Article Text

Abstract
Background: Poor clinical handover creates discontinuities in care leading to patient harm. However, the field of handover research continues to lack standardised definitions and reliable measurement tools to identify factors that would lead to harm reduction and improved safety strategies.
Objective: This paper introduces a conceptual framework to underpin a research agenda around the important patient safety topic of clinical handover.
Methods: Five frameworks with potential application to clinical handover were identified in a consultation process with clinicians, researchers and policy makers.
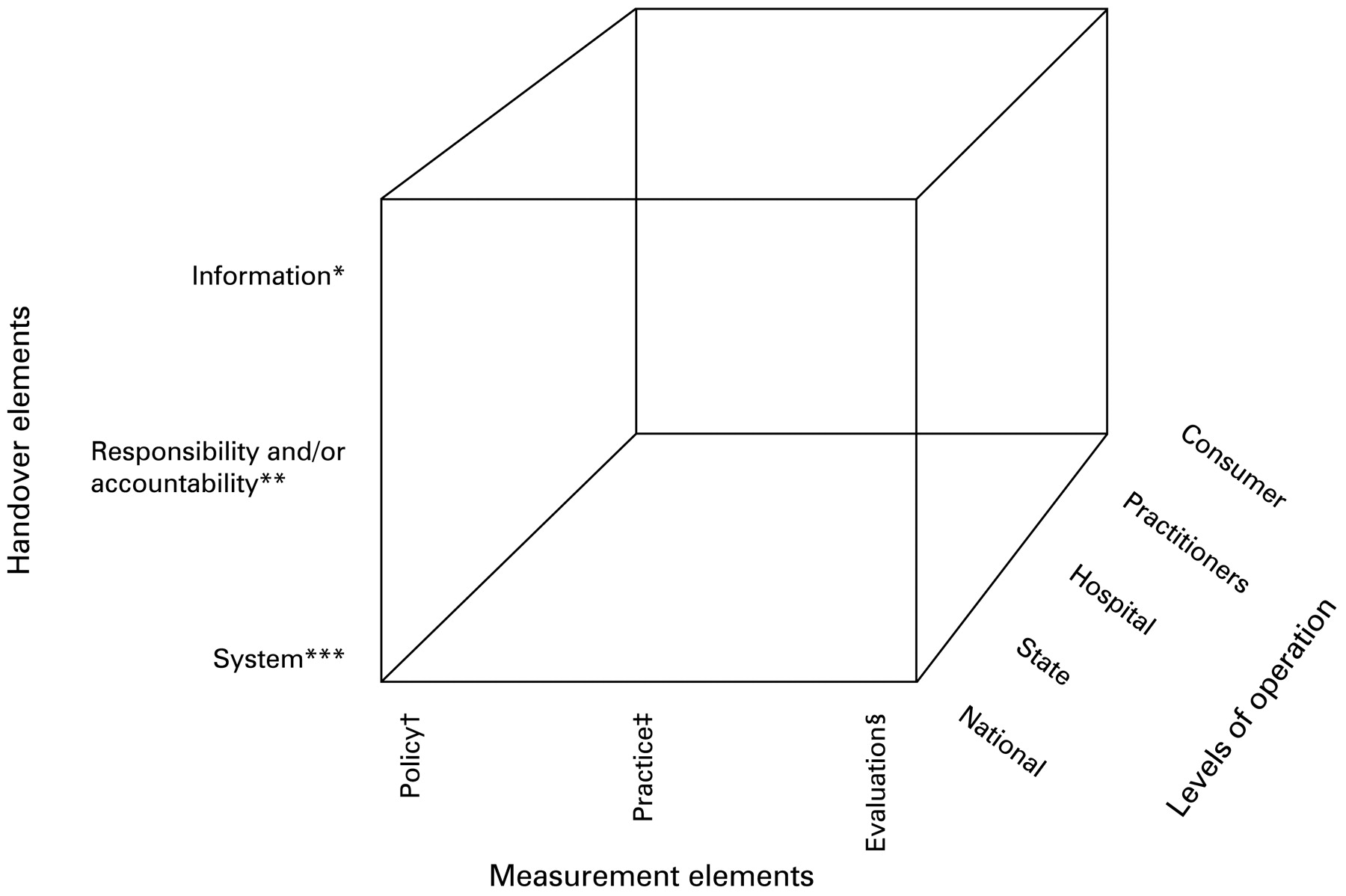
Results: The framework consists of three key handover elements—information, responsibility and/or accountability and system—in relation to three key measurement elements—policy, practice and evaluation. Using this framework an analysis of current “gaps” in the measurement of handover was completed.
