Article Text

Abstract
Background Sign-out is the process (written, verbal or both) by which one clinical team transmits information about patients to another team. Poor quality sign-outs are associated with adverse events and delayed treatment. How different specialties approach written sign-outs is unknown.
Objective To compare written sign-out practices across specialties and to determine consistency of content, format and timeliness.
Methods The authors evaluated all non-Intensive Care Unit written sign-outs from five inpatient specialties on 18 January 2012, at Yale-New Haven Hospital, focusing on content elements, format style and whether the sign-outs had been updated within 24 h. In our institution, all specialties used a single standardised sign-out template, which was built into the electronic medical record.
Results The final cohort included 457 sign-outs: 313 medicine, 64 general surgery, 36 paediatrics, 30 obstetrics, and 14 gynaecology. Though nearly all sign-outs (96%) had been updated within 24 h, they frequently lacked key information. Hospital course prevalence ranged from 57% (gynaecology) to 100% (paediatrics) (p<0.001). Clinical condition prevalence ranged from 34% (surgery) to 72% (paediatrics) (p=0.005).
Conclusions Specialties have varied sign-out practices, and thus structured templates alone do not guarantee inclusion of critical content. Sign-outs across specialties often lacked complex clinical information such as clinical condition, anticipatory guidance and overnight tasks.
Statistics from Altmetric.com
Introduction
Handoffs occur during a change in responsibility for a patient from one care provider or team to another.1 Patient handoffs have become increasingly central as duty restrictions have led to increased transfers of care.2 Clear and concise interactions between physicians during handoffs are important for ensuring patient safety, as poor communication often contributes to medical errors.3 Sign-out is the process (either written, verbal or both) by which information is transmitted about patients from one medical team to another.1 Failure to communicate relevant information effectively during a sign-out can lead to mistakes or delays in medical decision-making that ultimately threaten patient safety.4 Poor quality sign-outs have been associated with adverse events, near miss events, delayed treatment and diagnosis and inefficient use of time.5
Despite the importance of sign-outs for patient care and safety, there appears to be much variation and little standardisation of these sign-outs, even within a specialty at a single institution.6 Previously, we found that only 38% of written sign-outs among our internal medicine residents contained information on the patient's current clinical condition (including symptoms, vital signs, physical exam, laboratory/procedure results or clinical stability), and only 30% of written sign-outs included information from all three categories of current clinical condition, hospital course and tasks to complete.7
Though researchers have examined written sign-out approaches within some specialties,6–11 we are not aware of any studies that have compared sign-outs across specialties. Standardisation of sign-out across specialties may offer the opportunity to improve sign-out quality, strengthen communication between care providers and reduce the potential for error.12 Many articles have advocated for standardisation as an improvement strategy for sign-outs.4 ,6 ,13–16 Furthermore, it is likely that there is a core set of sign-out information needs that spans specialties. Though it may be important to allow structured flexibility, since specialties likely approach sign-out in unique ways, it is important to determine the degree to which specialties agree on the fundamentals.
Since 2007, this institution has had a centralised handoff committee composed of clinicians from multiple departments across the hospital. This committee developed a single standardised sign-out template built into the electronic medical record (EMR) and used by all specialties. The committee also developed handoff curricula for trainees, with common core elements across the institution.17 This study was designed to determine whether the committee's efforts resulted in the presence of a common core set of sign-out standards across specialties, or whether specialty-specific cultures overwhelmed the attempt at institutional standardisation. Therefore, we conducted a cross-sectional analysis of sign-outs from five inpatient specialties at our institution, assessing content, format and whether the sign-outs had been updated within 24 h.
Methods
Setting
Yale-New Haven Hospital (YNHH) is a 966-bed academic medical centre located in New Haven, Connecticut. At the time of our study, YNHH used an EMR system called Sunrise Clinical Manager (Allscripts, Chicago, Illinois, USA). Sign-outs were embedded within this EMR.17 We studied sign-outs from medicine, general surgery, paediatrics, obstetrics and gynaecology. We further subdivided medicine into ‘hospitalist’ and ‘house staff,’ as these teams function independently at YNHH.
