Article Text

Abstract
Objective: To determine the efficacy of a computerised decision aid in patients with atrial fibrillation making decisions on whether to take warfarin or aspirin therapy.
Design: Two-armed open exploratory randomised controlled trial.
Setting: Two research clinics deriving participants from general practices in Northeast England.
Participants: 109 patients with atrial fibrillation aged over 60.
Interventions: Computerised decision aid applied in shared decision-making clinic compared to evidence-based paper guidelines applied as direct advice.
Main outcome measures: Primary outcome measure was the decision conflict scale. Secondary outcome measures included anxiety, knowledge, decision-making preference, treatment decision, use of primary and secondary care services and health outcomes.
Results: Decision conflict was lower in the computerised decision aid group immediately after the clinic; mean difference −0.18 (95% CI −0.34 to −0.01). Participants in this group not already on warfarin were much less likely to start warfarin than those in the guidelines arm (4/16, 25% compared to the guidelines group 15/16, 93.8%, RR 0.27, 95% CI 0.11 to 0.63).
Conclusions: Decision conflict was lower immediately following the use of a computerised decision aid in a shared decision-making consultation than immediately following direct doctor-led advice based on paper guidelines. Furthermore, participants in the computerised decision aid group were significantly much less likely to start warfarin than those in the guidelines arm. The results show that such an approach has a positive impact on decision conflict comparable to other studies of decision aids, but also reduces the uptake of a clinically effective treatment that may have important implications for health outcomes.
- DCS, decision conflict scale
Statistics from Altmetric.com
Patients increasingly expect to be actively involved in decision-making about their own medical care1 and health policy reflects this.2 Increasing emphasis is placed upon shared decision-making, especially where decisions require an evaluation of potential trade-offs between benefits and harms of alternative treatments.3
A systematic review of the effectiveness of decision aids concludes that they can help patients participate in decision-making and make informed choices consistent with their values by presenting the clinical evidence and the likely effects of alternative treatments. Decision aids also improve patients’ knowledge, reduce decision conflict and engage patients more actively in decision-making, but have little impact on patient satisfaction, and a variable impact on the actual decisions made.4
Shared decision-making may be of value in the treatment of patients with atrial fibrillation to prevent stroke. Atrial fibrillation affects almost 5% of people over the age of 65 and approximately 10% of men over 75.5 It increases the risk of stroke by about fivefold and this risk can be reduced by 68% by warfarin anticoagulation and to a lesser extent by aspirin.6 Warfarin and aspirin also have markedly different profiles of harm, with the risk of major bleed being the predominant concern with warfarin treatment, exacerbated by interactions with lifestyle, diet and other drug therapies.
The aim of this exploratory trial was to determine the efficacy of a computerised decision aid compared to the standard use of clinical guidelines derived from the same decision analysis7 in patients with atrial fibrillation making decisions on whether to take warfarin or aspirin therapy. We also explored the impact and process using observational methods (see Murtagh et al8). The null hypothesis was that the computerised decision aid applied in a shared decision-making consultation would not lead to lower decision conflict than traditional application of doctor led guidelines and advice.
METHODS
This study began as a three-armed open, randomised controlled efficacy trial supported by an observational study which included video recording of consultations and post-consultation interviews. Building on previously developed evaluative guidelines we designed and piloted two different versions of a decision aid.7,9 Both versions included individualised risk and benefit presentation and a section to support shared decision-making. One version used explicit value elicitation employing the standard gamble method and a Markov decision analysis (“explicit tool”), the other included only the risk/benefit presentation (“implicit tool”). Early in the trial, the observational study showed that participants in the explicit arm found the elicitation of utilities using the standard gamble to be difficult, so this arm was discontinued (see Murtagh et al).8 This paper describes the results of the completed two-arm trial comparing the implicit computerised decision aid with evidence-based paper guidelines (see table 1 for details).
