Article Text

Abstract
Problem: Ten percent of infants born will require admission to a neonatal facility. Coordinated activity to monitor and improve the quality of care for this high risk, high cost group of infants is considered a high priority. At the time of initiation of this project no system for collection and analysis of neonatal data existed in Northern Ireland.
Design: In 1994 an ongoing prospective centralised data collection system was implemented to facilitate quality improvement and research in neonatal care. We aim to ascertain if there has been a demonstrable improvement in the quality of care provided since the initiation of this system.
Setting: All nine Northern Ireland neonatal intensive care units returned prospectively collected socioeconomic, obstetric and neonatal episode data.
Key measures for improvement: Achievement of the agreed quality indicators relating to transfer patterns, thermoregulation, antenatal steroid administration, and timing of administration of surfactant during the period 1 April 1999 to 31 March 2000 were compared with data for the period 1 April 1994 to 31 March 1996.
Strategies for change: Monitoring included audit and annual feedback of timely clear and relevant data where results were provided confidentially as standardised reports, together with anonymised comparisons with other similar sized units. Draft recommendations were made at regional level and units were asked to adopt finalised consensus guidelines at the local level and to implement changes to clinical practice.
Effects of change: The proportion of transfers taking place in utero increased from 26% to 42% and antenatal steroid administration from 68% to 82%. Normothermia on first admission improved from 66% to 71% for inborn infants. The proportion of infants receiving surfactant where the first dose was given within an hour of birth increased from 13% to 66%.
Lessons learnt: A multiprofessional regional care network can facilitate the development of agreed standards and a culture of regular evaluation leading to quality improvement.
- quality improvement
- neonatal intensive care
Statistics from Altmetric.com
It has been estimated that 10% of infants born will require admission to a neonatal facility and that, overall, approximately 3% will receive neonatal intensive care.1 Although this care is relatively low volume, it remains a significant cost within the health service and, in particular, can be associated with significant mortality and long term morbidity. Coordinated activity to monitor and improve the quality of care is therefore a high priority.
OUTLINE OF PROBLEM
The clinical specialty of neonatology has had a high profile in the development of an evidence base for quality improvement and clinical guidelines through organisations such as the Cochrane Collaboration.2 However, it is also recognised that publication of this information will not in itself lead to effective implementation unless this is applied at a regional and local level in the multiprofessional environment in which care is provided. Neonatal quality improvement networks have been developed to facilitate this process3 and to enhance the translation of research into clinical practice by the monitoring of care provided. Integrated standardised neonatal data collection systems are therefore of fundamental importance if quality improvement is to be achieved. A variety of systems already exist,3 but often require large database management teams and expensive infrastructure. No such system existed in Northern Ireland at the time of initiation of this project.
DESIGN AND SETTING
To address this deficiency, the regional Neonatal Intensive Care Outcomes Research & Evaluation (NICORE) Group was established in 1993. Part of the remit of this multiprofessional group was the establishment of a simple, low cost, centralised, regional data collection system to support quality improvement and research. The group was comprised of representatives from CESDI (now CEMACH), Clinical Genetics, Epidemiology, Midwifery, Neonatology, Nursing, Obstetrics and Gynaecology, Paediatrics and Public Health and therefore, from the outset, a culture of collaboration and local ownership was encouraged. Project leads were also identified and designated in each participating neonatal unit.
The group recognised that assessing the “quality” of care can be fraught with difficulties, particularly if the assessment is predominantly outcome rather than process driven, and concluded that it would be useful to compare the implementation of suitable measures of process such as the appropriate use of treatments that have been shown to be clinically effective.4 Agreement was therefore reached regarding the data items to be collected and the definitions needed to reflect the elements of the potential consensus quality indicators.
All neonatal intensive care units in Northern Ireland agreed prospectively to collect and return this range of sociodemographic, obstetric and neonatal intervention and outcome data items to the central NICORE database. Details of the full set of data collected have been reported previously.5 One NICORE proforma was completed by medical or nursing staff in accordance with agreed guidelines for each infant admitted or readmitted to any neonatal facility for intensive (level 1 or level 2) care6 within the first 4 weeks of life. Each unit was responsible for devising local checking mechanisms to ensure that all appropriate infants were included. In order to facilitate this process, each unit received regular listings of returned proformas from the NICORE coordinator to check against manual or computerised records.
In 1994 the approved data collection system was integrated into the everyday activities of the NIC units and since then has provided regular feedback of reliable, meaningful, and timely information to each unit. This study aims to ascertain whether there have been demonstrable improvements in the quality of the care provided since its implementation by quantifying how well units are reaching agreed targets.