Sign-out processes at YNHH differ among specialties, but usually contain verbal and written components. Hospitalists are the exception, as they do not conduct verbal sign-out. Hospitalist teams are comprised of attending physicians, physician's assistants (PAs), and nurse practitioners/advanced practice registered nurses (APRNs). Hospitalist sign-outs are expected to be written initially by the admitting attending. PAs or nurse practitioners/APRNs are expected to update the sign-outs each day. Hospitalists are discouraged from writing ‘nothing to do’ if there are no overnight tasks. Internal medicine house staff teams are comprised of attending physicians, residents, interns and medical students. Residents are expected to write the sign-out initially, but interns or residents can update the sign-out. Verbal sign-out is expected to take place between interns, with residents supervising. On general surgery teams, interns and PAs generally write and update sign-outs. Sign-out usually occurs between an intern and a PA. In paediatrics, interns are expected to write and update sign-outs, though senior residents can update them as well. Interns are expected to lead the verbal sign-out process and residents are expected to supervise. It is expected that sign-outs are updated daily. For obstetrics and gynaecology, interns and residents write and update sign-outs. Residents are expected to present verbal sign-out for gynaecology, while interns and residents are expected to present verbal sign-out for obstetrics, supervised by attendings.
The written sign-out note is embedded within the EMR and includes a common structured template for all specialties. Some specialties have additional specialty-specific fields.17 Some fields (name, location, gender, age, medical record number, visit reason, allergies, weight, admission date, conservator status, care coordination issues and likelihood of being discharged the following day) are automatically inserted from the EMR, while others (primary medical doctor (PMD), history and ‘to do’ list) are free text, requiring data entry. Paediatric sign-outs automatically also include diet, while surgery sign-outs automatically include selected laboratory results. A patient's medications are optional to include when printing the sign-outs.
Any clinician with access to the EMR (including medical students, PAs, APRNs, house staff, fellows and attending physicians) can review and/or modify sign-outs. Once created, a sign-out note remains open for continued editing and revision until the patient is discharged. Consequently, each patient can have only one sign-out note per hospitalisation from any given specialty. However, different specialties can create separate sign-out notes for the same patient. In preparation for verbal sign-out, teams often print a sign-out ‘report’ which includes all sign-out notes for their patients.
Study cohort
We obtained all non-Intensive Care Unit (ICU) written sign-outs from five inpatient services at YNHH on the evening of Wednesday, 18 January 2012. This date was in the middle of the resident work year, the rotation block and the week. We chose to study five inpatient specialties—internal medicine, general surgery, paediatrics, obstetrics and gynaecology—that we felt would best represent a diverse group of general clinical services.
Though we included patients in step-down units, we excluded all patients in ICUs because ICUs often have sign-out systems quite distinct from non-ICU services. We excluded well baby nursery patients because paediatric teams generally do not produce written sign-out notes for these patients.
We included in our study any sign-out note created by the same specialty as the service to which the patient was assigned. We did not count sign-out notes written by consulting specialties.
Measures
We assessed sign-out based on content and format, and whether the sign-outs had been updated within the last 24 h. We defined outcome measures based on existing evaluation tools in the literature, and expert opinion.4 ,5 ,7 ,9 ,10 ,18 ,19 We included whether the sign-out had been updated because shift-to-shift sign-out by definition is intended to be focused primarily on short-term upcoming events and because these are often related to the most recent events of the day. Opportunity for sign-out related adverse events is higher when old, irrelevant information is not removed and when new, important information is not added.4
For content, we determined the presence or absence of several content items: the PMD; diagnosis and/or presenting symptoms; general hospital course (defined as a description of any event occurring prior to sign-out collection date, including medication changes, treatments and operations); new events (defined as a description of any event occurring on the sign-out collection date, including medication changes, treatments and operations); clinical condition (defined as either objective data such as vital signs, physical exam findings, laboratory or procedure results; a description of the patient's stability or trajectory (eg, ‘improved’ or ‘resolved’); or a description of the patient's symptoms); and description of current mental status.