Conclusion: The paper argues that measurement will identify gaps in knowledge about handover practice and promote rigor in the design and evaluation of interventions to reduce patient harm.
Statistics from Altmetric.com
Poor clinical handover creates discontinuities in care leading to patient harm. It has been associated with inaccurate clinical assessment and diagnosis, delays in diagnosis, delays in test ordering, medication errors, inconsistent or incorrect results translation, duplication of tests, increased length of stay, increased in-hospital complications and decreased patient satisfaction.1 Coronial cases may assist in elucidating the link to harm.2 In spite of this, the handover research field continues to lack standardised definitions and reliable measurement tools to identify risk factors.
Australia is leading international efforts to improve clinical handover.34 It has been designated as the lead to develop and implement standardised solutions as part of the World Health Organization (WHO) Patient Safety Alliance ‘High Fives’ Initiative. This innovative initiative seeks to leverage cross-national learning among seven countries, using evidence-based protocols within five key patient safety areas. These include the prevention of5:
handover errors;
wrong site/wrong procedure/wrong person surgical errors;
continuity of medication errors;
high concentration drug errors;
promotion of effective hand hygiene practices.
This paper focuses on clinical handover and introduces a conceptual framework to underpin a research agenda within this essential area. Although the development of metrics for handover will take concerted effort, we argue that measurement can help discover and fill gaps in our current knowledge of handover practice and promote rigor in the design and evaluation of interventions that aim to reduce patient harm in handover.
WHAT IS CLINICAL HANDOVER?
There are multiple conceptual models of clinical handover within healthcare. For this paper, we adopt the following definition:
Clinical handover refers to the transfer of information and professional responsibility and accountability between individuals and teams, within the overall system of care.
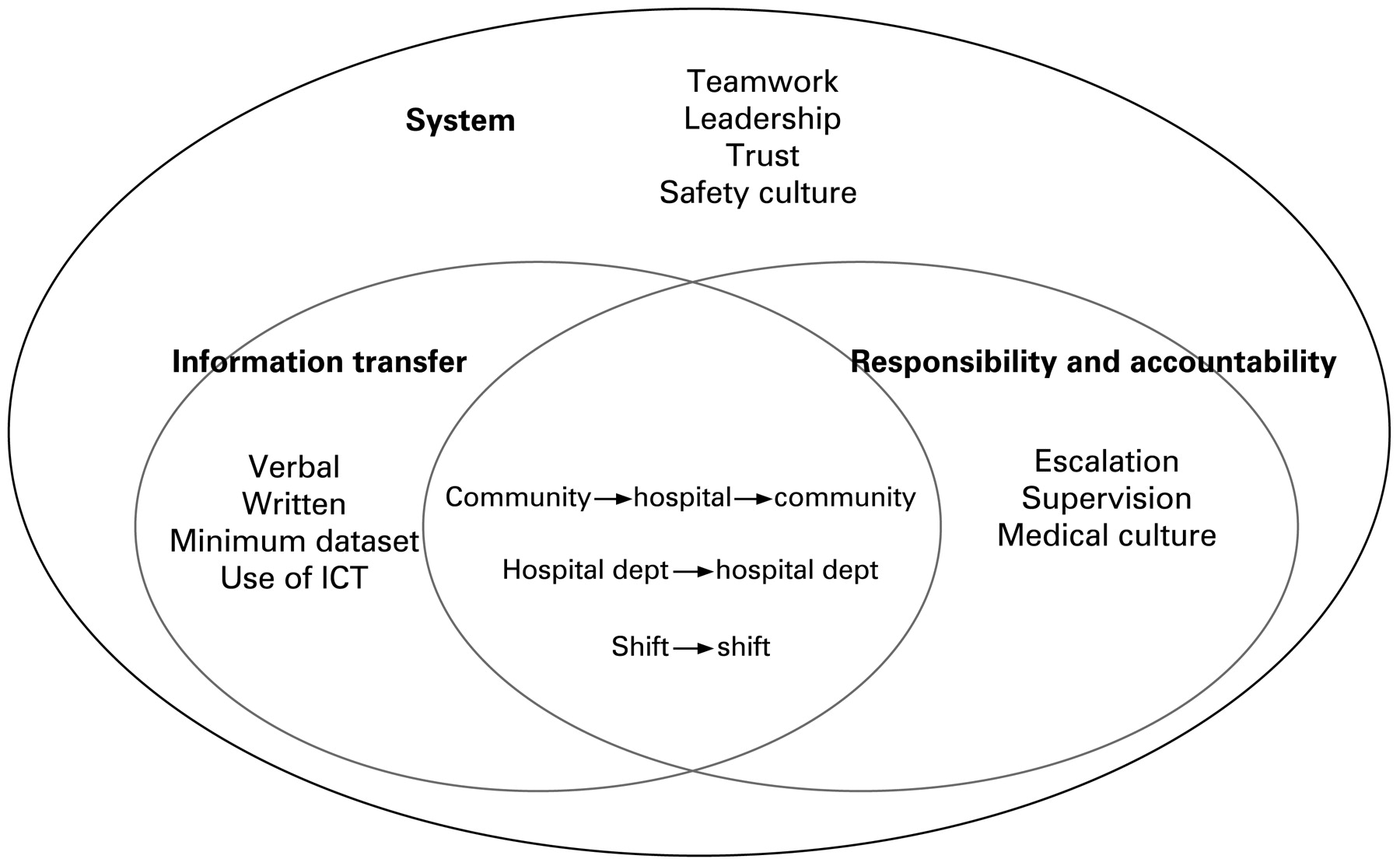
This definition is consistent with recent US definitions6 and the current Australian Medical Association definition which focuses on responsibility but is implicit in its recognition of information transfer.7 Measurement of safety and quality in handover requires consideration of the transfer of three key aspects: (1) information, (2) responsibility and/or accountability, in (3) the context of teams and their work environments8 (fig 1). Although used synonymously, responsibility and accountability are discrete concepts. Responsibility is a personal attribute that can be delegated whereas accountability represents an organisational attribute, often mandated, and which cannot be delegated. Both are important ideas and have growing attention.9

