Article Text

Abstract
Background: Most nationally standardised quality measures use widely accepted evidence-based processes as their foundation, but the discharge instruction component of the United States standards of Joint Commission on Accreditation of Healthcare Organizations heart failure core measure appears to be based on expert opinion alone.
Objective: To determine whether documentation of compliance with any or all of the six required discharge instructions is correlated with readmissions to hospital or mortality.
Research design: A retrospective study at a single tertiary care hospital was conducted on randomly sampled patients hospitalised for heart failure from July 2002 to September 2003.
Participants: Applying the Joint Commission on Accreditation of Healthcare Organizations criteria, 782 of 1121 patients were found eligible to receive discharge instructions. Eligibility was determined by age, principal diagnosis codes and discharge status codes.
Measures: The primary outcome measures are time to death and time to readmission for heart failure or readmission for any cause and time to death.
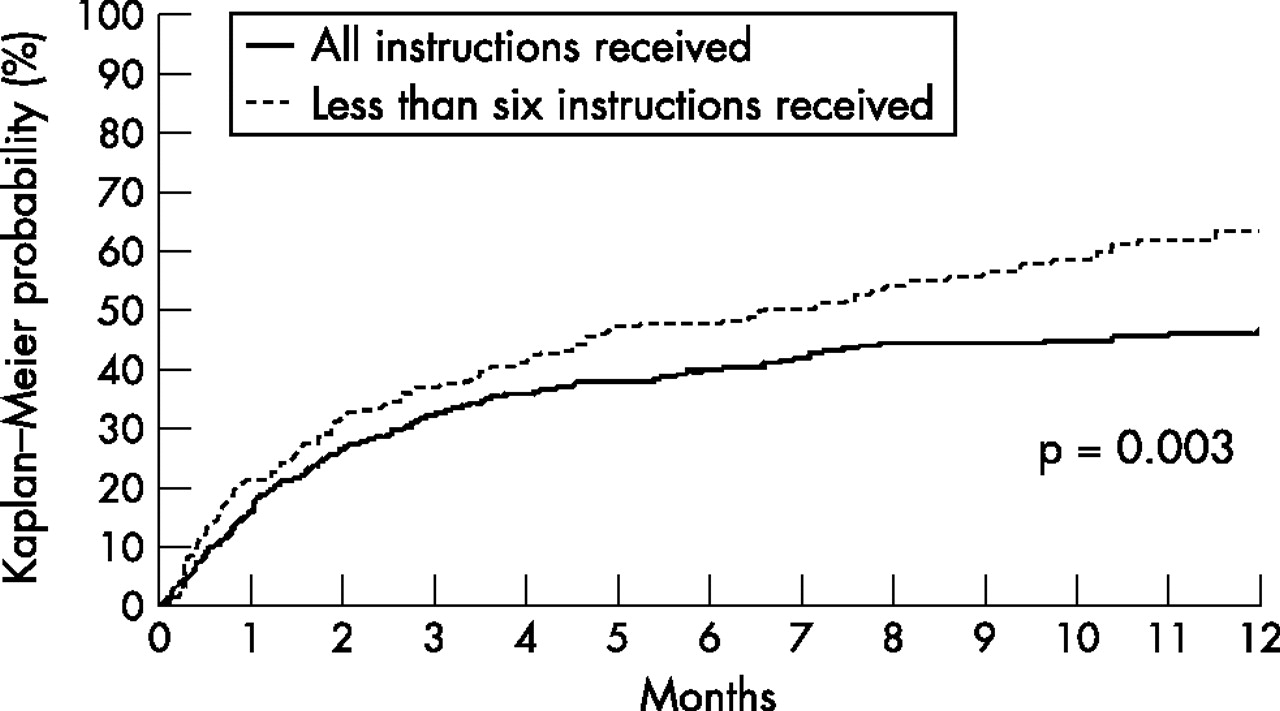
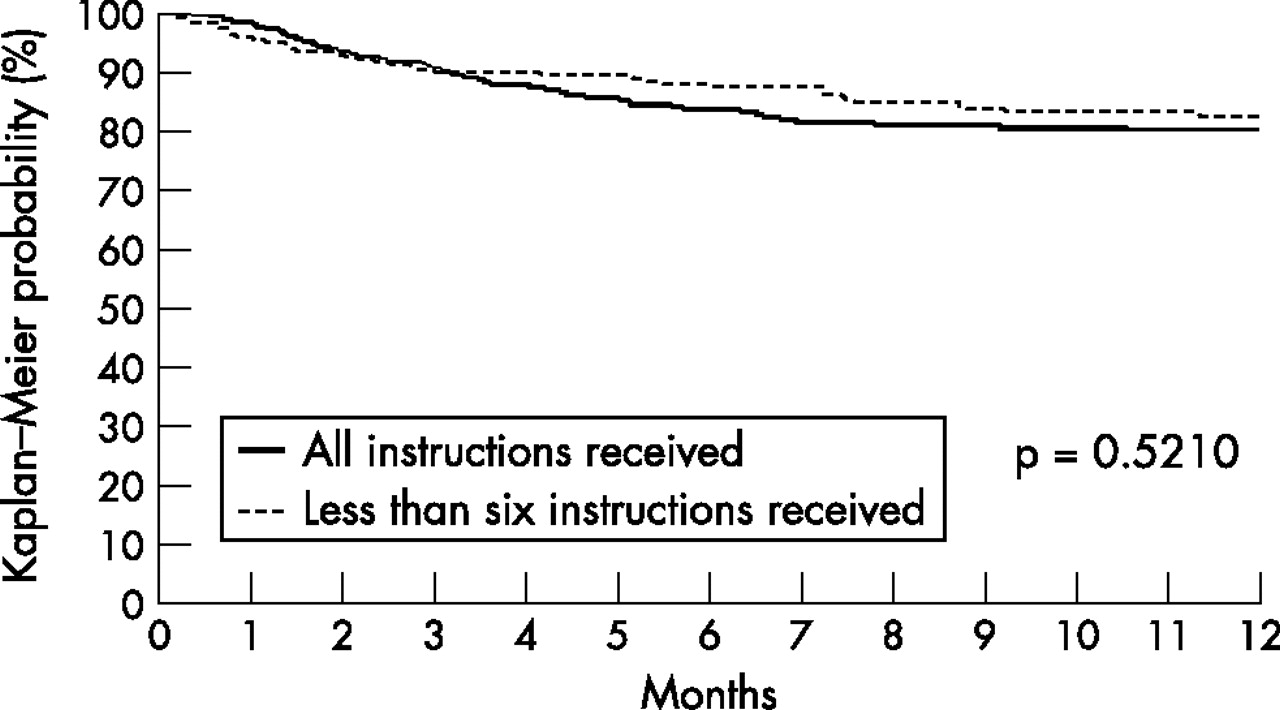
Results: In all, 68% of patients received all instructions, whereas 6% received no instructions. Patients who received all instructions were significantly less likely to be readmitted for any cause (p = 0.003) and for heart failure (p = 0.035) than those who missed at least one type of instruction. Documentation of discharge instructions is correlated with reduced readmission rates. However, there was no association between documentation of discharge instructions and mortality (p = 0.521).
Conclusions: Including discharge instructions among other evidence-based heart failure core measures appears justified.