We assessed whether the sign-out contained anticipatory guidance: statements predicting overnight events. We defined these statements as if/then statements or “statements qualifying an “as needed” (PRN) order”. We also examined whether the sign-out contained tasks (assignments for the overnight team), but we excluded the phrase ‘nothing to do.’ We evaluated the text of all anticipatory guidance statements and overnight tasks to calculate frequencies of containing a plan for the predicted event or task, a rationale for that plan, a plan and rationale, or neither.5 For example: ‘If patient requires transfusion (anticipation), please call blood bank (plan), patient has multiple antibodies (rationale).’ To test the reliability of coding, we randomly selected a set of 50 records for reabstraction by a different investigator (LIH), of which 46 had sign-outs available. The κ score for agreement on presence of anticipatory guidance was 0.87 and for presence of tasks was 0.92.
To examine format, we described the major variants of sign-out layout (ie, whether the sign-out contained only prose; whether it listed events by issue; or whether it listed by either date or a combination of issue and date). We also noted the date when the sign-out had last been updated.
We created a composite score based on four elements that we felt defined a comprehensive sign-out, based on the literature,4 ,5 ,7 ,9 ,10 ,18 and that would be applicable across multiple different specialties: updated in the last 24 h, included diagnosis/presenting symptom, included general hospital course, and included clinical condition. We did not include elements such as PMD, medications or laboratory results because our sign-out system automatically incorporates these from the EMR. Sign-outs received 1 point for each of the four elements that they contained. We considered a sign-out with a composite score of 4 to be a comprehensive sign-out.
We looked at several variables to see if they were associated with comprehensiveness of sign-out: specialty; training of the last person who updated the sign-out (such as medical student, APRN, resident or attending), which we used as a proxy for who generally updated/wrote the sign-outs; and days since admission.
The Human Investigation Committee at Yale Medical School approved this study and granted waivers for the Health Insurance Portability and Accountability Act and for patient consent.
Analysis
We assessed the frequency of content elements, format and being updated within 24 h, and tested differences among specialties with χ2 test or Fisher's exact test as appropriate. Using a logistic regression model, we analysed whether a composite score of 4 was associated with specialty, level of training of last updater and days since admission. We used SAS V.9.2 (SAS Institute, Cary, North Carolina, USA) for quantitative analyses. We used p<0.05 as the level of significance. All tests were two-tailed.
Results
Study sample
On the study date there were 654 patients admitted to eligible specialties: 392 medicine, 88 surgery (including trauma, surgical oncology, transplant, endocrine, vascular, emergency general surgery and gastrointestinal), 119 paediatrics, 42 obstetrics and 13 gynaecology. After excluding all ICU patients and well-baby nursery patients, and recategorising patients who had been labelled with the wrong specialty, there were 489 eligible patients: 330 medicine (comprised of 165 hospitalist patients and 165 house-staff patients), 68 surgery, 36 paediatrics, 41 obstetrics and 14 gynaecology. Of these eligible patients, 457 (93%) had sign-out notes (table 1).
Characteristics of study sample
Content
Content elements are shown in table 2. The frequencies of including plan and rationale in anticipatory guidance statements and tasks are shown in figure 1 for medicine only, which comprised the great majority of anticipatory guidance statements and tasks.
Content elements of written sign-outs, by specialty

Proportion of medicine sign-outs including anticipatory guidance and tasks.
We identified several themes for anticipatory guidance statements in the complete dataset. Most anticipatory guidance statements discussed one of the following: what to do if the patient developed a fever; medication recommendations for insomnia, agitation or pain; plan for responding to a change in vital signs; parameters for avoiding nephrotoxic medications in patients with acute kidney injury; and transfusion parameters.
Tasks tended to focus on following up recommendations from consult teams; following up lab results; monitoring for worsening respiratory status and for appropriate overnight fluid intake and output; and ensuring the patient had the appropriate overnight procedure or imaging study. Types of tasks were not appreciably different between specialties except that surgical tasks were most often to conduct a postoperative check on the patient. When we included ‘nothing to do’ as a task, we found that they comprised 45 (51%) of medicine house staff tasks; however, no other specialty used that phrase. Thus, listing ‘nothing to do’ as the task seems to be a pattern specific to medical house staff sign-outs at our institution.
Format
Format varied among specialties. Paediatrics and obstetrics tended to format their sign-outs by issue (89% and 97%, respectively). Surgery was divided between prose only (50%) and other (date or issue/date combination, 47%). Medicine hospitalists used predominantly prose format (96%), while medicine house staff were more evenly divided among the three format groups. Gynaecology contained mostly prose formats (79%).