Trial interventions
Participants
Participants were recruited from 40 general practices throughout Newcastle and North Tyneside, Gateshead, and South Tyneside Primary Care Trusts and Northumberland Care Trust between November 2001 and June 2004. As we were interested in the use of the methods in day-to-day primary care we recruited both those patients who were already taking warfarin and whose care would be regularly reviewed (prevalent cases) and patients considering taking warfarin for the first time (incident cases). Prevalent cases of non-valvular atrial fibrillation were identified by screening for digoxin and warfarin from computerised prescribing data and by computerised diagnostic registers where available.10 Incident cases were identified opportunistically.
Participants were eligible for inclusion if they were aged 60 years or over and had either chronic non-valvular atrial fibrillation (confirmed by electrocardiogram) or paroxysmal atrial fibrillation. Exclusion criteria were: acute onset of atrial fibrillation requiring cardioversion; previous stroke or transient ischaemic attack; absolute contraindications to warfarin; taking warfarin for another indication; dementia or cognitive impairment sufficient to hinder shared decision-making; non-English speaking; and where the risk of cerebral bleed on warfarin was likely to exceed or approximate to the reduction in risk of thromboembolic stroke.7
Recruitment and randomisation
Eligible participants were sent a letter of invitation co-signed by their own general practitioner (GP), along with an information leaflet on atrial fibrillation, treatment with aspirin and warfarin, and a consent form. Signed consent was obtained before randomisation and was confirmed at the research clinic. Participants were randomised to either: (a) computerised decision aid (intervention) or (b) evidence-based paper guidelines (control), using electronically-generated random permuted blocks via a web-based randomisation service provided by the Centre for Health Services Research. Allocation was stratified by risk of stroke using the SIGN strata.11
Interventions (see table 1 and fig 1 for summary)
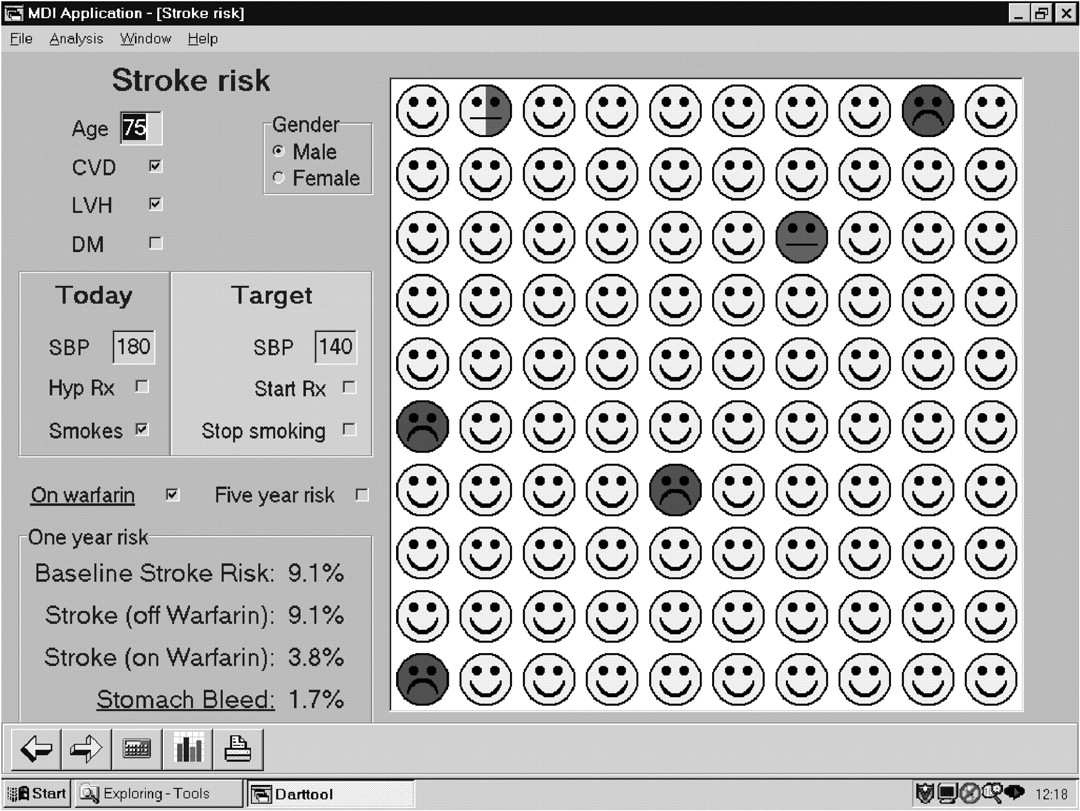
Risk communication screen in the computerised decision aid.