- ACEI, angiotensin-converting enzyme inhibitor
- LVF, left ventricular function
Statistics from Altmetric.com
Healthcare organisations commit considerable financial and personnel resources to collect information and modify their healthcare delivery systems in response to mandated quality metrics required by the government, private payers, credentialling organisations, and public reporting agencies. The use of some of these quality measures is supported by peer-reviewed studies which provide evidence of association of the measure with clinical outcomes. Other measures appear to be based only on professional opinion or consensus. Recent emphasis on evidence-based medicine and practice is consistent with the use of quality measures shown to be associated with desirable health outcomes or states.1
Hospitals in the United States, accredited by the Joint Commission on Accreditation of Healthcare Organizations, are required to assess quality using prescribed measures called core measures for specific diseases. Heart failure is one of the diseases that a hospital can choose to assess. Three of the Joint Commission’s heart failure core measures are evidence-based: assessment of left ventricular function (LVF), prescription of angiotensin-converting enzyme inhibitor (ACEI) and provision of adult smoking cessation advice/counselling. A fourth measure, however, appears to be based only on consensus opinion or professional judgement. The consensus-based discharge instruction metric requires documentation that patients received written discharge instructions or educational materials in six categories: activity, weight, diet, discharge medications, follow-up appointment and worsening symptoms.2,3 However, evidence to support the efficacy of this practice is limited. Heart failure discharge instructions are a non-pharmacological therapy that has been accepted by expert consensus and incorporated into multidisciplinary disease management processes.4
Expert opinion or consensus is frequently used in decision making in healthcare, and intuitive insights can seem unchallengeable (“everyone knows this”); studies in social and cognitive psychology repeatedly show that consensus can be misleading. Although all may agree or even know that patient education and discharge instructions are good, the measure under consideration is not the actual receipt but documentation of the receipt of specific information by patients. The quality of instruction or education is not directly assessed, nor is it clear that all patients with heart failure require such information on all visits.
Fortunately, to produce a usable indicator of quality or performance, not every dimension needs to be accurately defined, studied and accepted. Depending on its use, an indicator that is closely associated with some desired event or outcome can be sufficient. Such an indicator could be an acceptable proxy measure of quality.
The purpose of this study was to determine whether time to readmission and survival time among patients with heart failure are associated with delivery of the six heart failure discharge instructions as reflected in the medical record.
STUDY DESIGN
Administrative and medical record data for this retrospective study were obtained from discharges at Saint Marys Hospital, a tertiary care academic centre, in Rochester, Minnesota. Patients hospitalised for heart failure from July 2002 to September 2003 were eligible for sampling. Seventy five charts were randomly chosen from each month’s discharges, which yielded a sample of 1121 patients discharged with a principal diagnosis of heart failure. Of these 1121 patients, 782 patients met the Joint Commission criteria to receive discharge instructions. Eligibility was determined by age, principal diagnosis codes and discharge status codes. Patients ⩾18 years of age with a principal diagnosis of heart failure, hypertensive heart disease with heart failure, or hypertensive heart and renal disease with heart failure (International Classifications of Disease, Ninth Revision, Clinical Modification codes 428, 402 or 404, respectively) and discharged to home, home care or home care with intravenous treatment were included. Patients discharged to skilled nursing facilities or other acute-care hospitals were excluded.
Using an administrative file which includes reports of all statewide deaths as well as other reports of patient deaths, records were assessed for hospital readmission or death from initial discharge up to 31 October 2003. Readmissions were classified into heart failure related and unrelated causes. Patients in all stages of heart failure were included. Registered nurses reviewed the medical records to determine the extent of compliance with the documentation of written discharge instructions. Additional collected data included patient’s age, sex, and zip code of residence, admission source, compliance with LVF assessment, and ACEI prescription at discharge, discharge disposition, disease severity based on all patient refined diagnosis-related groups,5 and level of comorbidity using the component diseases in the Charlson index.6,7 Other evidence-based guidelines, LVF assessment and ACEI prescription, were assessed in the Joint Commission heart failure core measures. These guidelines were included as variables to determine whether any association with outcomes was due to adherence to these guidelines or the documentation of discharge instructions. In compliance with the Mayo Clinic Institutional Review Board and state of Minnesota regulations, any patient who had not authorised access to his or her medical record for review for research purposes was excluded.
Statistical analysis
Associations between documentation of discharge instructions and the time of readmission to hospital and death were described using Kaplan–Meier survival methods and assessed univariately using log-rank tests. Analyses were performed for both any readmission and only readmission for heart failure (figs 1 and 2). Associations between compliance with discharge instructions and compliance with the evidence-based measures were assessed using χ2 tests. Multivariable Cox regression models were developed to assess the effects of discharge instructions, adjusting for other patient factors. Potential covariates included patient demographics, severity of illness, distance from Rochester, discharge disposition, compliance with other Joint Commission core measures and comorbidities.

