Article Text

Abstract
Introduction Prolonged emergency department boarding times (EDBT) are associated with adverse clinical outcomes and longer hospital stays. A rapid admission protocol was designed at our institution to reduce both EDBT and time to admission orders (EDTAO) for patients admitted to the internal medicine service.
Methods The existing admission process was examined by a team of clinical and administrative leaders who focused on developing a change management architecture, narrowing clinical roles, mandating direct communication, establishing clear boundaries for patient responsibility and instituting carefully constructed holding orders. The number of steps in the admission process was reduced from 50 to 10. We collected EDBT and EDTAO for all patients admitted to the internal medicine service before and after intervention using a simple interrupted time-series design.
Results The study involved a total of 9604 admissions to one of three inpatient destinations (general medicine ward, telemetry or intensive care unit). The overall EDBT decreased from 360 min in the preintervention period to 270 min in phase 4 (p<0.001). The overall time to admission orders decreased from 210 min in the preintervention period to 75 min in phase 4 (p<0.001) overall. However, no improvements were noted in EDBT for telemetry or ICU patients.
Conclusions Institution of a rapid admission protocol successfully reduced overall EDBT at our institution, although few gains were noted for patients with a telemetry or ICU destination. In total, the intervention saved 27 884 h, or 1161 emergency department patient-days, over the course of a single year.
- Crowding
- emergency service, hospital/organisation & administration
- health services research
- operations research
- outcome and process assessment (healthcare)
- healthcare quality improvement
- quality of care
- emergency department
- healthcare quality
Statistics from Altmetric.com
- Crowding
- emergency service, hospital/organisation & administration
- health services research
- operations research
- outcome and process assessment (healthcare)
- healthcare quality improvement
- quality of care
- emergency department
- healthcare quality
Prolonged emergency department boarding times (EDBT), defined as “the mean time from inpatient bed request to physical departure” from the emergency department (ED) is the source of increasingly intense and appropriate scrutiny.1 Studies have shown that prolonged EDBT is associated with delays in antibiotic administration, increased mortality and increased lengths of stay.2–5 Longer EDBT also results in ED overcrowding, diversion of valuable staff resources from other patients, decreases in ED treatment capacity and loss of revenue.6–11 Recently, the Joint Commission on Accreditation of Healthcare Organizations included EDBT as a potential focus for hospital review.12
A number of factors may contribute to prolonged EDBT for admitted patients, including insufficient inpatient beds, inadequate staffing or inefficient discharge and room turnover practices. Inefficiencies within the ED may also prevent the timely transition of patients from ED to inpatient units. Despite the importance of creating a rapid admission process, hospitals, particularly large academic centres, struggle with achieving this goal.9 Some have suggested that for clinical redesign efforts to succeed, change management concepts must be applied with particular attention to multidisciplinary physician leadership and institutional support.6 9 10
At our institution, three sets of outside consultants were hired to improve the ED admission process over the last decade, with little success. However, the consultancies were illuminating, demonstrating that the process was complicated and riddled with ambiguities, redundancies and competing interests emerging from multiple centres of influence. In response, a team of clinical and administrative leaders from the Departments of Internal Medicine and Emergency Medicine developed a rapid admission protocol (RAP) to facilitate the transfer of patients admitted to the internal medicine service. In this article, we describe the development of the RAP, including the guiding principles used to design the process. We also measure the protocol's effectiveness in achieving two goals: reducing time to admission orders and total boarding time.
