Article Text

Abstract
Background: All anaesthetists have to handle life threatening crises with little or no warning. However, some cognitive strategies and work practices that are appropriate for speed and efficiency under normal circumstances may become maladaptive in a crisis. It was judged in a previous study that the use of a structured “core” algorithm (based on the mnemonic COVER ABCD–A SWIFT CHECK) would diagnose and correct the problem in 60% of cases and provide a functional diagnosis in virtually all of the remaining 40%. It was recommended that specific sub-algorithms be developed for managing the problems underlying the remaining 40% of crises and assembled in an easy-to-use manual. Sub-algorithms were therefore developed for these problems so that they could be checked for applicability and validity against the first 4000 anaesthesia incidents reported to the Australian Incident Monitoring Study (AIMS).
Methods: The need for 24 specific sub-algorithms was identified. Teams of practising anaesthetists were assembled and sets of incidents relevant to each sub-algorithm were identified from the first 4000 reported to AIMS. Based largely on successful strategies identified in these reports, a set of 24 specific sub-algorithms was developed for trial against the 4000 AIMS reports and assembled into an easy-to-use manual. A process was developed for applying each component of the core algorithm COVER at one of four levels (scan-check-alert/ready-emergency) according to the degree of perceived urgency, and incorporated into the manual. The manual was disseminated at a World Congress and feedback was obtained.
Results: Each of the 24 specific crisis management sub-algorithms was tested against the relevant incidents among the first 4000 reported to AIMS and compared with the actual management by the anaesthetist at the time. It was judged that, if the core algorithm had been correctly applied, the appropriate sub-algorithm would have been resolved better and/or faster in one in eight of all incidents, and would have been unlikely to have caused harm to any patient. The descriptions of the validation of each of the 24 sub-algorithms constitute the remaining 24 papers in this set. Feedback from five meetings each attended by 60–100 anaesthetists was then collated and is included.
Conclusion: The 24 sub-algorithms developed form the basis for developing a rational evidence-based approach to crisis management during anaesthesia. The COVER component has been found to be satisfactory in real life resuscitation situations and the sub-algorithms have been used successfully for several years. It would now be desirable for carefully designed simulator based studies, using naive trainees at the start of their training, to systematically examine the merits and demerits of various aspects of the sub-algorithms. It would seem prudent that these sub-algorithms be regarded, for the moment, as decision aids to support and back up clinicians’ natural responses to a crisis when all is not progressing as expected.
- crisis management
- anaesthesia complications
- accidents
- human error
- system failure
Statistics from Altmetric.com
All anaesthetists have to manage life threatening crises which may arise with little or no warning.1–4 Indeed, with a risky procedure in a sick patient, much of the working day may be spent preventing and heading off potential crises. Anaesthetists manage the vast majority of these complex problems promptly and efficiently with skilled pattern recognition and frequently practised clinical routines. However, high profile cases documented in the lay press from around the world indicate that these patterns of response do not always lead to the resolution of problems.5 Attention has been focused worldwide on the safety of health care and the ways in which it may be enhanced. Working groups from several countries including the USA,6 UK,7 and Australia8 have produced documents outlining plans for improving the safety of health care. This set of 25 articles outlines a structured approach for when things are going wrong during anaesthesia.9–32 Prevention is, of course, better than cure. However, prevention (for example, appropriate preoperative assessment, checking and planning) is not the intent of this set of articles.
As indicated above, situations do arise during which patient safety is compromised when the usual measures have been or are being taken. This is the context in which an incident report may be submitted. The Australian Incident Monitoring Study (AIMS) was started in 1988.33 In 1993 a symposium issue reviewing the first 2000 incidents was published in the journal Anaesthesia and Intensive Care.34 The symposium consisted of 30 papers looking at various aspects of anaesthetic incidents. These included clinical crises and adverse events (such as anaphylaxis, difficult intubation, cardiac arrest, the wrong drug problem), assessments of the applications and limitations of physiological monitors (for example, the pulse oximeter, the electrocardiograph, the capnograph), and an evaluation of the factors involved in the generation and resolution of these incidents. In seven out of every eight incidents which arose when patients were breathing gas from an anaesthetic machine, the anaesthetists involved recognised the problem and responded appropriately.4 However, in one out of every eight it was considered by an AIMS panel of reviewers that the application of a simple learned routine, properly applied, would have expedited the diagnosis and/or led to an appropriate response more rapidly—and often more effectively.4 This is because previously learned and intuitive strategies and work practices which have evolved for speed and efficiency under normal working conditions may fail to adjust in a crisis.35 Use of such “pre-compiled responses” is consistent with the “rapid phase” learned responses to some crises in aviation, nuclear plant operation, community rescue organisations, and military command, many of which are routinely tested in simulation situations.2
These findings suggested that there is a place for defaulting to a simple structured routine when the anaesthetist is uneasy that all may not be what it seems to be, when the situation is deteriorating, or when an adverse outcome seems likely. It is well recognised within the field of human error and safety that the use of simple succinct guidelines and protocols reduces the burden on the individuals involved and allows their limited available cognitive resource to be used for essential immediate tasks.36,37 Some of the principles underlying this structured approach have been dealt with in a companion paper.35
THE “COVER–ABCD A SWIFT CHECK” CORE ALGORITHM
After considering a number of alternatives, it was generally agreed after a series of three meetings, each attended by 60–100 anaesthetists, that a “core” algorithm should form the basis for the management of any crisis in which the anaesthetist was uncertain of the exact cause or which was not going exactly as expected.4 A common starting sequence for all crises was thought to be essential because it was recognised that it is very difficult to recover from a “mind set” that a particular problem is being faced when, in fact, the problem is a different one requiring a completely different solution.