Probability of readmission for any reason (p = 0.003).
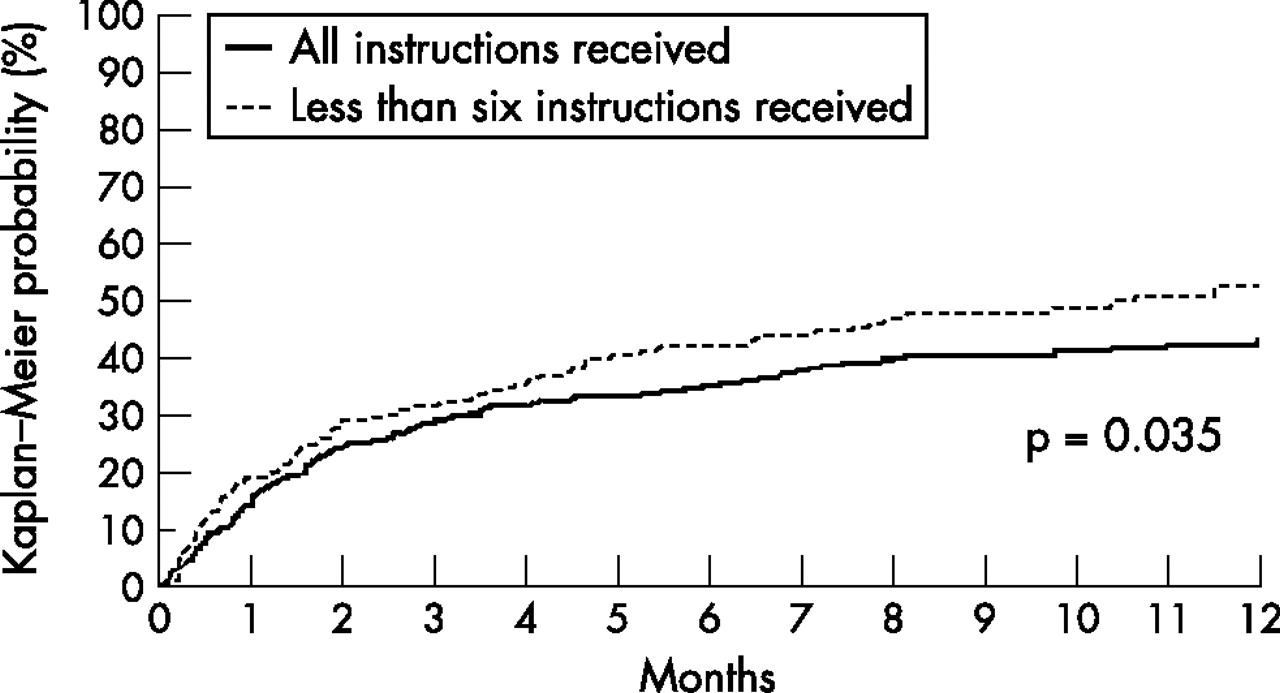
Probability of readmission for heart failure (p = 0.035).
The relative importance of the components of discharge instructions was based on a Cox regression model including important covariates and considering each discharge instruction component in a stepwise fashion. A dose–response assessment of the documentation of discharge instructions was based on a multivariate Cox regression model where the number of components were evaluated in lieu of the indicator that all instructions were provided. Data were not readily available on patient-perceived health status or support at home.
Principal findings
Assessment of the documentation of individual instruction types found that patients received drug instructions the most (91%) and weight monitoring instructions the least (70%). In all, 68% (532 of 782) of eligible patients had documentation of receiving all six types of instructions, and 6% (15 of 250) of patients had no documentation of any of the types of instructions. The most frequent combinations of instructions types not received involved activity, weight and symptoms. Only one of the eligible patients was excluded from the LVF assessment measure, and only one of those patients did not have qualifying documentation for the assessment. Also, 436 (56%) patients had left ventricle dysfunction and qualified for the ACEI prescription at discharge measure.