The data were checked, validated, and analysed centrally by the NICORE research staff using the Statistical Package for Social Sciences for Windows (SPSS) version 10 (SPSS Inc, Illinois, USA), where each anonymised record corresponded to one episode of care. Episodes were allocated to financial year according to the date of discharge or death. A baby unique identifier (BUI number) was created centrally which linked episodes of care to each infant and thus allowed tracking across transfers to other neonatal units. This labour intensive process facilitated infant based analyses—for example, ultimate status of final discharge—as opposed to episode based analyses which would look at status on discharge from a single episode of care.
Using the approach suggested by Parry et al,4 the aim of this study was to compare four evidence-based quality indicators for neonatal care between two time periods separated by a number of years during which participating units were provided with regular reports to enable them to undertake local audit and quality improvement activities. The two comparative periods were 1 April 1994 to 31 March 1996 and 1 April 1999 to 31 March 2000.
KEY MEASURES FOR IMPROVEMENT
All relevant literature (research, reviews, and recommendations/guidelines from professional bodies) was appraised in conjunction with expert opinion and local policies for each clinical area identified as an area for potential quality improvement. The four key indicators of quality care were chosen and agreed by the multiprofessional NICORE group from the agreed prospectively collected data items with standarised definitions. Group consensus was obtained over two NICORE meetings with members being requested to identify important indicators for their individual units. A limited number of indicators were selected since quality improvement can usually be most effectively achieved and sustained when approached in an incremental fashion involving smaller steps.
Clinical area 1: Transfer patterns
Measure
The proportion of in utero transfers for first admissions.
Rationale
In utero (prior to the onset of labour) transfer as opposed to postnatal transfer to a neonatal intensive care unit is considered the safest choice7,8 for high risk preterm infants. Delivery of these infants should take place at the regional centre or in a unit with facilities and staffing in accordance with the recommendations of the British Association of Perinatal Medicine (BAPM), following in utero transfer rather than transfer after birth.9
Clinical area 2: Thermoregulation
Measure
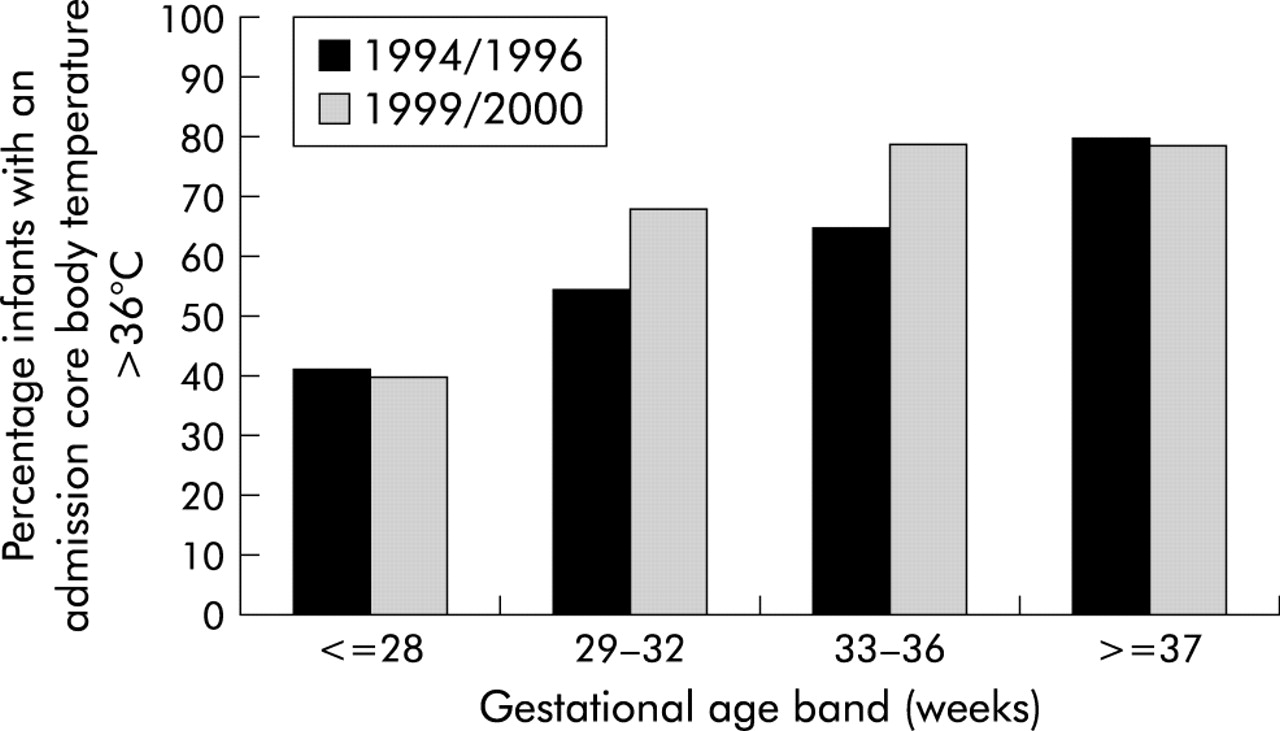
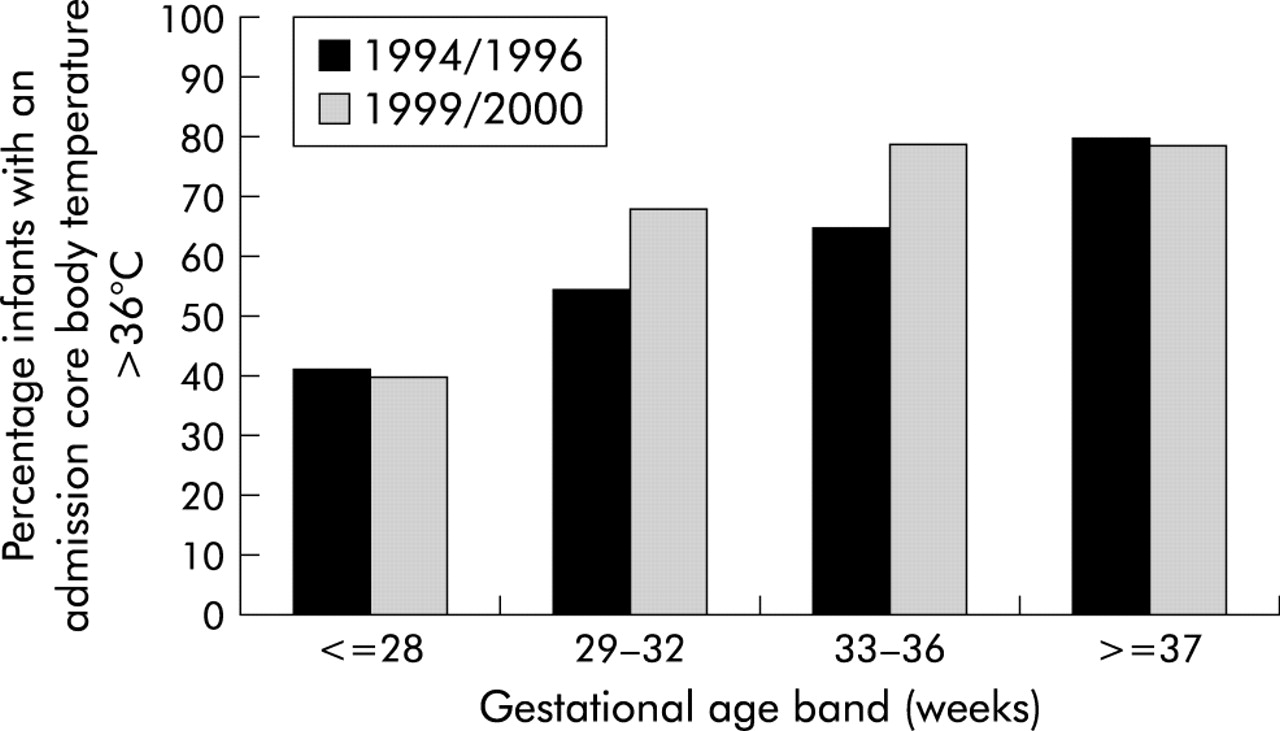
The proportion of inborn infants with an admission core body temperature >36°C.
Rationale
Maintenance of body temperature is very important at the time of birth and during transfer for neonatal care but this still provides a challenge in practice. It has been recommended that admission core body temperature should be >36°C.10
Clinical area 3: Antenatal steroid administration
Measure
The proportion of “at risk” mothers who received at least a partial course of antenatal steroids.