Defining handover—information, responsibility and accountability, and system elements.
Coronial findings provide powerful examples of how discontinuities in care contribute to patient deaths. These can be linked with one or more handover elements. We provide three vignettes to describe cases deemed representative to each element (box 1).2
Box 1: Coronial case studies related to handover—matched to the three key elements*
Key element 1: Information Case number: 739/022
Postoperative anaesthetic instructions were written in the wrong place and subsequently not communicated by either the primary nurse or nurse in charge to the resident medical officer. The patient, who had undergone a subtotal thyroidectomy, was suffering stridor and the anaesthetist should have been contacted immediately. The resident medical officer was inexperienced at performing tracheotomies, which resulted in delays in securing the airway. The patient experienced major cerebral hypoxia and subsequently died.
Comments
This case highlights the complexity of information provision and use within the transition of patient care. Information about care and when to call for assistance was available but not transferred to the appropriate caregiver. This meant that the anaesthetist was not called in a timely manner.
Key element 2: Responsibility and/or accountability Case number: 2350/012
A surgical registrar failed to contact senior medical staff about a patient’s deteriorating status. The patient had been reviewed by a surgeon on day 2 of his hospital stay and diagnosed as having peptic ulcer disease but was not reviewed again. On day 5 he had a fatal cardiac arrest. There were no formal written guidelines identifying the circumstances in which junior medical officers should contact the admitting consultant within the institution in question. The surgical resident gave pain relief but did not call for another vital review by the surgeon before day 5.
Comments
This case highlights the complexity of combining the concept of responsibility with accountability. It could be argued that this case is more about accountability as it is operationalised (ie, lack of a policy to define when to call in a senior doctor). A lack of responsibility would then be demonstrated if the junior doctor did not attend the patient or did not believe that this was within her or his remit.
Key element 3: System Case number: 1294/032
An initial verbal report by the first radiologist reviewing a motor car accident patient was not documented or made available for clinicians. The patient was discharged with no reported head or neck abnormalities. The CT scans were routinely reported the following day when the second radiologist reported a fracture of the second cervical vertebra. The patient’s general practitioner was contacted and the patient returned to hospital, dying days later from complications including haemorrhage around the cord associated with the fracture. The process of radiological reporting and communication with the emergency department was seriously deficient.