Although the percentage of patients with documentation of all of the discharge instructions was higher among the patients who had ACEI prescriptions (76%; 237 of 310) than among those without ACEI prescriptions (69%; 87 of 126), this difference was not statistically significant (p = 0.109). Interestingly, documentation of discharge instructions was considerably lower among patients without left ventricle dysfunction (60%; 208 of 346; p<0.001).
Figures 1 and 2 show the Kaplan–Meier curves of time to readmission for heart failure and time to readmission for any cause. Overall, 9% of patients were readmitted for heart failure within 14 days, 16% within 30 days, 29% within 60 days and 37% within 90 days. Similarly, readmissions for any cause were 10%, 18%, 31% and 41% at 14, 30, 60 and 90 days after discharge, respectively. Figure 3 shows the survival time to death curves. Note that survival time to death is assessed irrespective of readmission status. Overall, 292 patients were known to have died; 116 of these patients died before any readmission in our system. There was no statistically significant association between documentation of discharge instructions and survival (p = 0.521).

{kind=link}
{kind=link}
{kind=link}
Survival time to death from any cause (p = 0.521).
Table 1 presents the results of univariate analysis on the association of documentation of type of discharge instruction with readmission. Patients with all instructions were significantly less likely to be readmitted for both any cause (p = 0.003) and readmission for heart failure (p = 0.035; table 2) than those who were missing documentation of at least one type of discharge instruction. Missing instructions on activity appeared to have the biggest effect on time to readmission for both heart failure-related and all readmissions. There appears to be a dose–response relationship in that patients who received more of the six components have longer times to readmission for both readmissions due to any cause (p = 0.004) and heart failure (p = 0.042); the higher the number of components, the longer the time to readmission. Renal disease, geographical distance from our institution and all patient refined diagnosis-related groups weight were all independently associated with time to readmission (table 3). Documentation of all discharge instructions (whether considered as an indicator or as a number of components) was still significantly associated with time to any readmission (p = 0.011 and 0.026) and had some association with time to heart failure readmission (p = 0.078 and 0.105) in Cox regression models incorporating the important covariates. The ACEI measure was not associated with time to any readmission (p = 0.407) but had some association with time to readmission for heart failure (p = 0.072).
Univariate assessment of time to readmission by discharge instruction category (n = 783)
Statistical results of association of increased time to readmission with receiving all heart failure discharge instructions compared with missing at least one instruction
Results of multivariable Cox regression model for time to readmission for any reason
DISCUSSION
Documentation of compliance with the discharge instruction component of the heart failure core measure was associated with a decreased rate of readmission. Significant associations were seen between discharge instructions for patients with heart failure and time free of readmission, particularly with instructions on activities. Providing patients with comprehensive discharge instructions seems to contribute to keeping patients with heart failure out of hospital, for both heart failure and any cause, and may be a valid approach in preventing readmissions to the hospital. Although these results are obtained in the US, they can be generalised to other healthcare systems if the same evidence-based standards are part of the regimen of care for patients with heart failure. Interventions to decrease early readmissions or death among patients with heart failure should target both medical management and the adequacy of support systems. These interventions probably need to be applied to all patients who are admitted.8
When it comes to delaying readmissions, discharge instructions appear to have an effect over and above any effect of prescribing ACEI. Although initially not based on solid evidence, the core measure assessing the documentation of these instructions is associated with an indicator of higher quality, longer time to readmission.
