mortality after fracture of hip: the East Anglian audit
BMJ 1995; 310 doi: https://doi.org/10.1136/bmj.310.6984.904 (Published 08 April 1995) Cite this as: BMJ 1995;310:904
- C J Todd, senior research associatea,
- C J Freeman, research/audit assistantb,
- C Camilleri-Ferrante, consultant in public health medicineb,
- C R Palmer, medical statisticiana,
- A Hyder, research/audit assistantb,
- C E Laxton, senior registrarb,
- M J Parker, research registrarc,
- B V Payne, consultant in medicine for the elderlyd,
- N Rushton, consultant orthopaedic surgeone
- a Health Services Research Group, Department of Community Medicine, Institute of Public Health, University of Cambridge, Cambridge CB2 2SR
- b Directorate of Public Health Medicine, Anglia and Oxford Regional Health Authority, Cambridge
- c Department of Orthopaedics, Peterborough District Hospital, Peterborough
- d Norfolk and Norwich Healthcare NHS Trust, Norwich
- e Orthopaedic Research Unit, University of Cambridge Clinical School, Addenbrooke's Hospital, Cambridge
- Correspondence to: Dr Todd.
- Accepted 17 February 1995
Abstract
Objective: To investigate differences between hospitals in clinical management of patients admitted with fractured hip and to relate these to mortality at 90 days.
Design: A prospective audit of process and outcome of care based on interviews with patients, abstraction from records with standard proforma, and follow up at three months. Data were analysed with {chi}2 test and forward stepwise regression modelling of mortality.
Setting: All eight hospitals in East Anglia with trauma orthopaedic departments.
Patients: 580 consecutive patients admitted for fracture of neck of femur.
Main outcome measure: Mortality at 90 days.
Results: Patients admitted to each hospital were similar with respect to age, sex, pre-existing illnesses, and activities of daily living before fracture. In all, 560 (97%) were treated surgically, by a range of grades of surgeon. Two hundred and sixty one patients (45%; range between hospitals 10-91%) received pharmaceutical thromboembolic prophylaxis, 502 (93%; 81-99%) perioperative antibiotic prophylaxis. The incidence of fatal pulmonary emboli differed between patients who received and those who did not receive prophylaxis against deep vein thrombosis (P=0.001). Mortality at 90 days was 18%, differing significantly between hospitals (5-24%). One hospital had significantly better survival than the others (odds ratio 0.14; 95% confidence interval 0.04-0.48; P-0.0016).
Conclusions: No single factor or aspect of practice accounted for this protective effect. Lower mortality may be associated with the cumulative effects of several aspects of the organisation of treatment and the management of fracture of the hip, including thromboembolic pharmaceutical prophylaxis, antibiotic prophylaxis, and early mobilisation.
Key messages
Key messages
Being older, having a poorer level of activities of daily living, being male, and having a history of cardiovascular disease were important determinants of death
One of the hospitals had a much higher survival rate. This seemed to be due to an aggregate effect of the total package of care
Routine thromboembolic prophylaxis is indicated for patients with fractured hip
Written policies that include prophylaxis should be developed and implemented for this vulnerable group of patients if mortality is to be improved
Introduction
In the financial year 1990-1, 55748 people were admitted to hospital with a fracture of the neck of femur in England.1 The incidence of such fractures has been increasing for several years and is predicted to continue to increase.2 Fractures of the hip affect primarily women aged 65 years and over. Preferred treatment is normally surgical correction.3 Patients with a hip fracture occupy about 20% of orthopaedic beds in England and Wales, and the average length of stay is 30 days.2 Mortality at one year after fracture is 12-20% above that expected for the age-sex group, and most of this excess occurs within the first four months. Many survivors never regain their previous level of physical function.4 Also, many patients receive less than optimal treatment.5 Fractures of the hip will continue to be a major burden on orthopaedic services well into the next century,6 so the effective use of resources, while maintaining or improving quality, will be a central concern for both purchasers and providers of health care.
Recently, improvement of patient care through clinical audit has gained considerable attention. Clinical audit has been described as a “systematic, critical analysis of the quality of medical care, including the procedures used for diagnosis and treatment, the use of resources and the resulting outcome for the patient.”7 Audit should whenever possible monitor patient outcomes as well as medical process.8 Although process audit is quite common, relating process to patient outcome is more unusual. We conducted a prospective audit in hospitals throughout East Anglia, focusing on the relation between processes of care for fractures of the hip and patient outcomes. Indicators were chosen from recommendations resulting from a regional consensus conference,9 published material,2 and interviews with 22 orthopaedic consultants in the hospitals in which the audit was to be conducted. On this basis we agreed that the following represent good practice: multidisciplinary management of patients; preoperative assessment of health and social circumstances; postoperative planning within four days; early mobilisation; prophylactic measures against venous thromboembolism; giving prophylactic antibiotics; and assessment of outcomes such as mortality and mobility. While other findings are reported elsewhere,10 this paper considers the relation between aspects of treatment received by patients and mortality.