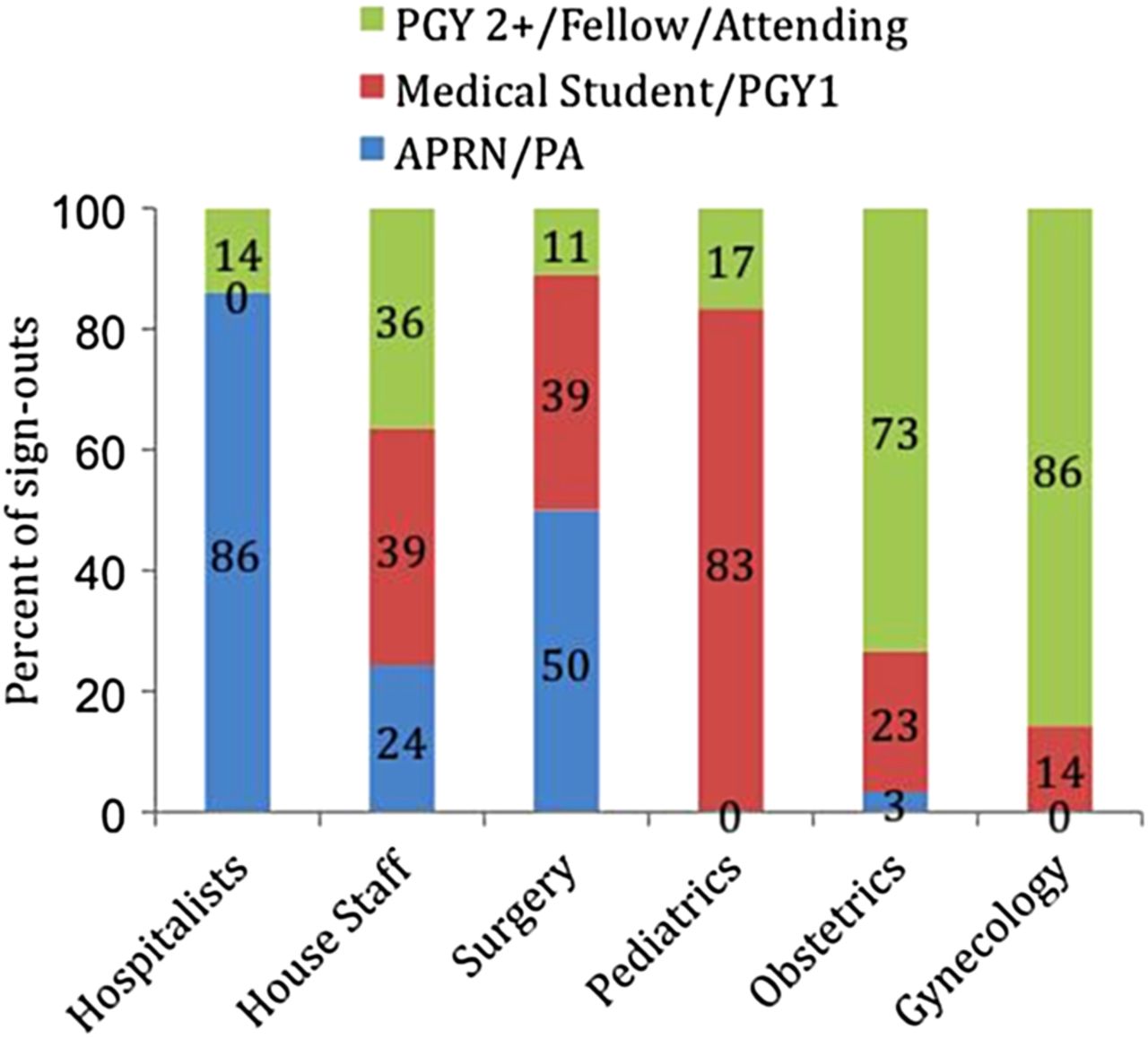
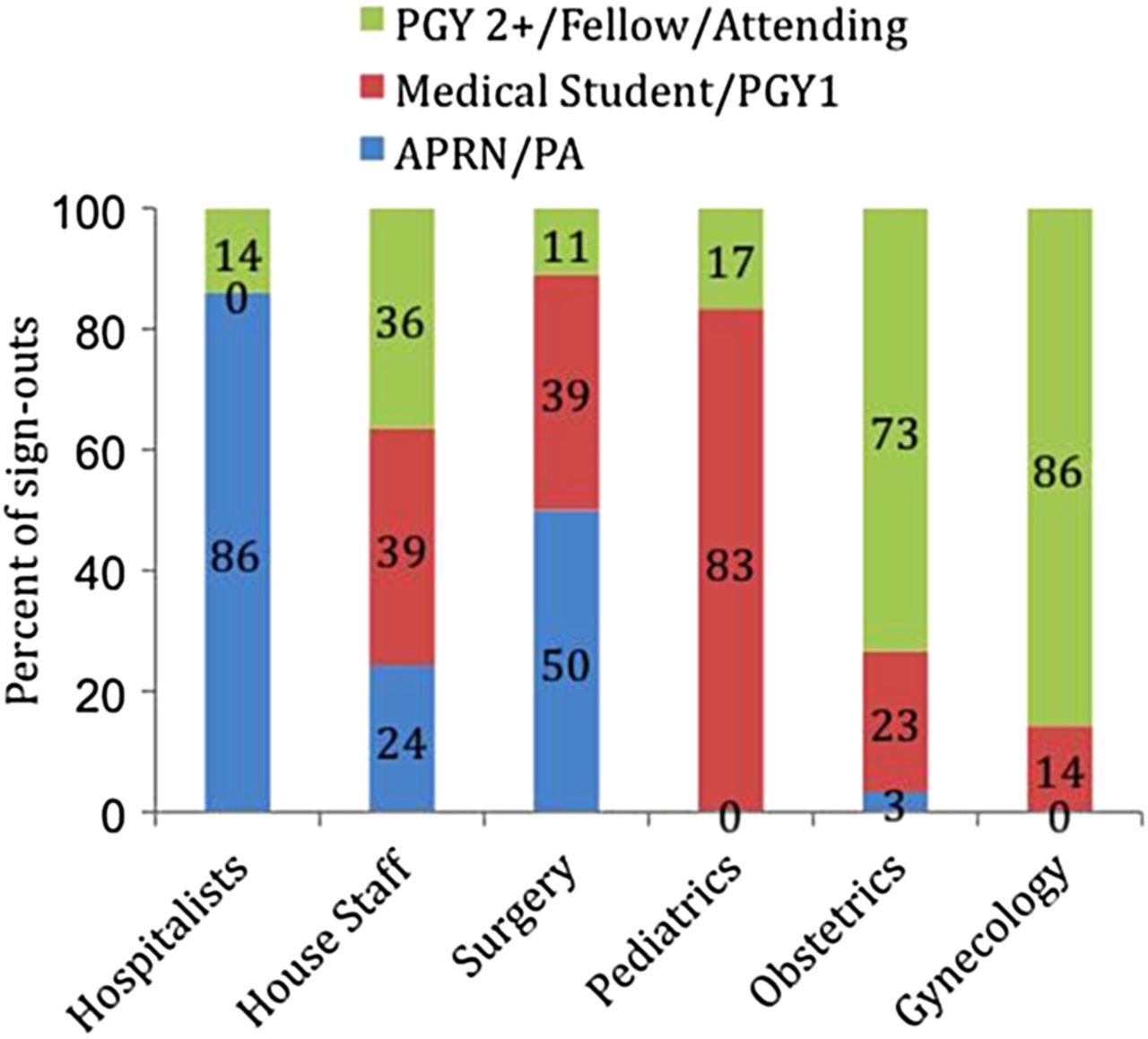
Training of last updater
Training of last updater was used as a proxy to represent the person who most often contributes to the sign-out in each specialty (figure 2). We found variations among specialties and even within specialties; for instance, house staff and surgery were fairly evenly divided among the three training groups.
{kind=link}
{kind=link}
Training of last updater, by specialty. PA, physician's assistants.
Updated
Nearly all sign-outs across specialties (96%) had been updated within 24 h.