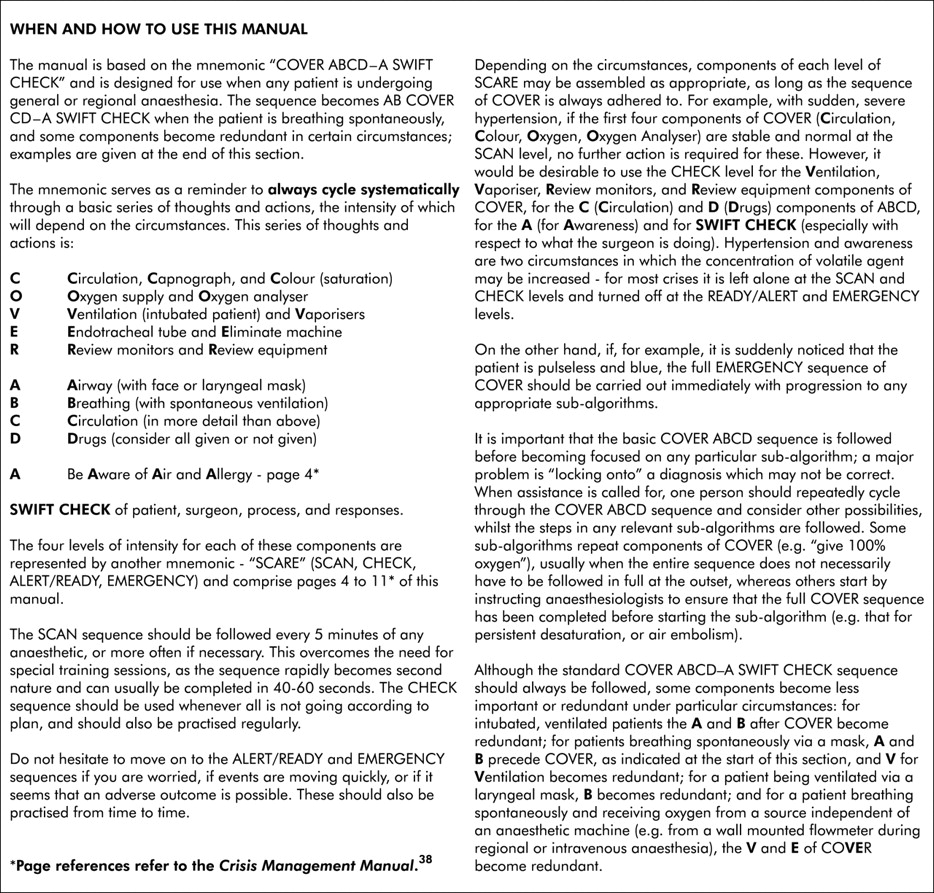
Such a core algorithm was devised based on the mnemonic “COVER ABCD–A SWIFT CHECK” which is suitable for use when any patient is undergoing general or regional anaesthesia. The original version, which was available on two sides of a single laminated sheet, is shown in tables 1 and 2. When the manual which resulted from this set of 25 articles was compiled, more detailed instructions were made available about aspects of this core algorithm (see figs 1 and 2). The use of the traditional cardiac arrest mnemonic “ABCD” was considered but it was thought that it would “miss” some dangerous problems related to the surgery, the use of the anaesthetic machine, and ancillary equipment which would require immediate resolution; this is discussed in the last section of this paper.
The initial component, COVER—which addresses problems arising from circulatory compromise, the gas supply, the anaesthetic machine, the breathing circuit, the ventilator and the endotracheal tube—has been validated against the 1301 relevant incidents under general anaesthesia amongst the first 2000 reported to AIMS.4 It was found that just under 60% of these problems had arisen from these sources and that COVER, correctly applied, would have provided a functional diagnosis and an appropriate response in virtually all the cases in 40–60 seconds.4 Subsequent users and many case presentations at audits have confirmed that COVER can be rapidly performed and is reliable.

Final instructions and abbreviations for the Crisis Management Manual.