Subjects and methods
The study sample comprised a consecutive series of patients admitted for fractured neck of femur (International Classification of Diseases, ninth revision, code 820) to each of eight hospitals throughout the former East Anglian Regional Health Authority that had a trauma orthopaedic department. To obtain a large enough sample to permit not only interhospital analysis (the central aim of the study) but also intrahospital comparisons of important variables, we estimated that we needed to recruit 80 consecutive patients from each hospital.11 For ease of identification and to maintain anonymity, hospitals are numbered 1 to 8.
We interviewed patients as soon as possible after admission about their residential status, social status (marital state, living arrangements), activities of daily living, and home support before their injury. We recorded processes of care on a standard proforma from medical and nursing records. This proforma had been developed on the basis of other work by members of the audit group12 and piloted in two hospitals before the audit began. Our primary source for information about process was the clinical records. When possible, we checked data by cross referencing records—that is, nursing, theatre, and medical notes—and more importantly against other information (for example, by asking nursing staff or the patient). We followed up patients (usually by telephone) at 30 days to assess satisfaction with services and at 90 days to assess activities of daily living, pain, social support (use of health and social services, support from family and neighbours, etc), and residential status. Mortality data were obtained from hospital records and from the information gained at the 90 day follow ups. Cognitive function is often considered an important determinant of mortality among patients with a fractured hip, but it was not viable to collect such data in this audit. Recent work suggests, however, that a simple mobility score can have a better predictive value than mental state,13 and these data were routinely collected.
Statistical analysis was conducted with SPSS for Windows Version 6.0. {chi}2 Tests reported below have one degree of freedom and use Yates's correction unless stated otherwise. Survival curves were produced with Kaplan-Meier estimates. We built a model of mortality on the basis of patient characteristics using forward stepwise logistic regression, with response being 90 day survival.
Results
Duration of recruitment, which began in all hospitals on the same day, ranged from 56 days to 131 days (mean 98.7) for seven hospitals. For the remaining one (hospital 2) admission for fractured hip was very slow, and we curtailed recruitment from this hospital after 145 days with only 24 patients. Data from this hospital are included for completeness. We could not recruit exactly 80 patients from each of the other hospitals owing to classification error or admission from outside the region. In two hospitals (4 and 5) we recruited 80 valid patients, in three hospitals (1, 3, and 7) 79 patients, in one hospital (8) 78 patients, and in the remaining hospital (6) 81 patients.
PATIENT CHARACTERISTICS
Table I shows the characteristics of 580 consecutive patients admitted for hip fracture to the eight hospitals during the audit. The men were significantly younger (74.7 years) than the women (81.6) (t=6.48, P<0.001). No significant differences existed between hospitals in terms of patients' age, sex, source of admission, score for activities of daily living before injury, type of fracture, the number of concomitant illnesses from which patients suffered at admission, or delay in operating. We can therefore be reasonably confident that we are comparing similar populations of patients.
Characteristics of 580 patients admitted with fractured hip to eight hospitals in East Anglia. Values are numbers (percentages) unless stated otherwise
MANAGEMENT OF PATIENTS
In all, 560 (97%) patients were treated surgically; of the 553 patients who had surgery and for whom information was available, 308 (56%) had their operation within 24 hours of admission (table II). A clear clinical reason for delay was recorded in only 53 of the 245 operations delayed for more than 24 hours; in 192 cases (34% of all operations) the delay was not explained in clinical terms. A delay in surgery of more than 48 hours was associated with higher mortality ({chi}2=5.79, P=0.016). Data about type of fracture were missing for nine patients, but in 79% (190/239) of cases of extracapsular fractures treatment was with dynamic hip screw, and of the 332 cases of intracapsular fractures treatment was mainly with hemiarthroplasty (227 (69%)) or with multiple screws (57 (17%)). Of the 556 operations for which information was available, 144 were performed by a consultant orthopaedic surgeon, 159 by a senior registrar, 145 by a registrar, 85 by a senior house officer, and 23 by another grade of surgeon (for example, associate specialist). Significant differences existed between hospitals in the grade of staff performing operations: all operations in hospital 2 were performed by a consultant compared with none in hospitals 1 and 6 ({chi}2=331.6, df=21, P<0.0001). No association existed between grade of surgeon and mortality ({chi}2=1.51, df=3, P=0.68). Of the 553 patients who underwent surgery and for whom information was available, 327 (59%) received a general anaesthetic and 226 (41%) spinal anaesthesia (table II), but mortality did not differ between these two groups ({chi}2=0.71, P=0.40).