Composite score analysis
While 412 (90%) sign-outs across all specialties had at least three elements of our composite score, less than half (49%) of all sign-outs contained all four elements. In addition, no sign-out contained zero elements. Surgery had the lowest percentage of sign-outs with a composite score of 4 (table 3). Compared with surgery, all specialties (with the exception of gynaecology) were significantly more likely to have a composite score of 4. We found that students and post-graduate year (PGY1) trainees were significantly more likely than either other group (RNs/APRNs/PAs and PGY2+trainees/fellows/attendings) to have a composite score of 4. Days since admission was not associated with a composite score of 4.
Multivariate analysis of achieving a composite score of 4
Discussion
In this cross-sectional study, we explored the written sign-out practices of several inpatient specialties. Because YNHH uses a standardised electronic sign-out template across all services with built-in prompts, we predicted that there would be a resemblance among sign-outs in content elements, format and being updated. We found that basic information such as diagnosis and hospital course was included at high rates by nearly all specialties. In addition, most sign-outs in all specialties had been updated within 24 h. Conversely, we found that complex elements, such as clinical condition, anticipatory guidance and tasks, were included at relatively low rates in all specialties despite training and templating. Nonetheless, despite similar overall areas of strength and deficiency, specialties differed significantly from each other in rate of content inclusion. Specialties were also not uniformly superior or inadequate at developing high quality sign-outs. For example, paediatric sign-outs were among the best of all specialties at including information about clinical condition and anticipatory guidance, but were the least likely to include the diagnosis and tasks to complete.
Sign-outs across specialties performed well on many elements, including being updated. It is also important to note that much important content was automatically included (such as demographics, medications, key laboratory results); at other institutions transcribing such content can be very time-consuming and error-prone. However, we found that the sign-outs were weakest about including information that may be considered most important to the sign-out. Sign-outs lacking content elements that require more clinical assessment (such as clinical condition, overnight tasks and anticipatory guidance) are associated with an increased risk of medical errors.5 Complex variables thus are important to include in written sign-outs because they help create a full picture of the patient for the covering team.
Interestingly, our multivariable analysis found that junior trainees (students and interns) were more likely than senior clinicians to include all elements of our composite score. We were surprised by this finding because our previous work showed that senior residents are more likely than interns to generate complex content such as clinical condition or plans for anticipatory guidance during verbal sign-outs.7 It is possible that junior clinicians rely more heavily on written sign-out materials and are consequently more motivated to be comprehensive and thoughtful in constructing them. This finding is worthy of further investigation.
Format varied widely among specialties, and sometimes even within specialties. We do not know whether certain formats are more effective than others, but it may be worth attempting some standardisation of format, at least within specialties. In the same way that clinicians have adopted a uniform method of presenting a patient's history and physical data on rounds so that all team members know what to anticipate during the presentation, standardisation of sign-out format may provide a more efficient and expected way of presenting data to the overnight covering team. For example, we noted that the obstetrics service used a highly structured and consistent format for the free-text section of the sign-out that was entirely obstetrics-specific. In fact, it was not even used by the same house staff when writing gynaecology sign-outs. In effect, this specialty has adopted a ‘structured flexibility’ approach in which elements of the sign-out have been standardised in appropriate areas and at appropriate levels without unnecessarily rigid requirements that a standardisation that works in one setting be applied to a different setting.20 In a similar fashion, the overall sign-out template used at the institution was designed with a structured flexibility approach in mind, in which major content and design elements were standardised (overall print report appearance, automated import of key fields, standardised major topic areas) but written format and specific content items were left open for different specialties to address in their own ways.
Our results for medicine house staff were fairly comparable with those found in similar studies. Horwitz et al21 analysed the sign-out process for medicine house staff at this institution, prior to the implementation of a standardised sign-out template and prior to a sign-out curriculum that is now taught to medicine interns when they begin residency. We found that 81% of written sign-outs included hospital course (defined as any event occurring during hospitalisation, including new events); 39% of sign-outs included clinical condition (defined as in our study); and 99% mentioned whether there were tasks to complete.7 In our present study, we found that 92% of medicine house staff sign-outs included hospital course; 70% of the sign-outs included new events; 59% included clinical condition; and 60% mentioned tasks (30%, excluding ‘nothing to do’). Bump et al9 studied the sign-out process for medicine interns and found that 99% of written sign-outs included general hospital course (similar to our findings); 42% of sign-outs included anticipatory guidance (also similar to our findings); and 90% included tasks. Thus, the biggest difference between our study and the two prior studies was a higher prevalence of clinical condition information but a lower frequency of tasks. These comparisons suggest that medicine house staff training may need to focus more on including tasks in computerised written sign-outs, or at least making it clear when there are no tasks to do.