Rationale
The benefits of antenatal steroid administration for babies born at ⩽34 completed weeks’ gestational age are well established both in terms of the reduction of the incidence of respiratory distress syndrome and neonatal mortality.11 80% of women should be able to receive at least a partial course of steroids prior to the delivery of an at risk infant before 35 completed weeks of pregnancy.12
Clinical area 4: Timing of administration of surfactant
Measure
The proportion of infants of <32 completed weeks’ gestational age who received a first dose of surfactant by the age of 1 hour.
Rationale
Administration of surfactant is an important part of the immediate neonatal management of immature infants,13,14 given either to help prevent the development of respiratory distress or as part of the treatment. As further evidence of the benefits of surfactant has accumulated, recommendations have been developed regarding early (prophylactic) treatment of the least mature infants.15
RESULTS FOR THE INITIAL PERIOD 1 APRIL 1994 TO 31 MARCH 1996
Transfer patterns
For first admissions, 473 of 1892 infants (25%) were “transferred in” from another hospital. Of these, 123 (26%) were transferred in utero, 68 (14%) during labour, and 282 (60%) were transferred after birth.
Thermoregulation
For the purpose of this analysis we chose to look at inborn first admissions since this is where health professionals can make a difference by following good practice guidelines for preventing heat loss immediately at birth in the delivery room, particularly for the smaller more vulnerable infants. Each unit also receives feedback on admission temperatures for outborn infants, but this will not be reported here.
For first admissions there were 991 of 1509 inborn infant episodes (66%) where the admission core body temperature of the infant was >36°C. For episodes where the infant was <29 completed week’s gestational age, 63 of 154 (41%) had an admission core body temperature >36°C.
Antenatal steroid administration
At least a partial course of antenatal steroids had been given to 552 of 815 mothers (68%) of infants born at ⩽34 completed weeks’ gestational age.
Timing of administration of surfactant
In this study we chose to look at both the proportion of infants of <32 completed weeks’ gestational age who received surfactant at any time following birth and those where the first dose had been given by the age of 1 hour.
For first admissions, of 419 infants <32 completed weeks’ gestational age, information regarding administration was available in 419, of whom 171 (41%) received surfactant and 22 (13%) received this within 1 hour of birth.
STRATEGIES FOR CHANGE
A founding principle of the NICORE group was that information relating to practice is fed back to the units via the NICORE links and that these data should be timely; easy to understand; relevant; contribute to the decision making processes at local and regional level; make a difference to the quality of care provided (that is, that the information is used); and are widely disseminated (through presentations, peer review publications, etc).
Audit results were provided confidentially to each participating unit as standardised reports, together with individual unit summaries and anonymised comparisons with other similar sized units. These included activity data, mortality and morbidity, together with levels of achievement of the agreed quality standards. NICORE links in each unit acted as facilitators for this ongoing process and reported to the regular meetings of the regional NICORE group.
EFFECTS OF CHANGE
Due to changes in the provision of services in a number of hospitals, NIC was only provided in nine of the 13 original units throughout both study periods.5 These were in four broad groups: the regional perinatal centre, five units providing continuing NIC, two providing short term NIC (until transfer to a larger unit, within hours to a maximum of a few days), and the regional paediatric centre which provides care for neonates primarily with surgical or cardiological conditions.
Activity data for the initial time period 1 April 1994 to 31 March 1996 have been published previously.5 During the 12 month period commencing 1 April 1999 there were 799 episodes of neonatal intensive care provided for 732 infants who fulfilled the criteria for inclusion. This represents approximately 3.5% of the total NI live births for the equivalent time period16 and accounts for 3405 days of level 1 care and 3822 days of level 2 care. These compare with experience in the initial period where 2067 episodes of intensive care were provided for 1948 infants over a 2 year period, amounting to a total of 18 072 days of level 1 and/or level 2 care. This represented 4% of live births during that period.5
Birth weight was ⩽2500 g for 58% (419/724) of infants, with 26% (189/724) weighing ⩽1500 g, compared with 53% (997/1897) and 19% (355/1897) respectively for the initial period (table 1).
Birth weight of infants
OUTCOMES
Between the two periods there was a reduction in overall neonatal mortality in the region from 5.5 per 1000 in 1995 to 3.8 per 1000 in 2000. There were 58 deaths (1999/2000), giving an overall mortality rate of 8%. The final outcome was not recorded in eight cases. Mortality increased rapidly with decreasing gestational age below 28 weeks (fig 1). Congenital malformations were detected in 110 infants (15%), 27 of whom died. This represents almost half of the total deaths.

Percentage survival against gestational age (1999/2000).