Process information on 580 patients admitted with fractured hip for each hospital and overall. Values are numbers (percentages) of patients unless stated otherwise
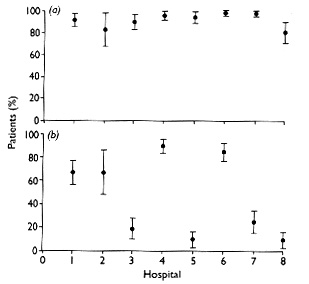
While most patients received prophylactic antibiotics, the use of pharmaceutical anticoagulant prophylaxis was more variable (table II; fig 1). In four hospitals (3, 5, 7, and 8) pharmaceutical anticoagulant prophylaxis was not routinely used. Mobilisation also differed. In hospital 6, 50% of the patients were mobilised on day 1 postoperatively; this level of mobilisation was not reached until day 2 in hospitals 2, 3, 4, 5, and 7 and day 3 or later in hospitals 1 and 8 ({chi}2=75.4, df=14, P<0.00001).

Percentages (with 95% confidence intervals) of patients admitted to each hospital with fractured hip who received (a) prophylactic antibiotics and (b) pharmaceutical anticoagulant prophylaxis
{kind=link}
PATIENT OUTCOMES
At 90 days, 468 of the 580 patients recruited were successfully interviewed (104 had died and eight were lost to follow up) (table III). In all, 15% (50/332) of the patients known to have intracapsular fracture and 22% (53/239) of those known to have extracapsular fractures had died before 90 days, a significant difference ({chi}2=4.29, P=0.038). No significant differences existed between hospitals in their rates of infection of hip joint, wound infection, pulmonary embolism, deep vein thrombosis, myocardial infarction, urinary tract infection, pneumonia, or revision of surgery (table III). The number of patients who were identified as having pressure sores was high at 129 (22%) (table III), and a wide and significant difference existed between hospitals ({chi}2=25.42, df=7, P=0.0006).
Outcomes of 580 patients admitted to hospital for fractured hip. Values are numbers (percentages) of patients
Postoperative thrombosis was diagnosed in 7% (22/305) of the patients who did not receive thromboembolic prophylaxis and in 3% (9/261) of the patients who received pharmaceutical antithrombotic prophylaxis ({chi}2=3.16, P=0.076). Although few patients were identified at postmortem examination as having had a fatal pulmonary embolism, whether the patient had received prophylactic treatment was highly significant. None of the 261 patients who received prophylactic antithrombotic treatment had a fatal pulmonary embolism. However, 4% (12/305) of those who did not receive prophylaxis against deep vein thrombosis had a fatal pulmonary embolism ({chi}2=8.68, P=0.003).
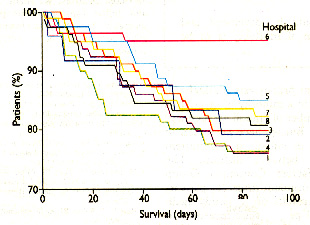
Figure 2 presents the survival curves of patients up to 90 days for the eight hospitals separately. While most of the hospitals had 90 day survival rates of approximately 80% (overall 82%), the survival rate of hospital 6 was considerably higher at 95%. This result was then investigated more fully with forward stepwise regression modelling. Younger people tend to require greater trauma before a hip will fracture than older people so we excluded the younger patients from the statistical modelling as they might have skewed the results. Thus regression analysis was based on 547 patients who were over 50 (nine were excluded because of age) and for whom we had no missing data on the variables entered into the analysis.

90 Day survival curves for each hospital for patients who had surgery for fractured hip
{kind=link}
Table IV shows the final model based on patient characteristics from this analysis. Age, activities of daily living, sex, and presence of cardiovascular disease seemed to be important determinants of death. Hospital 6, as opposed to any other hospital, also entered this final model as an independent protective factor, even though we adjusted for the other variables. Being male increased the odds of death 2.9-fold, and each unit increase in age or poorer score on activities of daily living increased the risk of death marginally. Presence of cardiovascular disease approximately doubled the risk of death. Being admitted to hospital 6, however, had a sevenfold protective effect.
Final model of mortality from forward stepwise regression of predictors of survival at 90 days after hip fracture
Discussion
The patients sampled from each hospital did not differ significantly on the sociodemographic variables or clinical characteristics collected. Thus we are reasonably confident that differences observed in outcomes are a function of the treatment and not primarily dependent on confounding effects of preexisting differences between patient samples. Recruitment was contemporaneous in all hospitals and over a short enough period to ensure that seasonal effects were negligible. Moreover, multivariate modelling took into account important aspects of case mix. The most important finding of this study is the difference in mortality at 90 days depending on hospital of treatment.
