Article Text

Abstract
The microsystem is an organizing design construct in which social systems cut across traditional discipline boundaries. Because of its interdisciplinary focus, the clinical microsystem provides a conceptual and practical framework for simplifying complex organizations that deliver care. It also provides an important opportunity for organizational learning. Process mapping and microworld simulation may be especially useful for redesigning care around the microsystem concept. Process mapping, in which the core processes of the microsystem are delineated and assessed from the perspective of how the individual interacts with the system, is an important element of the continuous learning cycle of the microsystem and the healthcare organization. Microworld simulations are interactive computer based models that can be used as an experimental platform to test basic questions about decision making misperceptions, cause-effect inferences, and learning within the clinical microsystem. Together these tools offer the user and organization the ability to understand the complexity of healthcare systems and to facilitate the redesign of optimal outcomes.
- design
- clinical microsystems
- patient safety
- process mapping
- organizational learning
Statistics from Altmetric.com
Health care confronts a wide range of problems commonly associated with increasingly complex and dynamic systems. The dramatic rise of patient safety as a national healthcare policy issue has stimulated dialogue about systems redesign, culture change, and advancement of medical education. The Institute of Medicine (IOM) report To err is human estimated that $29 billion was spent on correcting clinical errors and adverse events.1 By the standards of other high hazard industries, the rate of preventable service failures in medicine is alarmingly high. Problems facing health care include stabilizing the economics of the healthcare facilities, sustaining responsible levels of growth and development, managing limited resources, designing and engineering solutions for a variety of problems, improving public health, and protecting the hospital environment. All these problems occur within the context of systems—economic systems, ecological systems, chemical and physical systems, human physiological systems, social systems, political systems, and so on.
As changes continue to challenge healthcare systems, developing solutions and formulating policies requires an understanding of the complex and dynamic nature of the relevant systems. Such an understanding has two critical aspects: (1) representation in meaningful and reliable ways of the complexities and dynamics of micro and macro systems in which challenging problems occur; and (2) development of proper support for people who must learn about and solve problems related to these systems. This paper addresses both these aspects with the overall purpose of better understanding the science of systems through the use of the microsystem as an organizing construct of human/social dynamics that can meet the representational, educational, and decision support challenges involved in health care.
While much has been written about the conceptual underpinnings of the microsystem2–5 and its application in specific clinical settings,6,7,8,9,10,11,12,13,14,15,16 the purpose of this paper is to explore the microsystem framework as a design concept, specifically the role of understanding core and supporting processes in design and redesign of clinical care.
OVERVIEW OF CLINICAL MICROSYSTEMS
Systems in general often bring up images of “well oiled machines”. However, healthcare systems are often cumbersome, unwieldy, unfriendly and opaque to its users—patients, physicians, nurses, and staff, and even its executive. Healthcare systems are best described as complex adaptive systems. As such, they are a collection of individuals who are free to act in ways that are not totally predictable. The organizational boundaries are “fuzzy” in that membership changes and providers can simultaneously be members of other systems. Furthermore, given the complexity of these systems, the actions of individuals are interconnected so that the actions of one changes the context for all the others.17,18 One organizational construct that helps to operationalize the concept of a complex adaptive system is the clinical microsystem.