If the remainder of the algorithm had been used (ABCD–A SWIFT CHECK), it was considered that, correctly applied, a functional diagnosis would have been obtained in 99% of these incidents. However, unlike the COVER component, the ABCD–A SWIFT CHECK component is largely a diagnostic checklist. The anaesthetist would still have to handle the 40% of problems remaining after COVER—that is, those arising from the patient or from patient/doctor/procedure/drug interactions. To do this the anaesthetist may work from first principles, employ pattern recognition and learned sequences or, failing this, apply one of a set of prescribed sub-algorithms. Experience from audits of anaesthetic practice and ongoing review of AIMS forms has confirmed that it would be desirable for there to be a basic set of structured sub-algorithms to handle the problems arising from these sources when the problem is not immediately resolved, as on many occasions the management described constitutes a considerable departure from what would generally be regarded as currently accepted practice. The development of the 24 sub-algorithms deemed necessary is described in the other articles in this series as shown in table 3.9–32
How this was done is presented below. However, first, the issue of how to use the “COVER” component of the core algorithm is discussed in more detail.
HOW TO USE “COVER”
An important issue to arise from discussions about the core algorithm was the question as to when and how it should be invoked. The majority of potential incidents are recognised early in their evolution and are “headed off” by appropriate responses on the part of the anaesthetist. Of those events that actually moved an anaesthetist to fill in an incident report, seven out of eight were correctly recognised and promptly handled; for these, pattern recognition was clearly successful and the use of COVER was unnecessary, and would potentially have been more time consuming and disruptive than the initial response.
How should the anaesthetist recognise when the situation justifies invoking the full set of actions required by COVER?4 It is obvious, for example, that it is not worth getting rid of the anaesthetic machine when the saturation falls from 98% to 94% over 10 minutes. However, it is equally obvious that COVER should be invoked in full if a patient is suddenly found pulseless and cyanosed with slow wide QRS complexes on the electrocardiogram.
“SCARE”
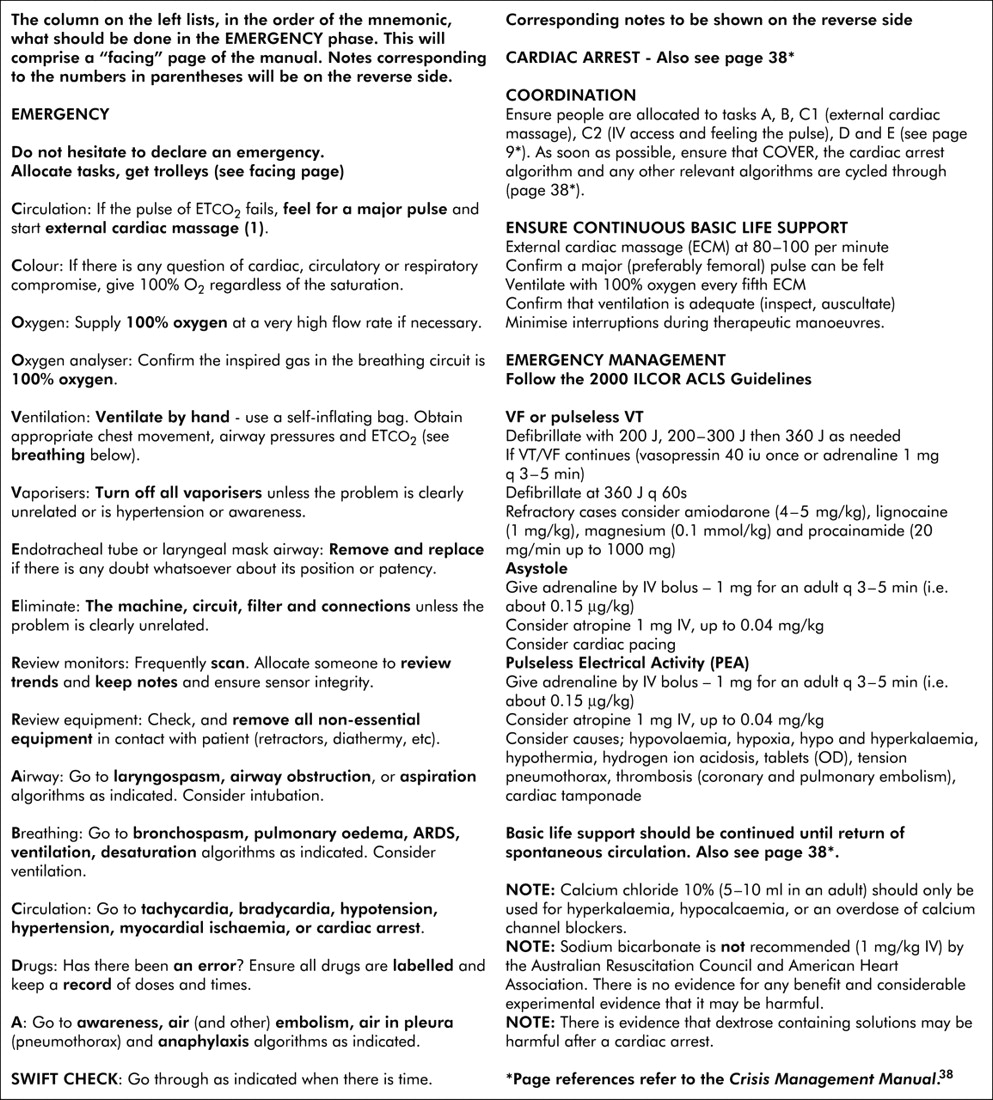
A solution to this problem lies in grading the application of each component of COVER into four levels represented by the mnemonic “SCARE”, depending on the degree of perceived urgency (Scan-Check-Alert/Ready-Emergency). These are shown in figs 3–6.