RESULTS FOR THE PERIOD 1 APRIL 1999 TO 31 MARCH 2000 AND COMPARISON WITH THE PERIOD 1994/1996
The performance of each unit in relation to the agreed quality indicators was assessed and overall results were tested for statistical significance by comparing the two time periods using the χ2 test.
Transfer patterns
For first admissions, of the 726 of 732 episodes where transfer status was recorded, no transfer occurred in 502 (69%). There were a total of 224 transfers (31%) of which 103 (46%) took place after birth, 28 (13%) during labour, and 93 (42%) before the onset of labour (in utero). The overall proportion of infants transferred increased significantly from 25% in the previous time period to 31% (χ2 = 9.2, df = 1, p<0.05). The proportions within the transfers were also altered with in utero transfers increasing from 26% to 42% (χ2 = 17.1, df = 1, p<0.001) while transfers after birth were reduced from 60% to 46% (χ2 = 11.4, df = 1, p = 0.001). Transfers during labour did not change significantly.
Thermoregulation
Comparison of admission temperature between the two periods shows an increase in infant episodes where the standard of an admission core body temperature >36°C was achieved from 66% to 71% (410 of 580) for inborn infants (χ2 = 4.8, df = 1, p<0.05). For infants <29 completed weeks’ gestational age the results were not improved (41%, 63 of 154; fig 2).
{kind=link}
{kind=link}
Achievement of admission temperature standard for inborn infants (for first admissions) over the two study time periods.
Antenatal steroid administration
Antenatal steroids had been given to 296 of 360 mothers (82%) where the infant was born at ⩽34 completed weeks’ gestational age. This is a significant increase from 68% in the earlier time period (χ2 = 26.1, df = 1, p<0.001). The improvement in antenatal steroid administration was mainly through administration to mothers where the membranes had not been ruptured for more than 1 day.
Timing of administration of surfactant
For first admissions, of 205 infants <32 completed weeks’ gestational age, information regarding administration was available in 194, of whom 105 (54%) received surfactant. For the 92 infants where information regarding time of administration was available, this showed a significant increase in the proportion where the first dose was received within 1 hour of birth from 13% to 66% (61 of 92; χ2 = 79.1, df = 1, p<0.001).
LESSONS LEARNT AND NEXT STEPS
In this study we have shown significant improvements in a number of indicators of the quality of neonatal intensive care. While other factors in addition to our intervention may have influenced practice, the improvements were consistent across standards and feedback from the participating units has highlighted the usefulness and impact of both the ongoing data collection and regular feedback of results. A major contributing factor to the improvement in care has been the agreement and dissemination of key indicators and the increased awareness of these among clinicians. This was encouraged by bringing the representatives from the participating units together regularly every few months to discuss the project and their local experience. Feedback to each unit via the annual standardised NICORE reports has allowed staff to quantify how well they are reaching agreed targets, to initiate local strategies for change, and to reassess the situation annually. An example of these reports can be seen in the online supplement available at http://www.qshc.com/supplemental. Each unit is now also given an opportunity to report on local quality improvement initiatives in subsequent annual reports. An example of this was the identification by one participating unit that there appeared to be a significant incidence of at-risk infants whose eyes were not being examined for retinopathy of prematurity at the appropriate time. Further local audit revealed that, where infants were transferred out to another unit or discharged home before this time, it was possible that the necessary arrangements were not always being made for review. A local protocol was developed to deal with this and subsequent re-audit demonstrated effective implementation. This experience was then shared with the network.
It is important that this monitoring process is not seen as punitive but as a regional collaboration with those engaged in the provision of care, often within limited resources of personnel, time and finance. As such it provides a basis for local activities which can be targeted to address issues of particular relevance to each unit, and so engender the support and commitment which is essential at the local level to result in effective and sustainable change.
While these results demonstrate an overall improvement between the two data collection periods, they also highlight the continuing problems faced by the very preterm infant. For example, almost half of all transfers still take place after birth, and this highlights the urgent need for a regional neonatal transport network. Also, for infants of <29 completed weeks’ gestational age, admission temperatures have not improved although published work has suggested ways in which changes can be made to address this.17
When embarking on a project such as this it is crucial to remember that time spent at the planning stages will help ensure smooth implementation. This planning includes notifying all stakeholders, identifying unit leads, resolving individual concerns locally, highlighting benefits of participation, and slowly dissolving barriers to change. All relevant parties should be involved in the early stages and also continue to participate so that a sense of local ownership is nurtured and good relationships can evolve over time. It is important that the multiprofessional nature of the provision of care is reflected in the range of those involved and in the membership of the steering group. Not only is it important to collect appropriate data, but it is also beneficial to discuss how these data will be collected, analysed, and fed back to the individual units in a clear and concise format. Some barriers to the data collection process were identified. For example, time constraints and workload of neonatal staff tend to result in a feeling of “not another audit form”. This was anticipated and pre-empted by (1) explaining the rationale for this through the identified link persons in each participating unit, (2) reaching agreement to this dataset through discussions of the regional group, and (3) limiting the number of data items in the first instance mainly to those essential to the analysis and feedback of important clinical areas.