Microsystems are groups of clinicians and staff working together with a shared clinical purpose to provide care for a population of patients.16,19,20 The essential elements of the microsystem include the patients, clinicians and support staff, information and information technology, and the care processes. The clinical purpose and its setting define the essential components of the microsystem, which include clinicians, patients, and support staff; information and technology; and specific care processes and behaviors that are required to provide care. Microsystems evolve over time, and they respond to the needs of their patients and providers as well as to external pressures such as regulatory requirements. They often co-exist with other microsystems within a larger (macro) organization such as a hospital. Previous research on clinical microsystems has identified 10 success factors (table 1).6,21 The microsystem concept is an organizational framework for providing and improving care by making explicit the “5 Ps”—purpose, patients, professionals, processes, and patterns (table 2).8 Excellent patient care is not provided by one person acting alone but is a byproduct of a team of providers working together to achieve a common goal. The 5Ps are a reminder of the essential elements of a well functioning microsystem and the interrelatedness of those elements in meeting the needs of the patient.8
Characteristics of high performing microsystems
The five essential goals (“5Ps”) of the microsystem
THEORETICAL FOUNDATIONS OF THE CLINICAL MICROSYSTEM
The microsystem concept is based on an understanding of systems theory, coupled with James Brian Quinn’s theory of a smallest replicable organizational unit of change.5,22 At the heart of the microsystem is the fact that humans have difficulty in understanding the complexities caused by the dynamic and systemic nature of certain problems.23–25 Even motivated and well educated providers often fail when confronted with complex problems that are within their capacity to solve but that are new and unlike the everyday problems they confront.25 When these problem solving failures are examined across disciplines and over a wide range of subjects, the evidence suggests that humans tend to focus on local aspects of a problem and do not easily grasp systemic and non-linear relationships among problem components, nor do they appreciate the delayed effects of their own decisions or those of other events within the problem situation.26 In short, many well educated leaders in positions of responsibility with regard to various complex dynamic feedback systems have not been trained to think systemically.27–29
FROM THEORY TO PRACTICE: DESIGNING AND REDESIGNING CARE AT THE MICROSYSTEM
It is necessary to have the means and methods to represent the complexities and dynamics of a system to support learning, problem solving, decision making, and policy formulation. A theory of systems is required that can be used to generate system models and representations at various levels of granularity. These simulations may include high level process maps of the core clinical care processes, as well as a detailed and formal representation of a complex system, so that a synthetic version of reality can be created in the form of an interactive simulation model (microworld). This allows humans to engage in experimental reasoning about the system and associated problems. These simulation models can be used to promote learning, hypothesis testing, decision making, and policy formulation if they are properly validated.30 The following examples offer two ends of the spectrum of approaches that can be used to build an understanding of clinical systems: process mapping and microworld simulations.
Understanding the clinical microsystem at the process level
“The first step is to draw a flow diagram. Then everyone understands what his job is. If people do not see the process, they cannot improve it.” W E Deming
The clinical microsystem provides a conceptual and practical framework for approaching organizational learning and delivery of care. Tensions exist between the conceptual theory and the daily practical applications of providing safe and effective care. Designing and redesigning care around the clinical microsystem is consistent with Donabedian’s model of structure, process, and outcome.31 Research on high performing microsystems has underscored the importance of process literacy coupled with effective measurement. Furthermore, a high degree of process awareness often drives the design of the work. The Spine Center at Dartmouth Hitchcock Medical Center provides an example of designing and implementing a program based on microsystem concepts.32 The Spine Center was built on a detailed understanding of core and supporting processes that would be required to provide care. The design team emphasized that improving clinical outcomes requires appreciating the inherent link between process and results. Ultimately, results depend on process. Linking performance and outcome data to the microsystem processes provides a helpful way to start identifying potential areas to focus improvement on the system that is producing the processes and outcomes of care rather than on the individual.16 The microsystem does not focus exclusively on outcomes; rather, it gives comparable attention to processes and structure, to the linkages among them, and to how they interact to respond to and meet the needs of the patient population.
An essential element in system analysis and monitoring is a physical and functional system mapping. This mapping is based on a comprehensive cognitive analysis which takes into consideration the sub- and supra-elements that allow the microsystem to function, as shown in fig 1. This systems alignment helps us understand the inter-connectedness of seemingly disparate parts of the healthcare system. For example, the hundreds of people that support the operating room team—blood bank technicians, radiology staff, intensive care unit personnel—enable the surgical microsystem to achieve its exceptional outcomes. Task analysis is a method used to describe and analyze how an individual (surgeon, nurse, patient) interacts both with the system itself and with others within that system. Task analysis describes what an individual is required to do in terms of cognitive processes, actions, or both to achieve the system’s goal. The task analysis is accomplished by observations of the process of care and interviews which carefully break down the multiple elements that are part of the microsystem. Figure 1 illustrates the complex interaction between the team, the support services, and hospital providers as well as the organizational structures that support these functions. It provides the foundations for understanding the relationships and transactions within the system and with its surrounding systems.