Our results demonstrated that there were certain differences among specialties, but often consistency within specialties, which suggests that there are specialty-specific cultures regarding written sign-outs. Yet we further found that even within a single specialty, practices were distinct in different settings. For instance, obstetrics and gynaecology are considered separate services but are staffed by the same resident pool. However, there were very different practices between obstetrics and gynaecology regarding update frequency (97% vs 71%, respectively), which likely had a trickle-down effect on variables such as hospital course and new events. Medicine provides another example; hospitalists and house staff varied on several elements such as format, anticipatory guidance and tasks. The medicine hospitalist and house staff teams function independently at YNHH. Their divergent approaches to the written sign-out may be influenced partly by the fact that hospitalists do not do verbal sign-out, and also by the distinct types of training that house staff and PAs/APRNs (whom we found to be the main group updating hospitalist sign-outs) receive.
This study has several limitations. First, as a single-site study at an academic institution it may not be widely generalisable. Our study is cross-sectional and may have been influenced by individual practitioners, especially within smaller fields such as obstetrics and gynaecology. Our study focused on written sign-outs only; thus, some of the components missing in these sign-outs may have been discussed in person during verbal sign-out. Nonetheless, we believe written sign-outs should always contain at the very least the elements in our composite score, as verbal information is not as durable. There are no official standards for how to write a sign-out; however, our assessments were based on numerous reports in the literature and have high face validity. Finally, we did not assess outcomes associated with quality of sign-outs, or accuracy of the content, and therefore cannot draw conclusions about ideal content or format.
In conclusion, we conducted a cross-sectional study at an institution with uniform EMR-based written sign-outs and determined that specialties differed in their approach to the written sign-out even in the presence of standardised templates. We found that there were certain specialty-specific sign-out practices, but that specialty practice varied in different settings. Most sign-outs across all specialties were updated within 24 h and included basic information such as diagnosis and hospital course. Sign-outs less frequently included complex data such as clinical condition, anticipatory guidance and overnight tasks, despite prompts included within the template. Thus, there is a trend across all specialties to report basic patient data and to update sign-outs, but not necessarily to address challenging aspects of a patient's clinical picture or to predict potential overnight events. Given the variability we encountered, we concluded that structured templates alone do not guarantee inclusion of critical content. We support institutional standardisation of the sign-out template but acknowledge that structured flexibility is also necessary. We recommend teaching residents and hospitalists across specialties how to write sign-outs in a way that highlights basic sign-out principles, but that addresses specialty-specific cultures. We suggest assessing the effect of these interventions on effectiveness of sign-outs and on patient outcomes. Future research may focus on comparing sign-outs over time to understand whether there is improvement as more experience is gained.
Acknowledgments
The authors wish to thank Kristina Dzara, Ph.D. for her assistance.
References
Footnotes
Previous presentations An earlier version of this work was presented as an oral presentation at the American Academy on Communication in Healthcare Research & Teaching Forum on 12 October 2012, in Providence, Rhode Island.
-
Contributors The three authors are justifiably credited with authorship, according to the authorship of ICMJE guidelines. Conception and design: ARS and LIH. Analysis and interpretation of the data: ARS, MSA and LIH. Drafting of the manuscript: ARS. Critical revision of the manuscript: MSA and LIH. Final approval given: ARS, MSA, LIH. LIH serves as guarantor.
-
Funding LIH is supported by the National Institute on Aging (K08 AG038336) and by the American Federation for Aging Research through the Paul B Beeson Career Development Award Program. LIH is also a Pepper Scholar with support from the Claude D Pepper Older Americans Independence Center at Yale University School of Medicine (#P30AG021342 NIH/NIA). This project was also supported by the Yale School of Medicine Office of Student Research.
-
Ethics approval Human Investigation Committee, Yale University School of Medicine.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement Data from this study will not be deposited to a repository but may be available in deidentified form upon request to the authors. Contact LIH for information.