All participants were seen in one of two research clinics each conducted by a single doctor, trained in delivering either the decision aid or guidelines but blinded to the alternative method. In the decision aid group, participants were taken through a presentation of the individualised benefits and potential harms of warfarin treatment and were invited to weigh up the advantages and disadvantages of treatment before coming to a shared decision with the clinic doctor. The individualised benefits/harms component included personalised risk assessment using the Framingham equation for stroke risk, and the benefits of warfarin based on data of effectiveness from trials and the risks of bleeding based on a systematic review of literature. The presentation used both graphical and numerical forms of presentation followed by a shared decision-making component (see Thomson et al (2000)7 and Thomson et al (2002)9 for details). In the evidence-based paper guidelines group, the clinic treatment recommendation was provided by applying decision analysis derived guidelines according to the participants’ risk factor profile7 and the recommendation made directly to the participant by the clinic doctor. All treatment decisions were conveyed to the participants’ own GP for ongoing care.
Outcome measures
The primary outcome measure was the decision conflict scale (DCS) measured immediately after the clinic visit.12 Decisional conflict is a state of uncertainty about a course of action. Such uncertainty is more likely when a person is confronted with decisions involving risk or uncertainty of outcomes, when high-stakes choices with significant potential gains and losses are entertained, when there is a need to make value tradeoffs in selecting a course of action, or when anticipated regret over the positive aspects of rejected options is probable. The scale has been widely applied and there are considerable empirical data to support the effects of decision supporting interventions on decisional conflict and its related modifiable constructs.12,13 The full scale includes 16 questions and has five subscales: informed (a measure of how informed the respondent feels); values (a measure of how clear the respondent feels about their personal values for benefits and risks/side effects); support (a measure of how supported the respondent feels in making their decision); uncertainty (a measure of how certain the respondent feels about their choice); and effective choice (a measure of whether the respondent feels they have made a good or bad decision). This last subscale is usually used after the decision only. The overall score ranges from 1–5, with 5 representing greater decisional conflict.
Secondary outcome measures were the State Trait Anxiety Inventory,14 a knowledge scale15 and Degner’s decision-making preference scale.16
Before clinic attendance (pre-clinic) participants completed a questionnaire that incorporated scales on decision conflict,12 their choice predisposition, knowledge, decision-making preference,16 general anxiety14 and risk factors and demographic information. Immediately following the clinic (post-clinic) participants completed scales on decision conflict, knowledge, decision-making role experienced, and anxiety. Three months after the clinic, participants were sent postal questionnaires including the DCS, decision-making preferences and the knowledge scale.
Other data were collected in the three-month questionnaire and from the participants’ primary care records, including adherence to the initial decision, current treatment, use of primary and secondary care services, cardiovascular risk (Framingham items), health outcomes (including stroke and TIA and adverse bleeding events) and degree of warfarin control.
Sample size
Assuming that groups would be compared using t tests and analysis of variance (ANOVA) it was calculated that 53 participants in each group (total 106) would give 80% power to detect a difference between groups of a mean score of 0.33 units on the DCS (standard deviation 0.6) assuming a significance level of 5%.