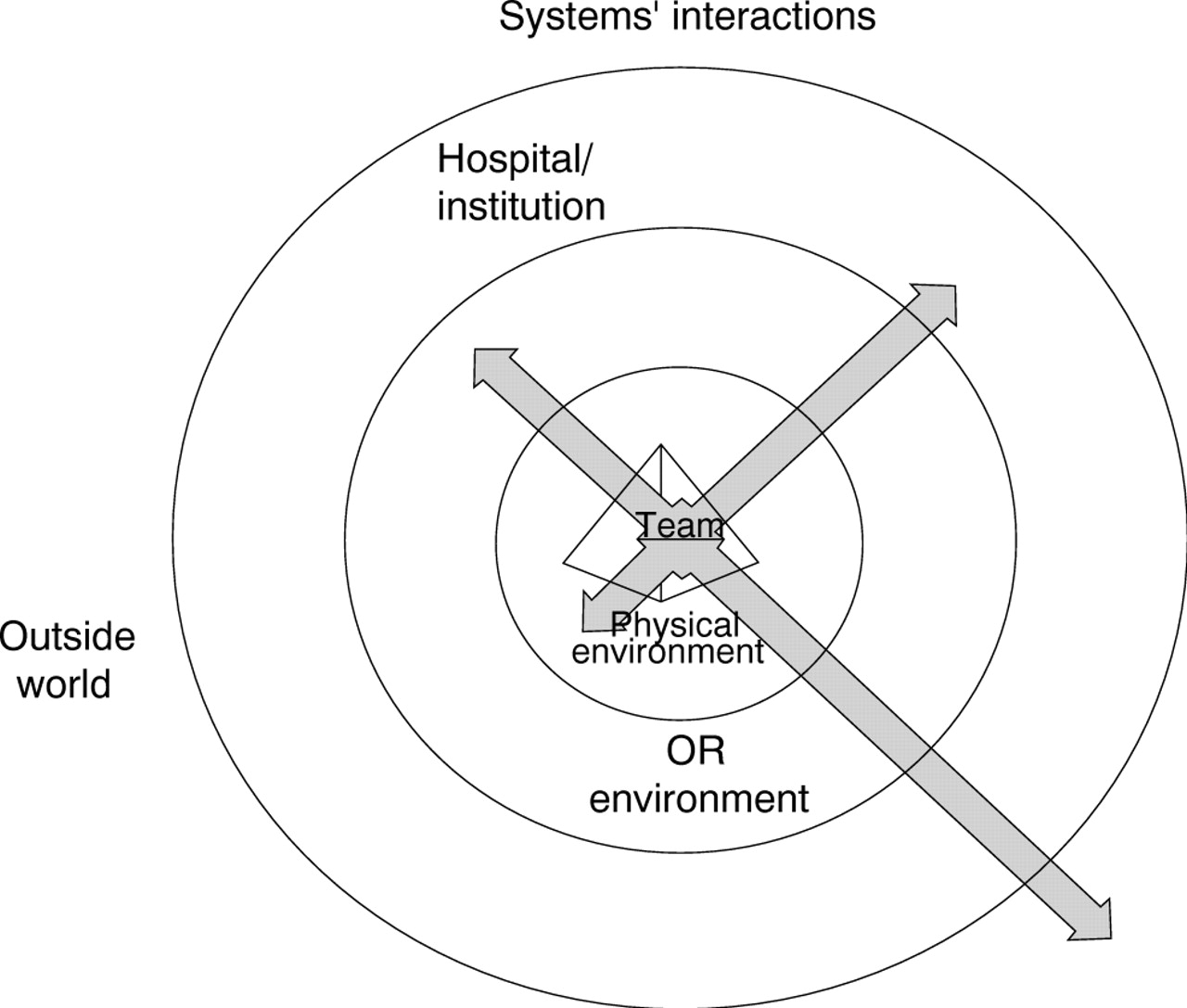
Graphic representation of a process analysis of the microsystem in supporting patient care and the organization.
System mapping has two other purposes. It serves as the “blueprint” upon which all changes (procedural and/or physical) are designed and analyzed before testing and implementation. It is also a “marketing” tool that facilitates “selling” the necessary changes to other teams and stakeholders. Internal marketing of change elements and process are often overlooked. Without local championship of change, system changes often fail. The importance of this cannot be overstated—the buy-in of local team system members is directly proportional to the local leadership provided by the microsystem champion.