Methods
Study design and setting
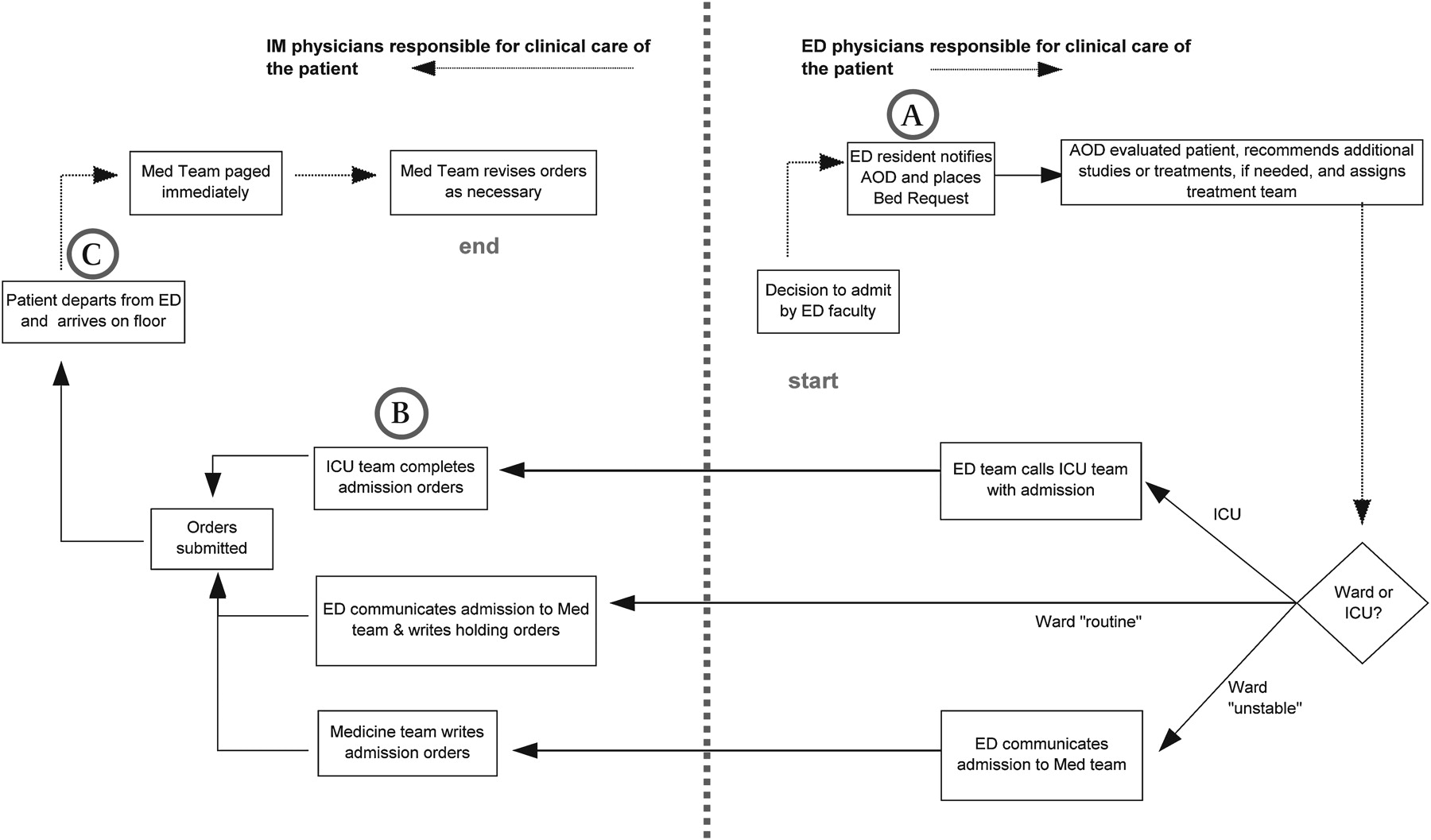
This study was conducted at Parkland Health & Hospital System, a 900-bed academic public hospital in Dallas, Texas, which houses the 24th busiest ED in the USA.11 We conducted a simple interrupted time-series study in which the primary outcome measures were (1) ED time to admission orders (EDTAO), defined as the time from inpatient bed request to receipt of admission or transitional orders, and (2) EDBT, defined as the time from bed request to departure from the ED (figure 1). We included all patients admitted to the internal medicine service from the ED between 23 May 2007 and 30 June 2008. The study period was divided into five phases (baseline: 23 May 2007 to 30 June 2007; postintervention phase 1: 1 July 2007 to 30 September 2007; phase 2: 1 October 2007 to 31 December 2008; phase 3: 1 January 2008 to 31 March 2008; and phase 4: 1 April to 30 June 2008). The admission process was redesigned over a 9-month period. The redesign process included three steps: (1) detailed assessment of the current state process; (2) development of a future state process, termed RAP; and (3) creation of a change management architecture. The University of Texas Southwestern Medical Center Institutional Review Board approved the research protocol.