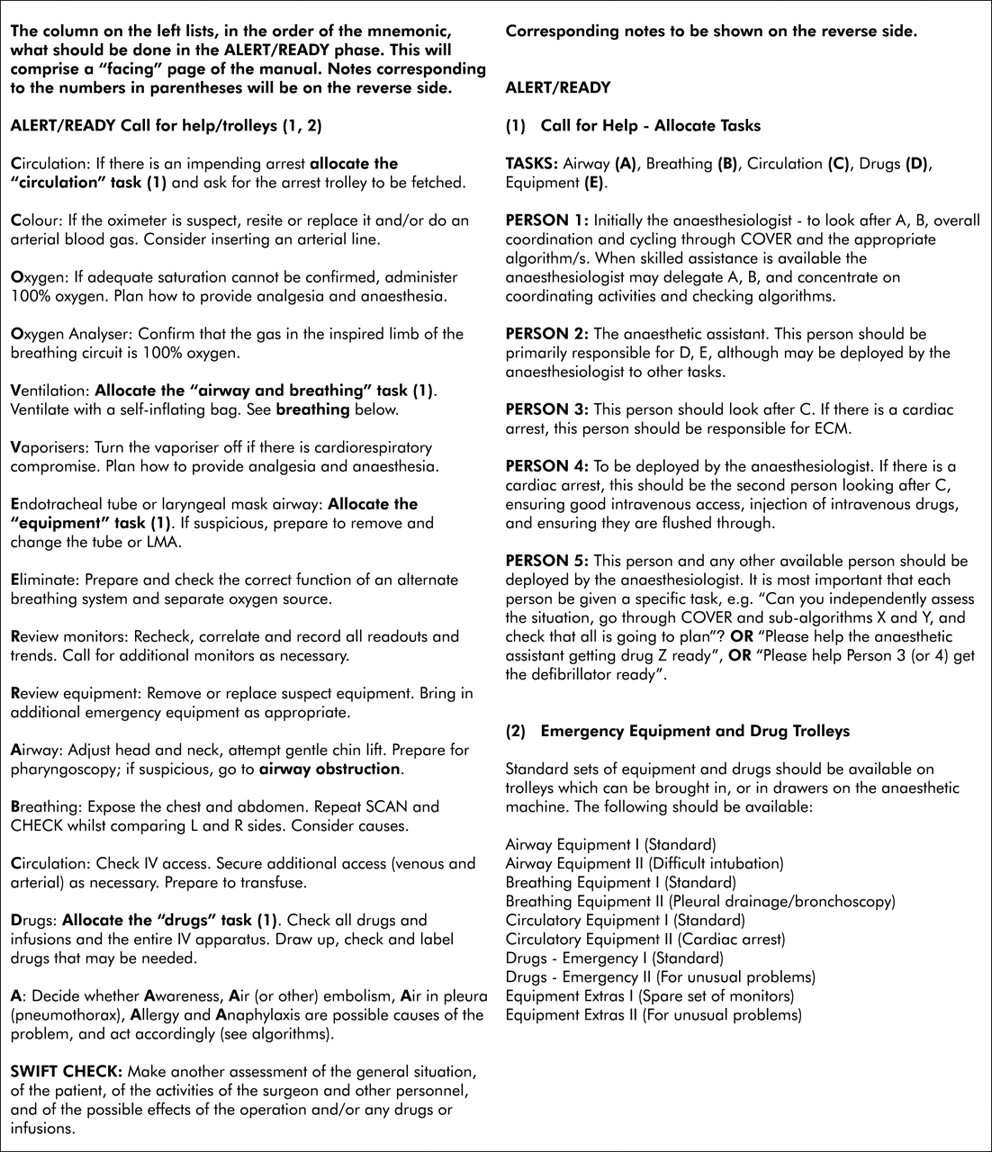
Items which, in the order of the mnemonic, should be done in the ALERT/READY phase.