Mapping the process of pediatric cardiothoracic surgery
We engaged providers and staff in a process mapping exercise to understand a microsystem designed to provide cardiovascular surgical care for children. Process mapping or flowcharting is a practical tool to create a picture of the sequence of steps in a process. Process mapping can be useful for planning a project, describing a standard way for doing a job (for example, in training and orientation), building consensus about the process (correct misunderstandings about the process), and reflection and improvement. Figure 2 includes several standard flowcharting symbols. Process maps can be created at different levels of granularity, from a high level overview of the major steps in the process to very detailed representation of each specific step or activity. Detailed process maps are especially helpful to standardize and improve processes. For use as an improvement tool, it is important to map the current process—not the desired process—so that opportunities for improvement can be identified. Being explicit about “core processes”—the basic work that involves patient care—can help providers and staff within the microsystem to shape what they know about their environment and provide insight into how to improve the process and overcome some of the barriers. The work that forms the core processes are made functional and operational by “supportive processes”. Both core processes and supportive processes are important to the functioning of the microsystem.33
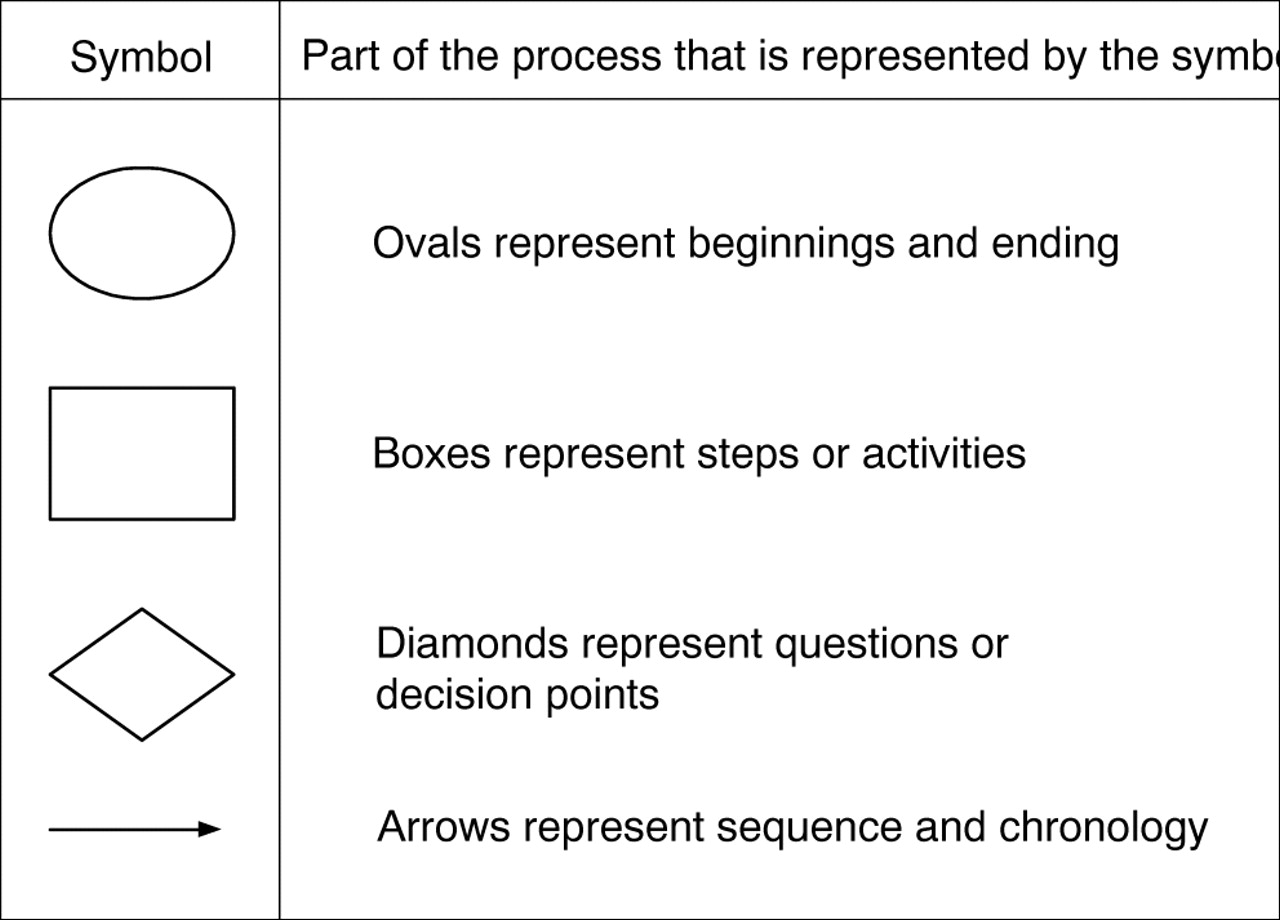
Process mapping symbols.