Data analysis
Baseline characteristics were compared using Fisher’s exact test for binary variables, χ2 tests for other categorical variables and independent sample t tests for continuous variables. Repeated measures analysis of variance was used to compare changes in the decision conflict score, anxiety and knowledge scores between the two groups. The general strategy was to investigate changes in outcome over time only if the omnibus test of variation between occasions was significant. Differences between groups at particular time points were only investigated if there was an overall significant group effect or a significant group by occasion interaction. The exception to this was primary outcome measure—the total decision conflict score—where the difference in mean score between groups at the end of the clinic was pre-specified as the primary comparison of interest. Differences in the final decision made at the consultation were investigated using logistic regression analysis.
RESULTS
The flow of participants through the trial is shown in figure 2. Pre-clinic there were no significant differences in the characteristics of the participants in the two groups (table 2). There was also no difference between the groups when asked who should make the decision in a clinical consultation. Post-clinic, participants in the decision aid arm were significantly more likely to judge that they were more important in making the decision (35/51 compared to 25/55, χ2 test for trend = 5.67; p = 0.018) consistent with the anticipated impact of the delivery mode.
Baseline characteristics comparing the two arms of the trial

Consort flowchart for the trial. AF, atrial fibrillation; DVT, deep vein thrombosis; MI, myocardial infaction; TIA, transient ischaemic attack.
Outcome measures
For the decision conflict scale (the primary outcome measure), the difference in total scores between groups (maximum score 5 for high decision conflict) was estimated on each occasion. The mean (95% CI) differences for decision aid group versus the guideline group were 0.02 (−0.22 to 0.26), −0.18 (−0.34 to −0.01) and −0.15 (−0.37 to 0.06) at pre-clinic, post-clinic and three month follow-up respectively with a negative difference representing a lower decision conflict. While decision conflict fell in both groups post-clinic compared to pre-clinic, the difference between groups post-clinic was significant