The various levels of each component of COVER should be used in combinations deemed appropriate for the situation. This provides great flexibility and appropriateness of response while still reducing the cognitive load for the anaesthetist. It can be argued that COVER is no longer an algorithm when different actions can be taken, depending on circumstances, and that it should more properly be called a “cognitive aid”, encouraging the use of various “pre-compiled responses”. However, for the sake of simplicity, we will continue to use the term algorithm for this set of articles.

Items which, in the order of the mnemonic, should be done in the emergency phase
The use of the SCAN level every 5 minutes during each case (fig 3) and of the CHECK level at regular intervals (fig 4) also overcomes the problem of regular formal training being required for the effective use of the core crisis management algorithm. Commercial jet airline pilots are required to undertake simulator sessions and be accredited every 3 months. However, to introduce this for every practising anaesthetist, whilst desirable, is not feasible at the moment, especially in developing countries.
In general, the slower and less serious the deviations from normal and the more monitoring and other information available, the less likely it will be that the EMERGENCY mode of COVER will need to be used. However, in circumstances in which the situation is obscure or not readily apparent due to opaque or non-specific signs, or is progressing rapidly, there should be no hesitation in invoking the algorithm to the full. In contexts in which no monitors are available, it is likely that the full application of the EMERGENCY mode of COVER would be much more frequently invoked.39
For those who have practised using COVER in this way, appropriate responses may rapidly be achieved while the anaesthetist is confident that the majority of possible contingencies have been accounted for. This knowledge is valuable for trainees who have not yet fully developed their pattern recognition and clinical response routines, for any anaesthetist who encounters a novel situation, when all is not going well, or when there is likely to be an adverse outcome. In this last context, the anaesthetist can proceed with handling the problem to the best of his or her ability, taking some comfort in the knowledge that any independent retrospective review must find that the appropriate responses had been made for over 99% of the spectrum of problems reported to AIMS.
The SCARE algorithms have been incorporated into the Crisis Management Manual developed from this set of 25 articles.38 There has been considerable feedback that the use of this SCARE-based graded response has proved to be quite satisfactory for those who have decided to use the manual as it is. However, the concept of using such a highly structured graded response does not have universal acceptance. Some prefer to remember the COVER algorithm only for emergency use when pattern recognition appears to have failed. Also, while the SCAN routine of the COVER mnemonic is perfectly satisfactory, some clinicians prefer their own “SCAN” routine based on local circumstances and their own equipment setup.
It is recognised that complexity can cause errors13 and that reducing choice, reducing the number of steps required, and ensuring that the duration of execution is as short as possible all assist in reducing the complexity of a system. However, this should not be at the cost of ensuring safety. There is a trade-off between relying on pattern recognition and using the highly structured approach represented in the Crisis Management Manual by the SCARE sequence. The challenge is to cover all contingencies while retaining as simple a set of responses as possible. It is likely that COVER will be refined with more use; there are advantages to defaulting to a standard sequence of actions when people have to work in teams in a crisis.36
“ABCD–A SWIFT CHECK”
The rationale for the use of sub-algorithms for the ABCD–A SWIFT CHECK portion of the mnemonic is the same as that which underpins the use of the core algorithm for the first part (COVER). Complex problems may be manifested by non-specific cues in circumstances in which a minor transgression or a delay in taking corrective measures might have serious consequences. For example, of 179 incidents first detected by oximetry and thus having manifested as desaturation, just under three quarters (represented by nine “clinical situations” including dangerous problems requiring rapid resolution such as hypoxic gas mixture and undetected oesophageal intubation) were handled by COVER.4,39,40 However, over one quarter fell into the ABCD–A SWIFT CHECK portion of the algorithm. These were represented by 12 “clinical situations”, some of which had relatively rare or obscure causes but required rapid diagnosis and a prompt response—for example, anaphylaxis, air embolism, tension pneumothorax, pulmonary oedema. In some of these cases the correct diagnosis was “missed” for a prolonged time. With such an array of possibilities it is too time consuming to work from first principles. In such circumstances, if the problem is not resolved immediately by actions based on pattern recognition, the use of a carefully validated prescribed algorithm is safer and more reliable than trying to work out what the problem is, and what to do about it, from first principles.
Early on, a number of anaesthetists commented that they found the use of A SWIFT CHECK as a mnemonic, as shown in table 2, to be contrived and unhelpful. It was therefore replaced as follows. Firstly, the sentence “Be Aware of Air and Allergy” was suggested as a reminder for what the As in A SWIFT CHECK stand for (Michael Burt, personal communication). Each A in this sentence acts as a reminder for two things: Awareness in the patient and as an exhortation to the anaesthetist to be Aware; Air for Air (and other) embolism and for Air in the pleural space (pneumothorax); and Allergy to act as a reminder for Allergic reactions and Anaphylaxis (see table 3).