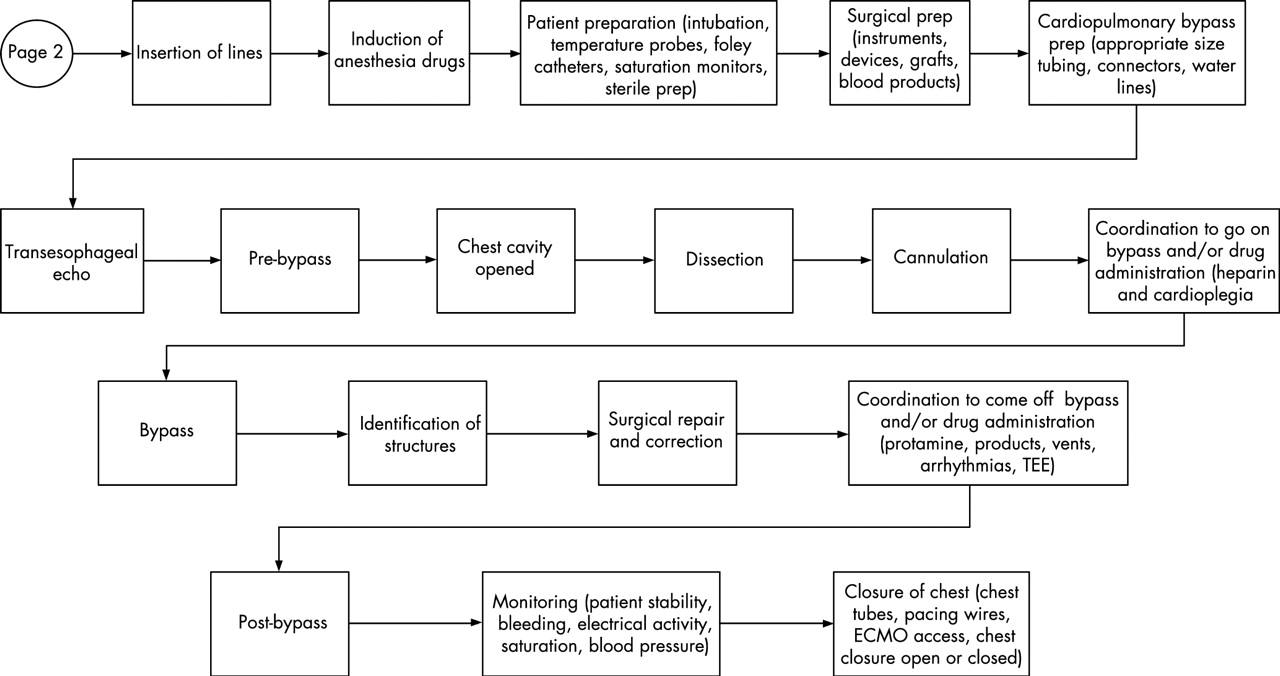
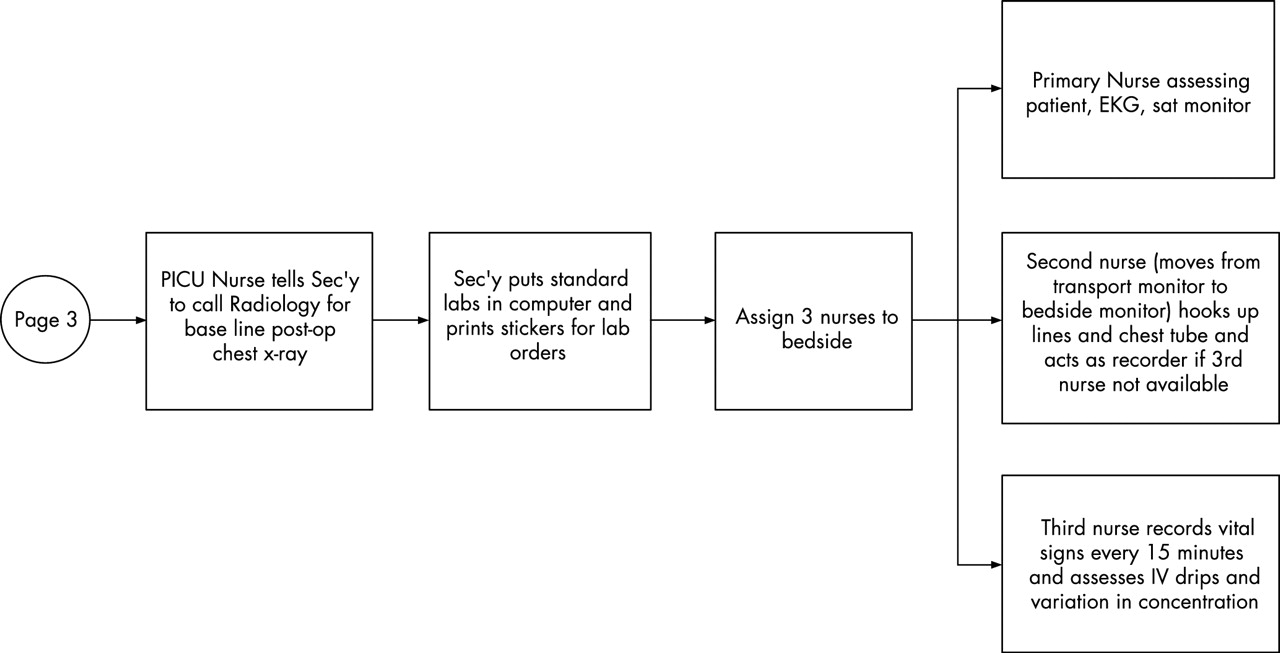
We asked the pediatric cardiothoracic surgical team members at two large urban medical centers to delineate the steps of care from the patient’s perspective, starting with the referral for surgery until the child’s first post-discharge follow up visit. We combined detailed walk-throughs, focused interviews, and task analysis to better understand the process.34 The process maps are shown in figs 3–5. Several questions are helpful when analyzing a process map to generate improvement ideas:

Process map of pediatric cardiovascular surgical care.

Process map of pediatric cardiovascular surgical care (continued).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Process map of pediatric cardiovascular surgical care (continued).
-
What is the goal of the process?
-
Does the process work as it should?
-
Are there obvious redundancies or complexities?
-
How different is the current process from the ideal process?
-
What are the various factions within the larger group, and how does this division support/hinder more effective processing of patient care?
-
What are the work-arounds to the proscribed process?
While mapping the process of care is an important step in designing improvements to the microsystem, we also found it to be instrumental in designing key aspects of a research protocol. We used a process mapping exercise to help us to assess the role of human factors on patient outcomes in pediatric cardiac surgery. As we completed the process mapping exercises and moved into the operating room to conduct observational studies, the process map became a data collection tool where data were linked to individual steps in the process. Furthermore, a process map can form the basis of the performance measurement tool, where measures are developed to assess and manage care at the process level and then several processes and corresponding measures are “rolled up” to assess and manage care at the microsystem level.