at the 5% level (t = 2.12, df = 107, p = 0.036). In terms of the DCS subscales the pattern of responses for the “informed” and “values” subscales followed a very similar pattern with significant (at the 5% level) differences between groups post-clinic, suggesting that the main contributions were in respondents feeling better informed and clearer about their personal values for the risks and benefits of alternative options. There were no differences between groups in the DCS subscales at three months.
There was a significant fall in anxiety immediately after the clinic (mean change pre-clinic to post-clinic of −4.57 (95% CI −6.30 to −2.84)) but no evidence that this reduction varied between the two groups (F1,95 = 0.001; p = 0.98).
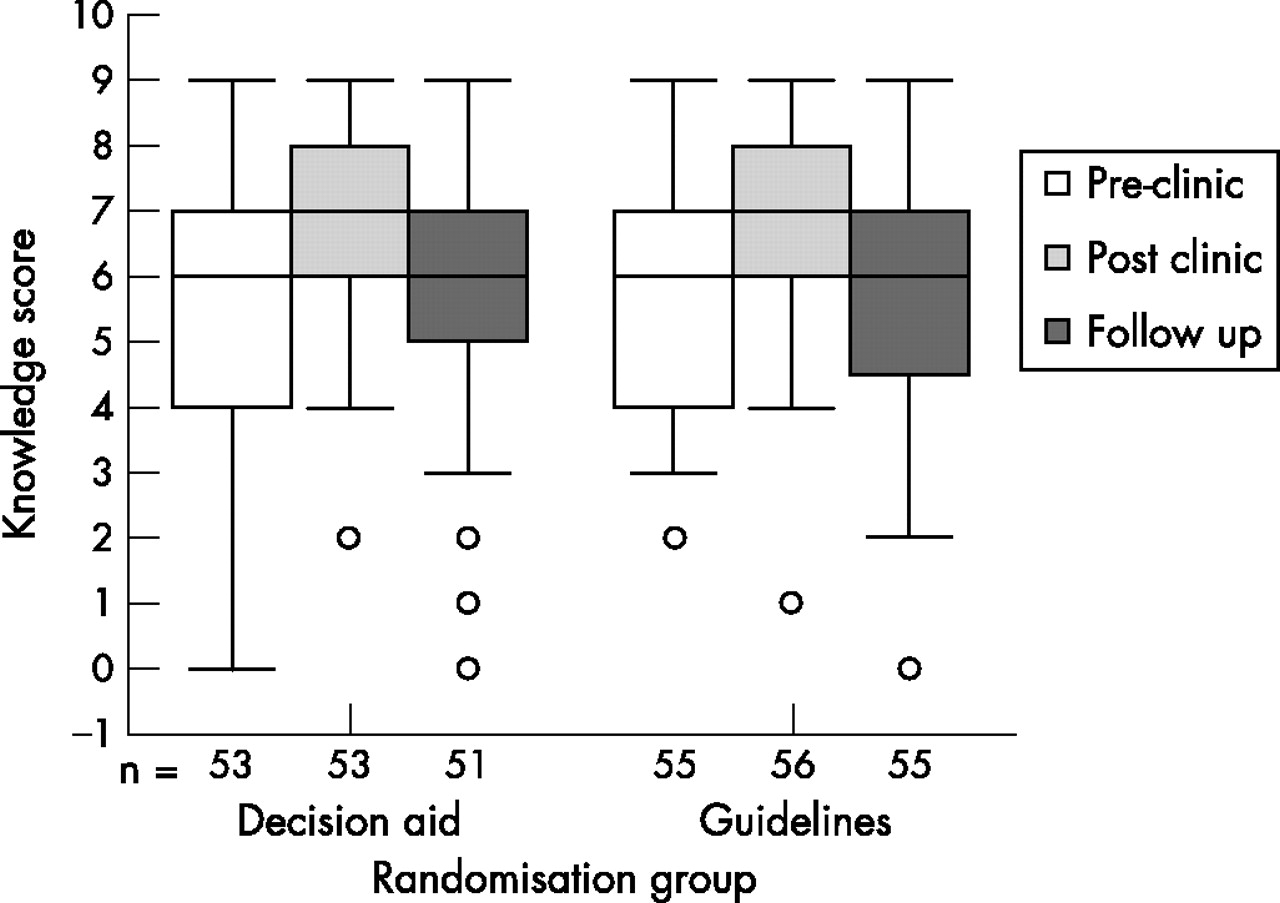
Although the overall knowledge scores improved slightly post-clinic, by three months they were back to pre-clinic levels; there was no difference between decision aid and guidelines groups at any point. Knowledge about warfarin was consistently higher than that about aspirin at each stage (figs 3 and 4). There was no impact of either decision aid or guidelines on knowledge about aspirin. Knowledge about warfarin improved in both decision aid and guidelines groups post-clinic but declined again in both groups by three months. Within the repeated measures analysis of variance framework an additional interaction between pre-clinic treatment and type of knowledge was included and this was significant at the 0.1% level (F1,106 = 33.8; p<0.001) indicating that participants currently taking warfarin had a higher mean warfarin knowledge score than participants on aspirin (difference = 1.79 with 95% CI 1.00 to 2.59).

Knowledge of aspirin in each group before, immediately after and three months after the clinics: box and whisker plots.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Knowledge of warfarin in each group before, immediately after and three months after the clinics: box and whisker plots.
Decision on treatment
Although participants in the decision aid group were less likely to start warfarin than those in the guidelines arm (39/53, 73.6% compared to guidelines 50/56, 81.7%, RR 0.82, 95% CI 0.68 to 0.99) (table 3) this difference is almost completely due to participants not already on warfarin; here the difference was 4/16, 25% compared to guidelines 15/16, 93.8%, RR 0.27, 95% CI 0.11 to 0.63.