Secondly, it was suggested that the SWIFT CHECK should now be taken simply as a reminder for a swift check during the normal 5 minute scan “of the surgeons’, assistants’, nurses’ and orderlies’ activities and of the operative site, a quick consideration of the pattern of physiological change revealed by the monitors, and a mental review of the patient’s history and preoperative status”.4 The conditions listed under SWIFT CHECK in table 2 have been dealt with in some of the companion papers (see asterisks in table 3) and in some additional algorithms in the Crisis Management Manual.38
DEVELOPMENT OF THE SUB-ALGORITHMS
Following analysis of the first 2000 reports as described in the 1993 symposium issue,34 the need for a number of specific sub-algorithms was identified to assist the anaesthetist in treating the remaining 40% of the incidents that were not corrected by the COVER core algorithm. Volunteer anaesthetists were given sets of incident reports from the first 4000 AIMS reports that dealt with the specific clinical problems shown in table 3. These sets were generated by using the key word section on the AIMS form. For incidents that involved large numbers of reports (such as airway obstruction and desaturation), at least two anaesthetists were involved in the initial data analysis while for those where there were fewer reports (such as water intoxication) one investigator initially reviewed the data. As the majority of reported cases were clearly dealt with well, the reporting anaesthetists’ described actions played an important role in creating the crisis management sub-algorithms. Each sub-algorithm was developed by those who had reviewed the reports and by at least one other specialist with a clinical interest in that area. Once a sub-algorithm had been created, the relevant analysts again reviewed each of the reports in the relevant set. The potential value of using a structured approach—that is, the application of COVER ABCD–A SWIFT CHECK to the diagnosis and initial management of each problem—followed by the application of the sub-algorithm for that specific problem was assessed in the light of each of the relevant AIMS reports from the first 4000. This was done by comparing the potential effectiveness of the structured approach for each incident with that of the actual management, as recorded in each report. A judgement was made by the reviewers as to whether the sub-algorithm, properly applied, would have led to a better or quicker resolution of the problem, and specific consideration was also given to whether use of the sub-algorithm could have caused a problem. Other relevant aspects of the incidents were tabulated. A paper was then written for each sub-algorithm outlining the background to the subject, with a description of the methods and the results of the evaluation for each sub-algorithm. These papers make up the rest of this set of 25 articles.9–32
Fourteen sub-algorithms for the ABCD portion of the mnemonic were developed and checked against the relevant incidents among the first 4000 reported to AIMS. Four were developed and checked for the four “As” of A SWIFT CHECK and six for aspects of SWIFT CHECK (see table 3). These sub-algorithms were then compiled as the original Crisis Management Manual.38
THE CRISIS MANAGEMENT MANUAL
The original Crisis Management Manual was developed as a 74 page document.38 Two thousand copies of this draft manual were distributed at the 1996 Scientific Congress of the World Federation of Societies of Anaesthesiologists held in Sydney, Australia. Comments and feedback were sought from those to whom the manuscript was delivered. These comments were then incorporated, wherever relevant, into the crisis management sub-algorithms. The refined sub-algorithms which resulted are shown in this set of 24 articles.
Each of these forms the basis for a page in the Crisis Management Manual. In the hard copy version of the manual there are easy-to-use tabs down the right hand sides of the pages to allow the anaesthetist immediate access to sub-algorithms for problems with non-specific cues such as desaturation, but which also allow direct access to sub-algorithms for specific problems such as anaphylaxis or air embolism, when these are immediately recognised. There are also tabs at the tops of the first few pages for rapid access to the SCARE sequences.
An electronic copy of the algorithms in the manual was made available on the internet.38 Unlike paper manuals, these web based manuals are more flexible and allow rapid updates to all users. With the more frequent use of personal computers and hand held devices, it was felt that this would be a beneficial medium in which to house the manual. To this end, an electronic software form of the manual has been developed using hypertext documentation that can be used on a personal computer or a hand held personal desk assistant (e.g. Palm Pilot™). The program uses frames with resizable boxes and scroll bars on the sides. Underlined text expands into full text boxes and, within the crisis algorithm itself, collapsible headings and hyperlinks and pop-up boxes are used to fully describe each of the sub-algorithms. The personal computer program is of most use as a teaching tool, while the ease of use and instant availability of a hand held device allows the manual to be instantly accessible during times of a crisis. This version is currently being used by some trainee anaesthetists in New Zealand (Charles Bradfield, personal communication).
COMMENTS ON THE CRISIS MANAGEMENT MANUAL
Since the publication of the core algorithm, five meetings on crisis management have been held: one at Noosa in Queensland in June 1993; one at Toukley in New South Wales in March 1994; and two 2 day meetings in association with Annual Scientific Meetings of the Australian Society of Anaesthetists, one in Fiji in November 1994 and one in Melbourne in October 1995. Finally, the electronic version was demonstrated at the 2001 Annual Scientific Meeting of the Australian Society of Anaesthetists in Canberra. The 2001 Canberra meeting was especially important as it was the first meeting for several years following dissemination of the draft manual. At all of these meetings the sub-algorithms presented in this issue were presented, discussed, and refined. It was recognised that the methods used for “validating” the algorithms were intrinsically limited and subject to “hindsight bias”. Prospective validation using simulation would be ideal but will require a large scale, carefully designed study.