CONCLUSION
In our experience the success of this work has occurred through effective quality improvement activities agreed and implemented at the local level in individual units. This is supported by a network of health professionals who complete and coordinate the data collection on a voluntary basis and the commitment of the NICORE group and the funding bodies who have provided support.
Key messages
A multiprofessional regional quality improvement network:
-
facilitates the development of evidence-based clinical standards;
-
provides the framework for a culture of regular evaluation leading to improvements in the quality of care provided;
-
requires adequate funding if quality improvement is to be sustained;
-
depends on regional and local commitment of key stakeholders at all stages.
We have identified areas of concern where further work needs to be carried out, particularly in the prevention of hypothermia. Based on the work reported here, the NICORE group has been instrumental in establishing an all-Ireland neonatal intensive care quality improvement network and in obtaining funding for further quality improvement projects. Current projects include reducing nosocomial infections, timing of surfactant administration, and timing of elective caesarean sections. In addition, funds have been made available to purchase a data management system for the neonatal units. This has been tailored to meet the needs of the NICORE dataset and reporting system including the collection and export of predefined data to the Vermont Oxford Network expanded dataset which will allow international benchmarking.18,19 This user friendly system will allow quick on-site access and analysis of unit data and hence ongoing monitoring of established and future quality standards.
However, in the long term the effective contribution of this type of work to improvement in care can only be fulfilled if adequate resources are made available for the development and maintenance of high quality clinical databases.20 This is an issue which must be recognised as high priority by those involved in service planning and commissioning at the national and regional level.
Acknowledgments
The authors and members of NICORE thank the units who contributed information to this study: Altnagelvin Hospital, Antrim Hospital, Craigavon Hospital, Daisy Hill Hospital, Downpatrick Hospital, Erne Hospital, Jubilee Maternity Hospital, Lagan Valley Hospital, Mid Ulster Hospital, Royal Belfast Hospital for Sick Children, Royal Maternity Hospital, Route Hospital, Ulster Hospital. Particular thanks are due to the coordinators on each site for their invaluable support in the timely completion and return of data. They also thank Terry Falconer, CESDI Project Manager, for providing additional denominator data.
REFERENCES
Supplementary materials
The table is available as a downloadable PDF (printer friendly file).
If you do not have Adobe Reader installed on your computer,
you can download this free-of-charge, please Click hereFiles in this Data Supplement:
- [view PDF] - NICORE individual hospital summary information.
Footnotes
-
Membership of NICORE Steering Group: Dr F Alderdice, Lecturer in Health Sciences; Dr C Beattie, Consultant in Public Health Medicine; Dr A Bell, Consultant Paediatrician; Dr D Brown, Consultant Paediatrician; Dr C Corkey, Consultant Paediatrician; Dr J Dornan, Consultant Obstetrician and Gynaecologist; Sr P Farrell, Senior Neonatal Nurse; Dr C Halahakoon, Consultant Paediatrician; Dr M Hogan, Consultant Paediatrician; Dr J Jenkins, NICORE Chairman, Senior Lecturer in Child Health and Consultant Paediatrician; Dr J Larkin, Paediatric Specialist Registrar; Ms E McCall, Research Assistant; Professor G McClure, Professor of Neonatal Medicine; Dr R McMillen, Consultant Obstetrician and Gynaecologist; Dr M O’Hare, Consultant Obstetrician and Gynaecologist; Dr M Reid, Consultant Paediatrician; Dr M Scott, Regional Coordinator CESDI; Dr F Stewart, Consultant Clinical Geneticist; Dr S Tharmaratnan, Consultant Obstetrician and Gynaecologist.JJ, FA and EMcC have all participated in the collection, analysis and writing of this study and act as guarantors for the paper.
-
Funding: Department of Health, Social Services and Public Safety, Northern Ireland Mother and Baby Appeal Fund (NIMBA), MRC and R&D Northern Ireland for F Alderdice Fellowship.
-
Competing interests: none
Linked Articles
- Quality Line