Our results with regard to the relative frequency and types of instructions documented as received were consistent with other studies on patients with heart failure. Patients received information about drug compliance with the greatest frequency and about weight monitoring with the lowest frequency.9,10 Vinson et al.11 identified non-compliance with drugs and with diet, inadequate follow-up, failed support system and failure to seek medical help with re-occurring symptoms as causes for preventable readmissions for heart failure. Chin and Goldman8 found that 21% of admissions for heart failure were due to non-compliance with diet and drugs. We found that the absence of documented information about activity seemed to have a role in readmissions. Our finding of a 41% probability of readmission within 90 days for any cause is similar to that of patients enrolled in a multidisciplinary case management approach to reduce readmissions for heart failure.12
Limitations
Our study has several limitations. Discharge instructions may have been given to patients but not documented. Documentation of discharge instruction requires an extra step in our medical record system, which may represent a barrier to consistent documentation. Since the end of the study period, steps have been taken to standardise and to simplify the process of documenting discharge instructions. In our study, it is unclear whether the discharge instructions themselves result in lower mortality and readmissions or whether the documentation of instructions is a surrogate indicator for some other intervention such as higher quality nursing care that actually results in lower rates. There could also be some patient factors such as perceived mental cognition and social environment associated with both documentation of discharge instructions and higher readmission rates.
Box 1 Joint Commission on Accreditation of Health Care Organization, United States standards—heart failure core measures*
HF-1 discharge instructions
Patients with heart failure discharged home with written instructions or educational material given to the patient or to the care giver at discharge or during hospital stay, considering all of the following activities: activity level, diet, discharge drugs, follow-up appointment, weight monitoring and what to do if symptoms worsen.
HF-2 LVF assessment
Patients with heart failure with documentation in the hospital record that LVF was assessed before arrival, during hospitalisation or is planned for after discharge.
HF-3† ACEI for LVSD
Patients with heart failure with left ventricular systolic dysfunction and without ACEI contraindications who are prescribed an ACEI at hospital discharge. For the purpose of this measure, left ventricular systolic dysfunction is defined as chart documentation of a left ventricular ejection fraction <40% or a narrative description of LVF consistent with moderate or severe systolic dysfunction.
HF-4 adult smoking cessation advice or counseling
Patients with heart failure with a history of smoking cigarettes who are given smoking cessation advice or counseling during the hospital stay. For the purposes of this measure, a smoker is defined as someone who has smoked cigarettes anytime during the year before arrival to hospital.
The generalisability of our study may be limited if the population is not typical of other hospitals. To deal with this issue, we stratified our sample into patients residing within 50 miles and those who travelled at least this distance for care. Even though patients from far away places had fewer readmissions to our facility, the effect of discharge instructions on readmission was consistent between the groups with lower readmissions among those receiving instructions. Given its status as a major academic referral centre, Saint Marys Hospital may treat a disproportionate number of more critically ill patients. Additionally, patients may be readmitted to other hospitals closer to home after discharge. Unlike most studies on readmission for heart failure, we did not stratify patients by heart failure classification or clinical criteria. However, when compared with these types of studies, our readmission rates are similar but with a lower rate for any cause. In a study by Harjai et al13 26.2% of patients with heart failure were readmitted within 30 days for any cause and 15.8% were readmitted for heart failure.
There are likely many other factors which influence readmission that are not dealt with by the heart failure core measures. The fact that we had no active follow-up of all patients may have understated the death rate. Our source did include a report of all death certificates from Minnesota (66.4% of patients). We believe that undercounted deaths would likely not affect the relationship with discharge instructions. Additionally, other outcomes which may reflect different aspects of quality of care were not assessed. Further studies are needed to examine the additional aspects of both hospital care and care after discharge for patients with heart failure, to determine the best practices that should be endorsed to assure the highest quality of care.
CONCLUSION
This study presents stronger evidence for the use of discharge instructions as an evidence-based measure than has been produced previously. Documentation of discharge information and patient education does appear, in fact, to be associated with reductions in both mortality and readmissions. The inclusion of this measure in the set of core measures on heart failure among other evidence-based measures appears justified.
Acknowledgments
We thank Amy Wagie, BS for statistical analysis support, Marlené Boyd for administrative assistance, Debra Hernke, RN for acting as a reviewer and Gordon Mosser for his comments on the draft of this paper.