It was agreed by all that the algorithms should only be used when the usual responses based on pattern recognition do not appear to have been successful. Also, right from the start it was agreed that the use of the traditional cardiac arrest mnemonic “ABCD” was too limited for more complex problems which arise because of the interposition of artificial gas supplies, anaesthetic machines (with additional hazards such as vaporisers), artificial airways, and various breathing circuits with failure prone components such as one-way valves and arrangements for carbon dioxide absorption. For example, hypoxic gas mixtures (especially 100% nitrous oxide), potentially fatal vapour concentrations, and circuit “over-pressures” must be excluded almost immediately or severe patient harm or death may ensue rapidly. A number of additional important points were raised at the various meetings.
Firstly, it is important to recognise that the AIMS reports simply constitute a body of information arising from occasions when anaesthetists were sufficiently interested or concerned by an event to report it and the surrounding circumstances as an incident. It is known that common or mundane events are under-reported—for example, circuit disconnections and leaks are under-reported but are nevertheless the most frequently reported incidents—whereas very dramatic and unusual events are more likely to be reported—for example, anaphylactic reactions or air embolism.41,42
The relative frequencies with which various types of incident are reported thus provide some hybrid reflection of the relative frequency with which they occur and the degree of interest or alarm they engender. Although reporting such comparative frequencies may produce considerable unease in classical epidemiologists, it does have practical relevance to a body of anaesthetists who are provided with a prioritised catalogue of events sequenced according to their perceived relative importance by fellow practitioners.39 Half of New Zealand anaesthetists who responded to a survey (57% response rate) felt that AIMS had changed their practice.43
The second issue addressed was whether the AIMS data are relevant to crises that actually have adverse outcomes. Data from anaesthetic deaths which were substantially attributed to anaesthetic management and which occurred within 48 hours of anaesthesia in the UK (790 deaths) and New South Wales (172 deaths) indicate that the AIMS data are relevant.39,44 In 80% of the deaths on the same day the first sign of disaster was a life threatening crisis. Of all these crises leading to death, three quarters are in the AIMS “top 10” and nearly all the remainder are in the next 10.39 There is also a striking similarity between the presenting signs in the UK and New South Wales studies (table 4);44 the non-specificity of these signs confirms that a structured approach would be desirable as there was a large number of causes of the underlying problems.
In the UK study 30% of deaths were in patients who were ASA grade 1–4 and in the New South Wales study 40% of deaths were in patients regarded as being “fair risks”. The conclusions that AIMS crises are relevant for validating crisis management algorithms, that many crises which result in death start with non-specific signs, and that problems may arise in low or moderate risk patients all support the routine use of a structured algorithm. Studies from elsewhere have confirmed that there is a strong association between “initial process events” and poor outcomes.45,46
The third problem which arose for discussion was that, even if structured algorithms are available, poor team work may compromise their execution. Again, the ideal is that practising anaesthetists should undergo regular simulation sessions in which they play various roles in crisis situations—that is, the equivalent of cockpit resource management sessions in the aviation industry.47–49 However, in reality this will not be possible for all anaesthetists in the near future. Experience from attending real crises and from observing Australian anaesthetists in simulated crisis situations—for example, during the crisis management simulation session in Toukley, New South Wales in March 1994—confirms that teamwork is often poor. The use of a crisis management manual allows a coordinating person (usually an anaesthetist) to allocate tasks for individual members of the operating room team. In this way, tasks will be prioritised and it will be ensured that the essential basic tasks are carried out in the correct sequence and in an expeditious manner. The value of a crew resource management approach cannot be overemphasised and its introduction into clinical practice needs to be widely supported.2,49 Better communication was cited by over two-thirds of operating room nurses and doctors as the most important intervention required to improve safety,49 underlining the importance of moving towards formal team training using simulators.
This may be based on the use of crisis management algorithms which, in the future, may be available as part of the software of integrated monitoring devices and clinical decision support systems. The first step was producing Palm and PC-based versions of this crisis management manual. The introduction of such an approach into commercial monitoring systems has gained interest by some manufacturers and is well recognised as being an effective way of applying information of this sort.50,51
Fourthly, the use of COVER ABCD–A SWIFT CHECK and the sub-algorithms does not guarantee a good outcome—merely that an appropriate sequence of actions will have been carried out in the vast majority of cases. In some instances something will have been done (such as a wrong drug given) or something will have occurred (such as pulmonary embolism) that has consequences that the anaesthetist cannot reverse or even control. Also, it is inevitable that the “core” algorithm and sub-algorithms will not always be correctly applied. However, if this is the case, as long as these are available in an easy-to-access form, others called to assist in the management of an escalating crisis will have a fresh chance of resolving the problem.