Proportion of participants who made a definite decision to start or continue warfarin by group by pre-clinic treatment status
This difference was confirmed by logistic regression. Fitting first a difference between groups, participants in the decision aid group were less likely to make a definite decision to start or continue warfarin than participants in the guidelines arm (OR = 0.33, 95% CI 0.12 to 0.95). Adjusting for pre-clinic treatment the difference between groups remained significant (OR = 0.29 95% CI 0.09 to 0.90). Finally an interaction between group and pre-clinic therapy was included in the model. This interaction was highly significant (change in −2 log likelihood = 16.4; change in degrees of freedom = 1; p<0.001). Participants not already on warfarin who were in the decision aid group were much less likely to start warfarin than participants not already on warfarin in the guidelines arm (OR = 0.01 95% CI 0.001 to 0.16).
Resource use and health outcomes
In the three months after the clinic there was no significant difference in GP consultations between the decision aid group and the guidelines group (n = 39 compared to n = 32, p = 0.35) nor in hospital appointments (n = 29 compared to n = 10, p = 0.06). Only three and four participants respectively were admitted to hospital. There were no strokes and no bleeds requiring admission. There was one transient ischaemic attack and one bleed precipitating GP consultation (both in the guidelines group).
DISCUSSION
This study assessed the impact of a computerised decision aid applied in a shared decision-making consultation on the primary outcome measure of decision conflict as compared to a traditional doctor-led application of paper guidelines. The key finding was a significantly lower decision conflict in the decision aid group than in the paper-based guidelines group immediately after the research clinic and this finding was present across all patients regardless of their initial treatment. Decision conflict was lower after the clinic in both groups.
In addition, there was a marked difference between the two arms in the decision whether or not to take warfarin when patients were not already on this treatment; those in the decision aid group were significantly much less likely to start warfarin than those in the paper guidelines arm.
There has been considerable debate about the most appropriate outcome measures for assessing the effectiveness of decision support tools.17 Many studies of guidelines have assessed their effectiveness in terms of adherence to the guidelines’ recommendations.18 In the case of shared decision-making, such a measure is less appropriate, since the aim is to support patients in making a “good decision” in a setting where the choice between treatments is not clear cut and is likely to be sensitive to patient values—that is, to support patients in making informed choices consistent with their values by presenting the clinical evidence and the likely effects of alternative treatments.
The decision conflict scale was developed to measure perceptions of personal uncertainty in making a choice about healthcare options, the modifiable factors contributing to uncertainty, and the quality of the decision made.12,19 Decisional conflict is a state of uncertainty about a course of action and is, for example, more likely when someone is faced with decisions involving risk or uncertainty of outcomes, and when there is a need to make tradeoffs between choices.
Our results show an effect size on decisional conflict that is comparable to other studies of decision aids,19 suggesting that the computerised decision aid does have a measurable and clinically important impact that is greater than the doctor-led paper-based guidelines. The difference is not maintained at three months, but this is unsurprising—the measure was designed to assess conflict around the time of a difficult decision. After three months, it is likely that the participants have become comfortable with, and more accepting of, the decision made.
The subscale analysis suggests that the main contributions to the observed difference between groups were from differences in feeling better informed and having greater clarity on values. Although we demonstrated differences in two of the subscales, all subscale scores were lower in the decision aid group. We cannot exclude the possibility of differences in the other three as the study was not powered to show differences in subscale measures.
The noted reduction in anxiety in both groups may be related to the opportunity for a prolonged consultation on their condition. Increased knowledge about warfarin may be related to the additional consultation time and the prior presentation of pre-clinic information. The effect was more noticeable for warfarin, likely to reflect the fact that in both groups the starting point for discussion was that warfarin is more effective than aspirin in terms of risk reduction,6 and thus the primary discussion was based on whether participants should take warfarin or, if not, consider aspirin.