Understanding the clinical microsystem through microworld simulation
Society confronts a wide range of problems associated with increasingly complex and dynamic systems—for example, stabilizing national economies, sustaining responsible levels of growth and development, responding to crisis situations, designing engineering solutions for a variety of problems, delivering safe patient care, improving public health, protecting the environment, and educating society for the information age. These problems occur within the context of systems—economic systems, ecological systems, physical systems, human physiological systems, educational systems, and so on—and are addressed by organizations which comprise another kind of system—a social system. With increasing problem complexity it becomes more difficult to understand such systems and to act effectively.24,25 This complexity is coupled with the fact that groups of individuals with differing backgrounds and levels of experience are often involved, often including multiple organizations. Individual differences can play a significant role in problem solving efficacy in these domains as well as in health care, particularly varying with regard to the amount of previous relevant experience. Many problems critical to health care occur within the context of complex dynamic multi-agent systems. One way to explore these systems and the effect of various scenarios is through microworld simulations.
Microworld simulations are computer based models created by building an interactive simulation model and are used in accordance with the principles of facilitated learning. Each microworld simulation is based on a mathematical model validated against data gathered from real-world problem scenarios and constructed in such a manner that different hypotheses can be tested, decisions tried out in alternative situations, policies formulated and tested across a variety of situations, and data collected on the performance of the simulation model as well as on the users interacting with the simulations.