Comments
This case encapsulates the complexity of handover (see fig 1) and could have been used as an example of a failure in information or as a failure in accountability (as in the other cases).
*These cases all represent multifactorial failures. They have been simplified and focused on one key element of handover for illustrative purposes. Further details are available, as cited.
HOW CAN MEASUREMENT HELP?
We argue that measurement has the potential to increase opportunities for understanding, controlling and improving the practice of clinical handover. Measurement has been well-established as vital to assessing the quality of care in today’s healthcare system.10 Growing evidence highlights its role in supporting evidence-based decisions and that it can assist in the improvement of care processes, better allocation of resources and promote efficiency.11 Discussion around safety measurement has also begun.12
Clinical handover can benefit from the establishment of consistent and transparent methods of measuring both quality and safety and evaluating changes in practice within handover. A mixture of quantitative and qualitative methods should allow the complexities in handover to be fully explored.13 Action research represents a family of research methodologies which pursue action (or change) and research (or understanding), concurrently.1415 It is, thus, an emergent process which is shaped by understanding borne of the evolving research process. It is particularly well suited to the area of handover where some aspects have a very limited evidence base (eg, in the sphere of responsibility and/or accountability) and where the need for action, in the face of increasing proof that poor practice leads to direct patient harm, is paramount.216
More detail about the field of action research and how this paradigm fits within the context of patient safety is elaborated upon in box 2. We argue that it is a well suited research approach for discovering gaps in the transfer of patient care and in designing sustainable interventions. Action research helps to explain and explore human interaction by employing qualitative interviews and observation.17 It bridges the gap between theory and practice in clinical care by drawing upon professional’s intuition and experience rather than relying on randomised controlled trials.18
Box 2: Explaining action research and how this approach “fits” clinical handover research
Distinguishing features of action research151920
A participative approach
The involvement of diverse teams
Investigation of organisational issues
A cyclic process incorporating action intervention
Benefits of action research within patient safety172122
Action research is increasingly employed in healthcare. This is because it can identify problems in clinical practice and help develop potential solutions. Benefits of action research in patient safety include:
Providing feedback to participants
Tackling practical/concrete problems
Embracing a variety of research methods (qualitative and quantitative)
Promoting organisational commitment
Benefits of action research within clinical handover
The limitations with the action research approach22 are outweighed by benefits within handover. The nature of clinical handover lends itself to action research.23 This is because it involves:
Many different contexts and stakeholders
Is highly dependent on culture and communication
Has limited theory
Has limited evidence of current practice and “gaps”
Currently suffers a lack of evaluation of interventions
FINDING THE KNOWLEDGE “GAPS”?
Many knowledge gaps exist in our understanding of clinical handover. Variations in practice, particularly those impacting on safety and quality, have not been systematically explored. The recency of both an educational and research focus in this arena has meant that interventions to improve practice remain largely unevaluated. Exceptions do exist and are growing in number, especially those which investigate the efficacy of informatics used to augment handover processes.24–27 However, the imperative to build an evidence base around success and failure in handover remains. This is crucial if interventions, at an individual, team and organisational level, are to be designed and tested to promote patient safety, efficiency and quality of care. A new approach is required to achieve this.