The sub-algorithms have been designed to be a simple set of instructions that can be followed in an emergency. It is inevitable that these algorithms will differ from “accepted practice” in some regions and do not represent the only acceptable course of action. However, it is suggested that they be followed in crises when pattern recognition has failed, at least in the first instance, as they have been designed to represent appropriate courses of action in the vast majority of circumstances. If this structured approach proves to be unhelpful, the anaesthetist can always revert to problem solving from “first principles”. The relevant sub-algorithm should also be examined following resolution of an incident to ensure that the reason for the crisis has not been missed and to facilitate appropriate ongoing care and management. Although the structured approach advocated may not be the best for every situation, it will be consistent, is unlikely to harm the patient, will assist in the diagnosis of the problem in 99% of cases, and will be better than the current clinical management by the average clinician in at least one in eight incidents.
Finally, crisis management is not complete until the consequences for the patient, his or her friends and relatives, all medical (and other) staff involved, and the implications for the institution, practice or system have been dealt with.52 An approach to this is outlined in the final paper in this set of articles32 and forms the last section of the Crisis Management Manual.38 An “open disclosure” standard has now been developed by the Australian Council for Safety and Quality in Health Care which supplements the approach advocated in this last section of the manual.53
The sub-algorithms presented in this set of 24 articles were developed as an adjunct for the practising clinician to use in the resolution of incidents that occur during anaesthesia. They are didactic but are open to debate, discussion, and criticism. They form the basis of what we believe to be a useful step in developing a rational evidence-based approach to crisis management during anaesthesia. However, much remains to be done. The COVER component has been found to be satisfactory in real life resuscitation situations.54 Carefully designed simulator based studies, using naïve trainees right at the start of training, could evaluate the approach advocated here against possible alternatives, and could systematically examine the merits and demerits of various aspects of the sub-algorithms and how they are presented. The extent to which “pre-compiled responses” should be required to be used—as in aviation and by the policies of some hospitals with respect to the use of cardiac arrest protocols—is likely to be the subject of lively debate as medical practice receives increased scrutiny. Due to the complexities of clinical medicine, however, it would seem prudent, for the foreseeable future, that the “core algorithm” and “sub-algorithms” described in this set of articles be regarded as “decision aids” to support and back up a clinicians’ natural responses to a crisis when all is not progressing as expected.55
Key messages
-
This paper forms the introduction to a set of 24 articles that outline a structured approach for use when things go wrong during anaesthesia. Prevention is not the intent of this set of articles as the focus is on crisis management.
-
From three meetings involving 60–100 anaesthetists it was agreed that a “core” crisis management algorithm was needed when either cause or response to treatment during an anaesthesia crisis was not apparent.
-
From the study of the first 4000 incidents reported to AIMS, a need for 24 specific sub-algorithms was identified based on successful strategies identified in the reports.
-
Using the application of the previously reported core algorithm, the 24 sub-algorithms were assembled in a user friendly manual for trial against the 4000 incident reports.
-
The trial showed that this structured approach would aid in diagnosis in 99% of crises and would provide better management than that of the average clinician, without patient harm, in one in eight of the situations.
-
Poor teamwork may compromise the execution of a structured algorithm.
-
These algorithms will differ from “accepted practice” in some regions and do not represent the only acceptable course of action.
-
Such structured approaches lend themselves readily to simulation training in anaesthesia, resuscitation, and intensive care.
Crisis management algorithm – memorise and practise: an explanation of each cue in the mnemonic “COVER ABCD”
“A SWIFT CHECK” (the checklist arising from the mnemonic need not be memorised but should be immediately available in the operating theatre)
Papers in Crisis Management series
Comparison of mode of presentation of 360 NCEPOD* and 138 NSW** crises44

Introduction to the Crisis Management Manual.

Items which, in the order of the mnemonic, should be SCANNED.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Items which, in the order of the mnemonic, should be CHECKED.
Acknowledgments
The authors would like to thank all the anaesthetists in Australia and New Zealand who contributed to the 4000 incident reports upon which this and the other 24 papers in the Crisis Management Series are based. The coordinators of the project also thank Liz Brown for preparing the draft of the original Crisis Management Manual; Loretta Smyth for typing; Monika Bullock RN for earlier coding and classifying of data; Dr Charles Bradfield for the electronic version of the algorithms; Dr Klee Benveniste for literature research; and Drs Klee Benveniste, Michal Kluger, John Williamson and Andrew Paix for editing and checking manuscripts.
REFERENCES
Footnotes
-
This study was coordinated by The Australian Patient Safety Foundation, GPO Box 400, Adelaide, South Australia 5001, Australia.
Linked Articles
- Quality Line
- Crisis management