{kind=link}
Rapid Admission Protocol (RAP) Workflow.
Assessment of the current state
A small team of clinical and administrative leaders from the Departments of Internal Medicine and Emergency Medicine was convened to lead this effort. Members of the team walked through the entire admission process from entry in the ED to arrival in the inpatient unit. The clinical workflow was examined using a variety of parameters, including level of acuity and inpatient destination. Each step in the admission process was documented on a process map, which was subsequently revised through a series of focus groups with key informants. During this examination, the process map was layered with cultural and organisational factors that could not be captured in a linear diagram; many of these factors reinforced inefficiencies in the admission process. The final process map revealed 50 to 75 steps between bed request and time to admission orders. Most of the participants agreed that the process was excessively complex, redundant and, in some capacities, unsafe. Nearly 25 problems with the admission process were identified; these were rank ordered by the team to select areas requiring immediate focus for investigation. The top 10 problems are reproduced in table 1.
Key problems identified by small-group participants
Development of a RAP
After considering problems inherent in the existing admission process, the project team developed a set of eight guiding principles to inform the construction and implementation of a new RAP (table 2).
Guiding principles used in developing the rapid admission protocol
Perhaps similarly to other academic hospitals, the team discovered that the admission process had grown knotty and tangled over the years. It was felt that the process required a sudden and transformational change, implemented at a fixed point in time. Once the decision was made to discard the old process, the team sketched various admission strategies over 2 months using the guiding principles. Once the first draft of RAP was agreed upon, the team sought feedback from staff in multiple clinical departments (internal medicine, emergency medicine, radiology, surgery and pathology), resulting in many minor and at least four major revisions of the process. In the 2 months before going live, negotiations became more intense between departments as we sought approval at the chairperson level; the RAP underwent 52 further revisions during this period. The final admission process was reduced from 50 steps to 10.
The team set 1 July 2007 as the implementation date since a new class of house staff would begin that day. Setting a deadline for implementation also lent a sense of urgency to the process, a component of successful change efforts noted in other industries.13 Three weeks before the implementation, physician and nurse staff received extensive in-service education about RAP through town-hall meetings and small-group sessions.
Among many changes, the new RAP specifically differed from the original process in four important ways. First, physician roles were narrowed and simplified. Previously, a single internal medicine house-staff officer, named the admitting officer on duty, was responsible for evaluating admitted patients to determine if additional studies or consults were needed, assigning the admitting service, communicating details of the admission to the receiving team and temporarily managing care of the patient. This convergence of responsibilities produced bottlenecks and resulted in unnecessary care transitions. In the new process, the role of the admitting officer on duty was narrowed to a handful of clinical activities (figure 1). Second, we instituted transitional orders that could be initiated by ED physicians to help expedite the transfer of clinically stable patients to the admitting unit of the hospital. These transitional orders are completed only after a structured hand-off communication occurs with the admitting team; this communication often results in considerations or recommendations from the receiving service. Transitional orders are valid for a maximum of 4 h and immediately superseded by admission orders from the primary team. To make the transition as safe as possible, we did not allow transitional orders for patients admitted to the ICU or for ward patients who were deemed clinically unstable by the admitting officer on duty or emergency physicians.