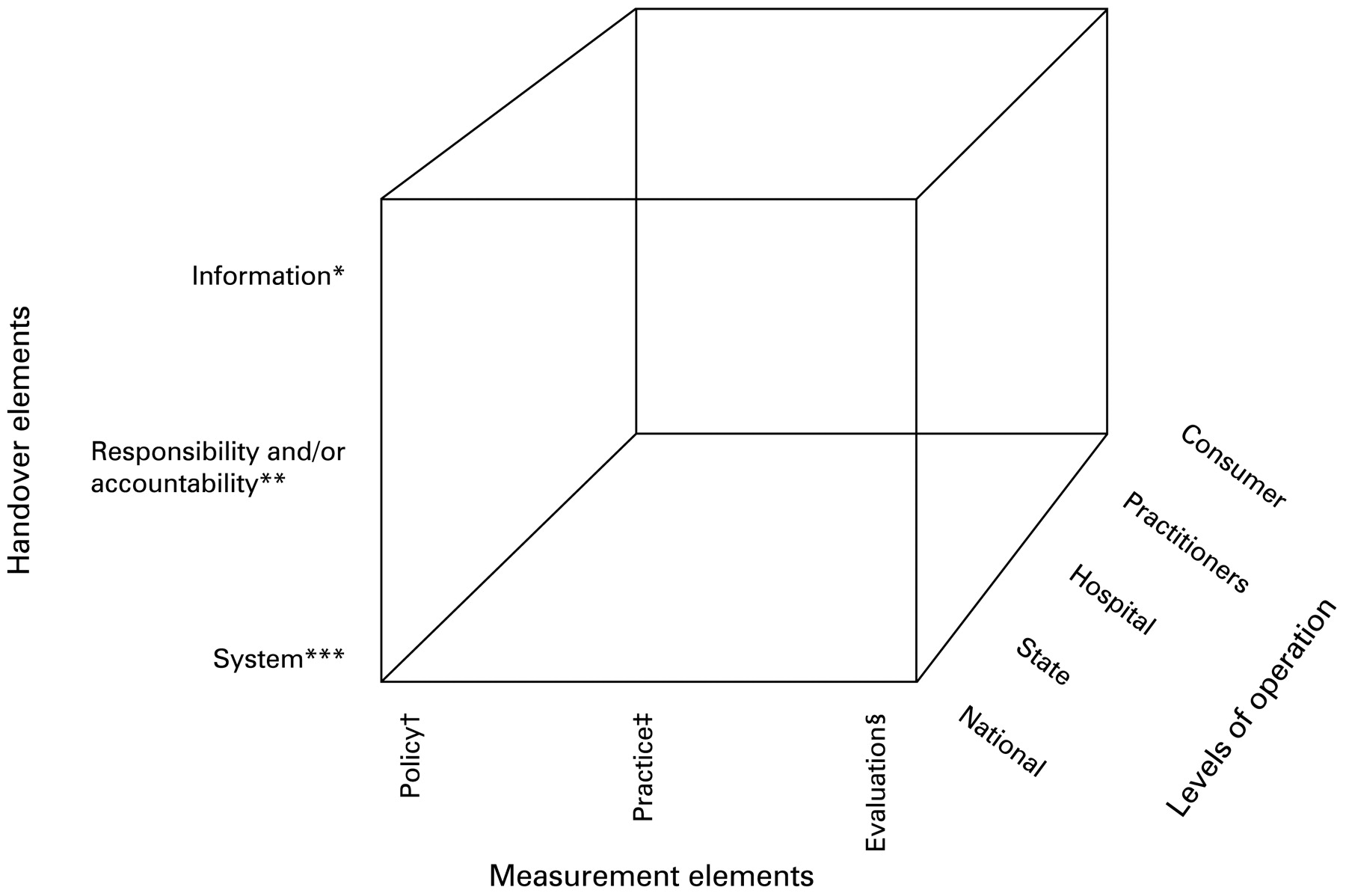
In developing a conceptual framework to underpin future national research a comprehensive literature review was undertaken. Five frameworks with potential application to the area of clinical handover were identified. This was followed by a consultation process with a group of 25 experts, consisting of clinicians, researchers and policy makers. (For the full proceedings, see: http://www.crepatientsafety.org.au/seminars/cre_ps_handoverworkshop.pdf (accessed 26 Mar 2009).) A hybrid framework which combined Donabedian’s model for evaluating quality28 and a normative model, as previously applied to primary healthcare, was proposed and ratified29 (fig 2). This framework allows the consideration of the three key handover elements—information, responsibility and/or accountability and system—in relation to three key measurement elements—namely, policy, practice and evaluation. The framework guides our analysis of current “gaps” in the measurement of handover.
{kind=link}
{kind=link}
Framework for handover—adapted from Donabedian28 and primary healthcare models.29 *Information: communication between health professionals about patient status and care options. **Responsibility and/or accountability: responsibility is not mandated but felt on individual level (ie, you are responsible for your own actions). Accountability is often mandated and cannot be delegated (ie, you are responsible to structures outside yourself). ***System: the larger context of communication and organisation surrounding patient care. †Policy: a written principle, standard or rule to guide decision making and action (eg, standard operating procedures for dispensing meds). ‡Practice: an accepted method or standardised activity (eg, the actual day-to-day practice of dispensing meds by pharmacy staff). §Evaluation: the process of determining whether an item or activity meets specified criteria (eg, based on a priori standards, trend analysis and benchmarking).