A prominent finding of the difference in the proportion of participants electing to take warfarin, which is almost fully explained by those not already on warfarin, is worthy of discussion. This implies that the threshold for choosing to take warfarin is higher in those participants using the decision aid. The most likely explanation is that the decision aid used within a shared decision-making consultation allows for a more balanced presentation of the benefits and the potential harm from warfarin treatment, whereas the paper-based guidelines, presented as direct advice to the patient, allow less discussion and presentation of potential harm and hence place emphasis on overall effectiveness. Thus participants presented with this balance are less likely to take warfarin given their greater understanding of the potential for harm.
The participants in the study included patients who were not on warfarin as well as patients who were already treated. Both were included because we saw the tool as supporting either initial decision-making or treatment review (not least because the clinical status of patients changes over time and merits annual review of such decisions as risk profiles may change). We also argued that it was likely that few, if any, of those currently taking warfarin would have had experienced any form of shared decision making, a feature supported by the focus groups and interviews with patients undertaken during the development phase of the decision aid. Nonetheless the decisions being made are different and this may in part explain the differences between decisions on warfarin initiation or continuation demonstrated.
Other studies of decision aids have suggested that participants are less likely to choose the procedure with a greater risk of adverse effects, for example a trial of a decision aid with participants choosing between watchful waiting and more invasive treatments for prostatic symptoms showed a 40% decrease in surgery rates.20 However, overall the systematic review of randomised controlled trials of decision aids does not reveal a consistent impact on treatment choices.4
Studies of risk perception suggest that people are more averse to risks that are out of their control (as may be felt to be the case with adverse effects of treatments) and to be more averse to proximate risks such as early bleed on warfarin, than more distant risks, such as the later risk of stroke.21 It is also the case that the nature of this decision is based on preventing a future event (stroke) that is probabilistic, a different setting to that of making choices between potentially curative treatments such as in cancer therapy. This suggests that application of shared decision-making, particularly in preventive therapies, might lead to lower rates of uptake of otherwise traditionally defined effective interventions, albeit in participants who are better informed and making decisions consistent with their values. Therefore, although trials may suggest that a patient will, in terms of stroke risk reduction, benefit to a greater extent with warfarin than aspirin, when the patient takes account of their informed personal values they may come to a different decision. This may lead to higher rates of future population health burden in terms of avoidable strokes incurred. There is thus a potential tension between the goals of preventive strategies based upon reduction of population-level disease burden and the choices made by well-informed patients.22
A number of studies have assessed decision-making preferences and treatment thresholds of patients with atrial fibrillation using a range of methods and demonstrate considerable variation in thresholds for warfarin treatment, although few use actual patients making real decisions.23 In studies using decision aids24,25 the majority of patients expressed a preference for aspirin, even if their absolute baseline stroke rate was as high as 4% per year, consistent with the findings of our study. Protheroe and colleagues used a decision analytical approach and found that decisions on treatment based on decision analysis would lead to fewer patients taking warfarin than if the decision were made on the basis of commonly available guidelines.26 Howitt and Armstrong27 found that people already taking warfarin were willing to take it for a lower level of benefit compared with those who were not, again consistent with our differential findings between participants on or not on warfarin at study entry. Furthermore Man-Son-Hing et al24 found that most patients already on aspirin preferred to continue taking aspirin rather than switching to warfarin, suggesting a smaller fraction of these patients would take warfarin at most levels of stroke risk compared with those who were taking or had experienced a course of warfarin therapy. Similarly, in the Howitt and Armstrong study,27 many of the patients expressed reluctance to switch from the anti-thrombotic therapy they were taking to another. Thus it is likely that patients already on an established treatment may prefer to remain with it, and this may in part explain our findings.
Our study has some limitations. The study was designed as an efficacy (explanatory) trial, with the tools being applied in a research clinic setting by appropriately trained doctors. At an early stage, one arm was discontinued (see linked paper8), but this does not affect the validity of the comparison between the remaining arms, the design of which remained unchanged. It was designed as an explanatory trial and participants were invited to a central clinic to see a doctor who was not primarily responsible for their care. This is an artificial situation, although the high levels of adherence to the decisions made at the clinic at three months suggest that the decisions had real meaning for the participants and their GP.