Third, the internal medicine team assumed full responsibility for the patient after either the admission or transitional orders were received. In our focus groups, ED nurses expressed frustration that it was sometimes unclear which set of physicians needed to be contacted for patient issues during the hand-off between services. With the new protocol, a “bright line” was created that clearly articulated responsibility for the patient at any stage in the admission process (figure 1). Fourth, before RAP, the desire to fully “package” a patient by completing all diagnostic tests before departure from the ED impeded flow. In the new protocol, routine patients are transferred to the admitting hospital unit as soon as a bed is available, even if the primary admitting team has not yet evaluated the patient. If the patient arrives to the unit, and full admission orders are not available, the primary team is paged and expected to evaluate the patient quickly.
Change management architecture
Heeding John Kotter's principle of developing a “guiding coalition” for any change effort, we developed a committee of clinical and administrative leaders in the internal medicine and emergency medicine departments to oversee implementation.13 This group was very familiar with RAP and met weekly for 2 months after implementation to discuss the performance of the initiative, review patient care problems, assess statistical process control charts and approve amendments to the protocol as needed. Members of this committee served as highly visible champions for RAP.
Statistical analysis
We calculated the EDTAO and EDBT for all patients in the study period using timestamps in the clinical information systems at Parkland Hospital. To assess differences with the baseline period, we calculated a median value for both outcome variables by phase and inpatient destination. Both EDTAO and EDBT were non-normally distributed; thus, we used the two-sample Wilcoxon rank-sum test to compare each of the postintervention phases with the baseline phase. All statistical tests were performed using STATA V.10 (Stata, College Station, Texas, USA). Statistical significance was set at p<0.05.
Results
Patient characteristics
The study involved 9604 admissions. We found minimal differences in the characteristics of the patients with respect to age, race, gender, proportion of Medicaid or self-pay, median number of comorbidities per patient, or relative proportion of principal diagnoses for heart failure, acute kidney injury or pneumonia between any of the study periods (table 3).
Characteristics of preintervention and postintervention patient groups
ED boarding time
The overall median EDBT decreased from 360 min in the preintervention period to 270 min in phase 4 of the intervention (p<0.001), representing a 25% reduction. The reduction in median EDBT was even greater for patients admitted to the internal medicine ward (345 min during the baseline period to 225 min during phase 4 of the intervention, p<0.001). Median boarding times showed little change for telemetry patients (375 and 360 min in the baseline phase and phase 4 intervention periods, respectively; p<0.001) and increased for ICU patients (360 min during the baseline period and 405 min during phase 4 of the intervention, p<0.001).
ED time to admission order
The median overall time to admission orders decreased from 210 min in the preintervention period to 75 min in phase 4 (p<0.001), representing a 64% reduction. Statistically significant reductions were also noted for all three admission destination types (ward, telemetry and ICU experienced a reduction of 71%, 64% and 38% in EDTAO, respectively; p<0.001 in all cases). These findings are summarised in table 4.
Median boarding and transfer times: baseline through postintervention phase 4
Discussion
Prolonged EDBT are associated with adverse clinical outcomes and longer hospital stays.2–5 Excessive numbers of boarded patients also contribute to ED overcrowding, which is associated with delays in diagnosis, treatment and increased mortality.14–16 We redesigned the ED admission process at our institution to improve the EDBT for patients admitted to the internal medicine service. After implementation of our RAP, EDBT was statistically significantly decreased, dropping by 25%. Adding each individual patient's times together, the intervention saved approximately 27 884 h of ED staff time, or 1161 ED patient-days, over a single year. The new RAP also resulted in a statistically significant reduction in the time to transfer of responsibility, reflected by a 64% drop in the EDTAO. Both improvements were durable and clinically meaningful. We found minimal differences in the characteristics of the patients throughout the study, suggesting that baseline and intervention periods were suitable for comparison.