INFORMATION
With regard to policy and practice, current knowledge focuses on what information formats exist and how that information is transferred within various models of clinical handover (see fig 1 for the relationship of this with other key handover elements). It is largely anecdotal, collected through small, mainly acute care, trials but points to the power of measurement in demonstrating inefficiencies which may have consequences on patient care. For instance, work on nursing handover demonstrated that 95% of nurses reported no handover process after-hours, leading to duplication of tests and delays in treatment.30 Within the medical model of handover, much of the research around information transfer follows recommendations for the development of standardised care planning and guidelines for clinical handover and surrounds the definition of a minimum dataset. The aim is to design a “simple, informative, time-saving and practical”31 way to assist clinicians, but this may require more applied, qualitative research to understand clinicians’ needs, perceptions and behaviours. Overall, there is a need for epidemiological research to explore and quantify outcomes.
Prior research has focused on producing guides for information handling in handover and how information and communication technologies (ICT) can assist this process.32 However, the evaluation of the effectiveness of ICT and other interventions surrounding information format, transfer and usage has occurred and more is required.3334 There is a need to define appropriate measures to use in such evaluations. Adverse events may be a suitable measure for the evaluation of the safety and efficacy of handover.1 But practical issues could mean that this tool will lack the precision required to make it meaningful.35 This includes the inability to accurately capture adverse events and near misses, due to variations in definitions and reporting. In addition the association between the adverse event and handover can be subject to attribution, recall and hindsight bias. It is clear that other process and outcome measures need to be established for use in the evaluation of clinical handover, potentially using medical simulation.36 Overall, information transfer in handover has been “Unstructured, informal and error prone, with the majority of doctors noting that there was no standard or formal procedure for clinical handover.”37 Rigor around measurement is necessary to progress research in this area.
RESPONSIBILITY AND/OR ACCOUNTABILITY
Contrary to information transfer, the main “gaps” surrounding responsibility and accountability relate to both a lack of knowledge and a lack of measurement (see fig 1 for the relationship of this with other key handover elements). In general, there is a paucity of research around systems of responsibility and accountability in healthcare. This is in spite of the increasing importance that these systems have for policy, practice and evaluation of clinical handover. Within handover there remains no clear policy around mechanisms of either responsibility or accountability, although models of accountability have been adapted for medical systems.38
Box 3: Measurement in handover—example research questions under each key element
Information
Policy
To determine whether standardisation of methods of information transfer will influence practice in clinical handover
Practice
To determine the ideal characteristics of clinical handover for different clinical settings
Evaluation
To determine the most appropriate process and outcome measures for use in the evaluation of clinical handover across clinical settings
Responsibility and/or accountability
Policy
To determine clinicians’ understanding of their responsibility and accountability for clinical handover
Practice
To determine the factors which facilitate or impair the implementation of an appropriate system of responsibility and accountability within and for clinical handover
Evaluation
To evaluate whether systems of accountability and responsibility within clinical handover are consistent and transparent across environmental and professional interfaces of care
System
Policy
To determine the most effective method of interdisciplinary team training to influence practice in clinical handover
Practice
To determine, classify and compare current clinical handover practice at jurisdictional and national levels
Evaluation
To determine whether improvements in clinical handover practice translate into better patient outcomes
Regarding practice, there has been a recent shift which has seen healthcare professionals increasingly encouraged to record all relevant clinical details, not only to aid communication but also as a record of their own judgements.39 This is attributed, largely, to a rise in public litigation, since written records give clearer lines of accountability than other formats. The vignette relating to this handover element illustrates the serious consequences that occur when junior doctors do not have explicit guidelines to follow about the escalation of care and communicating with senior staff. Clearly a handover is required when a patient’s care is escalated—that is, when they are transferred from the ward to intensive care. We argue that a more resilient approach to any handover includes the provision of instructions for when a patient may require an escalation of care. This is a complex subject, beyond the scope of this paper, and requires consideration of issues such as clinical judgement and supervision.
Although there may be exemplars of good practice in some large academic departments, most organisations continue to rely on traditions of practice and other sociocultural influences. Overall, the majority of healthcare organisations do not yet possess explicit structures as to whose responsibility it is, within care teams, to bring patient information to handover. Clearly, there is a need for developmental work in this arena, especially since clinical handover encompasses a multitude of interfaces at the individual, team and organisational levels.