The fact that we recruited participants to the trial who were largely prevalent cases and already on some form of treatment (aspirin or warfarin), lead to a heterogeneous group of participants and the subgroup differences in decisions made reflect this.
Each clinic was delivered by a single doctor, raising the question as to whether the findings reflect the different interventions, the different doctors delivering the interventions or some combination of the two. In some respects this is a false distinction; we were evaluating a package of decision support, and we attempted to minimise any doctor-specific effect by training the doctors in the intervention and the desired mode of delivery. The two doctors delivering the clinics did communicate differently, but that was the intention. The decision aid arm of the trial was presented and delivered within a consultation that incorporated a process of shared decision-making, while the doctor delivering the guidelines advice did so by directly advising the patient on what the guidelines recommended for that patient in a more paternalistic model. Indeed, the results of the survey of participants as to who made the decisions at the clinic suggest that this was effective and hence that the findings are likely to reflect the decision aid and its delivery, rather than the individual characteristics or style of the doctors. There were variations in doctors’ behaviours, but these appeared to be related to specific doctor–patient interactions, rather than the arm of the trial. Video-recording of the interactional dynamics of the consultations and detailed qualitative investigation of patients’ perspectives were an important element of this study and have been described in detail elsewhere.28,29
What is already known
-
Choice of prevention of stroke with warfarin or aspirin is sensitive to patient preferences.
-
Treatment decisions where patient preference is important can be supported by decision aids, but these need evaluation in appropriate studies.
-
A systematic review of decision aids shows that they improve patients’ knowledge, reduce decision conflict and engage patients more actively in decision-making, but have little impact on patient satisfaction, and a variable impact on the actual decisions made.
-
Some studies show reduction in uptake of procedures or treatments.
What this paper adds
-
Participants using a decision aid in a shared decision-making setting have lower decision conflict after its use than those where paper-based guidelines are used in a traditional way.
-
Those who are not already taking warfarin are much less likely to start this treatment when using the computerised decision aid than in the evidence-based paper guidelines arm. This could have significant implications for treatment uptake and stroke prevention.
In summary, our study suggests that a computerised decision aid that presents balanced benefits and harms of therapy in the setting of shared decision-making can lead to reduced decision conflict with an enhanced understanding by patients and decisions consistent with their values. This reflects the findings of use of similar decision aids in other clinical settings. In addition we found a marked difference in the actual decisions made in participants who were not already on warfarin with an apparent reluctance to start warfarin when participants were well informed and able to apply their values to their decisions. This finding may have significant implications for the impact of shared decision-making and the use of decision aids in patients who are making decisions about preventive therapies and is worthy of further exploration.
Acknowledgments
We would like to acknowledge the contributions of the many participants and general practices that made this study possible. We would also like to thank Emma Hutchinson and Margaret Childs for their clerical support, the study doctors (Drs Julian Hargreaves, Jon Tose and David Whitford), and Philip Lowe for programming of the computerised tool. Thanks also to Tim Rapley, Ben Heaven and Eileen Kaner for comments on drafts. The work reported in this paper arises from research funded by a Wellcome Trust Health Services Research Project Grant (Ref nos 065131 and 068380).
REFERENCES
Footnotes
-
Competing interests: None declared.
-
Funding: Wellcome Trust Health Services Research Project Grants. All authors are independent of the funding bodies.
Richard Thomson will act as guarantor for this paper.
The study was approved by the relevant local research ethics committees (Gateshead, South Tyneside, Northumberland and Newcastle/North Tyneside). The trial is registered with an International Standard Randomised Controlled Trial Number of ISRCTN24808514.
Linked Articles
- Quality Lines