Microworld simulations are used as an experimental platform to test the basic questions about decision making misperceptions, cause-effect inferences, and learning. For example, the user might manage a simulated health care inventory of drugs for an oncology ward by placing simulated orders on a series of patients with multiple acuities and physiological constraints such as low platelet counts. Due to various delays, the inventory in this problem typically exhibits oscillations. The severity of the oscillations depends on the lengths and nature of delays and on the user’s decision making heuristics. Although this seems like a straightforward and simple exercise to successfully complete, research has shown that the performance of users is surprisingly poor.25 The numerous changing factors lead to decreased performance by the clinicians who did not take into account the changing nature of a series of patients. Literature also shows that users systematically misjudge the feedback and delay effects involved in the problem, which in turn causes poor performance due to relying on multiple assumptions.34 Other examples of microworld simulations include managing hospital electricity in a busy city grid during a crisis such as a hurricane, patient flow through a hospital, and triaging patients on a busy Saturday night in a chaotic large metropolitan public emergency room.
Hurricane Katrina in 2005 showed that both of these aspects (the problem aspect and the human aspect) play a critical role in an effective response to complex problems. Many aspects of hurricane preparedness in New Orleans were reasonably well understood, as there had been a full scale simulation that predicted levee failure and other dire consequences in 2004. Unfortunately, the responses to the actual crisis situation were ineffective at many levels with failure of command and control, strategic and tactical responses, and with regard to both large scale prevention and recovery (precautionary planning, providing support for the displaced) and small scale response and rescue (providing emergency medical care, rescuing people stranded on rooftops) situations.23–25 What went wrong and why? With well informed and well intentioned people involved at nearly every level, how could the response have been so disorganized and mismanaged? How can we avoid such problems in the future? Hurricanes are predicted to increase in the years to come and will very likely strike another heavily populated area.
Throughout each of these examples, the essential systems questions addressed at a generalizable level include:
-
Are there any consistent misperceptions of delays?
-
Are feedbacks withheld reducing the diagnosis and treatment decisions by providers and system planners?
-
Does such a system capture the relevant dynamics of the healthcare system and diagnostic situations?
-
Can this system be used effectively to improve medical diagnostic practice and planning?
Opportunities to develop microworld simulations are significant and can help to improve our understanding of how systems and microsystems behave under real time, personnel and other resource constraints. Data collected on the performance of the simulation model as well as on subjects interacting with the simulations will help to refine this powerful tool.35 Future research is needed to support the role of microsimulations and microsystems and their applications to help redesign health care. Human performance can be improved if individuals are trained, through the use of interactive simulations, to think holistically and systemically rather than exclusively in terms of particular subsystems, checklists, and standardized procedures. Evidence suggests that such simulations can improve performance and response to unexpected and unlikely situations, and they are widely used in pilot training and more recently in health care.36–3839
CONCLUSIONS: PRACTICAL APPLICATIONS FOR ENGINEERING SYSTEM DESIGN
Learning at the individual as well as at the organizational level interacts in important ways with organizational dynamics and structures. The clinical microsystem provides a conceptual and practical framework for approaching organizational learning and delivery of care. This paper has (1) helped to identify and consolidate principles of systems that can be generalized across disciplines and prove useful in and promoting understanding of complex human dynamics in healthcare microsystems; and (2) started to investigate human and organizational use of the models, including an analysis of the principles and the utility of the simulations to capture levels of expertise and human/organizational learning.
There are many ways to learn about the nature of the systems we work within. A theory of systems is required that can be used to generate system models and representations at various levels of granularity. This may include high level process maps of the core clinical care processes as well as a detailed and formal representation of a complex system so that a synthetic version of reality can be created in the form of an interactive simulation model (microworld) that will allow humans to engage in experimental reasoning about the system and associated problems. Through process mapping, the key processes of a microsystem are delineated and assessed from the perspective of how the individual interacts with the system. Systematic analysis of the key and supporting processes of a microsystem using these tools is an important element of the continuous learning cycle of clinical microsystems and healthcare organizations.
REFERENCES
Footnotes
-
This work was partially supported by a grant from the American Heart Association, Award Number 0330274N.
-
Competing interests: none.
-
Full Ethics Committee/IRB approval was secured for this study at the Universities of Chicago and Miami.