A broad assertion about the lack of definition and measurement surrounding responsibility and accountability in handover is that it leads to compromises in patient safety.1 For instance, there is evidence that blurred systems of responsibility and/or accountabilities contribute to inadequate escalation of care.40 Research to survey current practice, within different models of handover with the aim of developing effective systems of accountability and responsibility, alongside policies to enforce them, is vital. However, even with policies in place professional practice has been shown to be guided by cultural and historical factors which need to be considered when developing clinical measures. Subsequent evaluation is crucial, to ensure consistency and transparency. In addition, staff’s responses to such measures should be sought, similar to other domains.41
SYSTEM
The concept of a “clinical microsystem” is useful in order to understand how the process of handover fits within the larger systems of communication and organisation relating to patient care42 (see fig 1 for the relationship of this with other key handover elements). Considerable literature exists on how to improve reliability and safety within safety-critical systems and these lessons are being applied to healthcare.43 Thus, policy at the system level exists that can be implemented in order to promote the effective transfer of information and responsibility and/or accountability across clinical handover. For example, policies designed to improve safety practices, emphasising issues such as teamwork, leadership and trust, contribute to improved communication and learning.
Teamwork is particularly pertinent in the multidisciplinary and complex interactions that relate to clinical handover. Unfortunately, there is currently no validated method of assessing teamwork but medical simulation training and research may provide opportunities to establish and evaluate existing objective measurement tools in order to help optimise team functioning in handovers.36 Other relevant questions from a system perspective are how best to determine an appropriate system for the escalation of care within handover, how to standardise necessary staff competencies, how to analyse the impact of cultural factors (at an individual, team and organisational level) on the practice and effectiveness of clinical handover and, also, how to classify and compare current handover processes at jurisdictional and national levels. Embedding effective handover into practice will not occur unless there is a fundamental understanding of larger context issues such as culture and teamwork, and an appreciation that handover forms part of a complex adaptive system.44
Finally, important questions, relating to the measurement of change and which are currently largely neglected, are:
How does change in handover practice impact upon quality of care?
Do improvements in clinical handover practice translate into better patient outcomes?
Translational research, adopting the principles of robust measurement, may provide some answers to systems-level issues. Examples of research questions for each of the three key handover elements (information transfer, responsibility/accountability and system), alongside the three key measurement elements (policy, practice and evaluation) demonstrate how our proposed framework for handover is useful in developing and prioritising future research in this area (box 3).
CONCLUSION
Lack of a systematic approach to clinical handover remains a major barrier to improving practice, reducing patient harm and ensuring safe care.137 Although the burdens of measurement are often emphasised, it can provide safety, quality and efficiency benefits.10 For clinical handover, an area that has previously been driven by an urgency for change and action, it appears that applying proven principles of measurement can offer a much-needed evidence base for interventions. Potential for patient safety benefits may follow.
The use of a conceptual framework to underpin this research process is necessary to identify the key knowledge gaps and how best to address these gaps with the use of policy, practice and evaluation guidance. Action research is also suggested as the best approach to identifying and alleviating such gaps in knowledge. Examination of current research shows that information transfer in handover has been anecdotally explored but needs more rigorous research to collect process and outcome data. Responsibility and accountability is an area that needs definitional and developmental work, reflecting a neglect of previous investigation in this influential area. System issues require translational research to explain clinical setting variations. This paper is the first to suggest a national research agenda. It has identified key concepts and how to investigate them. The next step is to establish priorities and resource needs. Improving measurement in handover must be a patient safety priority within all international efforts.
Acknowledgments
We would like to thank both the Australian Commission for Safety and Quality in Healthcare and a team of patient safety experts for their input into a national workshop on clinical handover during which the conceptual framework in this paper was first introduced and ratified.
REFERENCES
Footnotes
Funding: The NHMRC designated Centre for Research Excellence in Patient Safety (CRE-PS) was established in late 2005 with the objective of developing national research capability and capacity that in turn improve patient safety. The Australian Commission for Safety and Quality in Health Care is currently responsible for funding arrangements over a 5-year period with CRE-PS.
Competing interests: None.
Linked Articles
- Quality lines