What differed in hospital 6 to account for this better survival? Analysis revealed no single factor that accounts for the observed difference, but our audit suggests that it was the total package of care rather than any single variable. In hospital 6, patients were routinely treated by a designated multidisciplinary team for fracture of the hip, with early assessment and surgery, much of which was performed by one surgeon. Patients received prophylaxis routinely and were mobilised early, and plans for discharging a patient began almost immediately after surgery. While these factors individually do not account for the protective effect of being treated in this hospital, they and undoubtedly other factors in the overall care of these patients contribute to better patient outcome. Uncritical acceptance of the “advantages” of hospital 6 should, however, be avoided as random variation almost certainly plays some part in these findings.
One strength of audit is to highlight specific areas of care that need attention. Feedback to clinical staff and continued audit should help to bring about the necessary improvements. In this study the high rates overall of urinary tract infection, pneumonia, and pressure sores are noteworthy. Since the data were collected several initiatives have been implemented to improve these specific aspects of patient care. The input of nurses and other professionals allied to medicine is crucial, and these staff should participate more in audit. Audit methodology relies greatly on the accuracy of the record keeping of professional staff, and we have depended on clinical records to identify the treatment of our patient sample. Although this approach has proved feasible, it may not be ideal, and this must be borne in mind in interpreting the results.
PROPHYLAXIS
We defined prophylactic measures in terms of pharmacological measures only. Patients who did not receive anticoagulant drugs may well have been treated by a mechanical method. We did not differentiate between different pharmacological treatments; we simply recorded whether the patient's notes showed evidence of drug prophylaxis, but even this crude analysis seems sensitive to differences. It is striking that without differentiating between differing prophylactic regimens we still identified an overall effect of prophylaxis. This finding confirms the need for future research to identify the most effective prophylactic preparation for use with patients with fracture of the hip. None the less, the evidence from this study is strong enough for us to reiterate the recommendations of the Thrombolic Risk Factors Consensus Group that patients should (a) be assessed for clinical risk factors and overall risk of venous thromboembolism and (b) receive specific prophylaxis in addition to early mobilisation.14 Written policies that include guidelines on prophylaxis should be developed and implemented for this vulnerable group of patients if mortality is to improve. Such measures are now in train in the hospitals audited. This audit study was undertaken in the belief that clinical audit and confidentially collected data permit improvements in care. Because we guaranteed confidentiality, our orthopaedic colleagues let us examine the care provided and collect valid data. We are convinced that audits such as ours will permit more insight into the working of the NHS and facilitate improvement in care that is more patient oriented and meaningful than aggregate data such as those recently published allow.15
Although 93% of patients received antibiotic prophylaxis, the use of anticoagulant prophylactic drugs was much more variable, and only 46% of this series of patients were recorded as receiving thromboembolic prophylactic agents. Figure 1 suggests that a dichotomy exists in terms of hospital policies; half the hospitals used anticoagulant prophylaxis routinely (in nearly all cases), half only in a minority of cases. It is almost certain that the number of emboli we recorded represents underreporting. But we have no reason to believe that the reporting of emboli at postmortem examination was biased between districts. The Thromboembolic Risk Factors Consensus Group recommended use of anticoagulant drugs for patients with a fractured hip; the results of our study again confirm the importance of prophylactic measures to combat venous thromboembolism. Despite considerable evidence of its efficacy, treatment with anticoagulant drugs is by no means used routinely by surgeons throughout the United Kingdom.14 Risk of thromboembolism becomes appreciable for patients aged 40 or over, and patients with a fractured hip are at high risk: 40-80% will develop deep vein thrombosis, 10-30% proximal vein thrombosis, and 1-10% fatal pulmonary embolism if prophylactic measures are not taken.14
CONCLUSIONS
The present data, revealing the striking difference between hospitals in mortality after fracture of the hip, were collected with audit methodology. Thus these data generate a hypothesis rather than test a specific hypothesis. No single variable that we identified explains the protective effect of hospital 6, suggesting that it is an aggregative effect of the total package of care. Further work must be undertaken to identify more fully in what other ways, if any, treatment in hospital 6 differs and whether any specific components account for these clinically important differences.
This audit was funded by the East Anglian Regional Health Authority's clinical audit committee. We thank all the hospital staff who helped us in this work as well as the patients and their relatives. We thank Sue Jukes for secretarial help and Julian Lipscombe for preparing data and drawing diagrams. Approval was obtained from the relevant research ethics committees and all patients interviewed gave informed consent.