Transition to the RAP represented a significant cultural and procedural shift for our institution. We created consensus for the new protocol by hewing to five change management strategies. First, we formed a credible multidisciplinary team with the authority to make and defend changes in the status quo.13 Medical centres often have clinical leaders with substantial informal authority, whose reputation among staff may not be explicitly recognised in their title but whose regard for an improvement initiative will determine its viability. Hospital administrators and clinical leaders must be especially aligned in academic environments; otherwise, teaching needs may clash with hospital imperatives, resulting in gridlock.9 We selected our team with these considerations strongly in mind. Second, the particular tactics behind the protocol were not decided until this group first agreed upon a set of shared principles.13 17 During periods of intense negotiation, changes to the protocol were repeatedly evaluated against this compass, which formed, in a sense, a clinical and administrative “true north”. Third, we initiated a wide-ranging dialogue among the staff about the admission process, assembling perspectives from a diverse set of stakeholders. Multiple studies have demonstrated the importance of involving stakeholders when addressing ED overcrowding.6 9 18 Although we tackled a qualitatively different problem, our effort required a similar approach. Fourth, the RAP was negotiated under a fixed deadline, which lent urgency and clarity to otherwise time-consuming deliberations among multiple departments. Finally, we implemented the new protocol with “all hands on deck”, including a weekly meeting to review and act upon problems immediately. The primary outcomes of the intervention, EDBT and EDTAO, were carefully examined using statistical process controls that were transparent and accessible.
The benefits associated with reduction in EDBT have been well studied. However, in hospitals for which inpatient bed capacity is temporarily or persistently unavailable, a RAP may not reduce EDBT.10 In these situations, time to transfer to the appropriate inpatient team may be the next most important goal. Several studies suggest that providers who routinely deliver inpatient care should be responsible for admitted patients, even if these patients are physically located in an ED.19 20 We decided to tackle this problem in two ways; first, we established that transitional orders signified a full transfer of patient responsibility to the internal medicine team; second, we aggressively pursued reducing the time to transfer. At our hospital, telemetry and ICU beds are a scarce resource. For example, compared with other hospitals in Texas, Parkland's ICU to general bed ratio is in the 18th percentile. As a consequence, we did not realise reductions in EDBT for patients assigned to these destinations. However, both sets of patients experienced statistically significant reductions in the time to transfer of responsibility, as represented by the EDTAO. We are currently re-engineering the telemetry process at our hospital to reduce inappropriate utilisation on the inpatient ward. The ICU bottleneck represents a more challenging problem; in the next phase of improvement, we are working to better stratify high- and low-risk patients by using data from the electronic medical record, establish interfacility agreements for long-term ventilated patients, and use the results of this study to design a more flexible capacity in a new hospital that will replace the current facility in 2014. In future phases of this work, we will also prospectively follow clinical outcomes associated with throughput interventions; although we reviewed problematic cases throughout the intervention, the lack of systematic clinical data collection represented a weakness of this study.
The introduction of the RAP represents an important milestone for hospital flow and patient safety at our institution. The new protocol appears reliable, producing a reduction in boarding times that have persisted 1 year after the intervention. Our approach focused on developing change management architecture, narrowing clinical roles, mandating direct communication, establishing clear boundaries for patient responsibility and instituting carefully constructed holding orders. Hospitals with similar telemetry and ICU bed constraints may also wish to focus on both EDBT and EDTAO as we did. Our experience suggests that an internal team of appropriately equipped leaders is more likely to be successful than outside agencies or consultants.
Acknowledgments
We wish to thank Kelly Heathman, Josh Floren, Randy Blanchard, Jennifer Sharpe, Carol Croft, Michael Wainscott, Paul Pepe and the emergency medicine and internal medicine chief residents. We also wish to thank the senior administration of the Parkland Health & Hospital System and other faculty whose support was essential to this project: Ron Anderson, Jay Shannon, Joseph Minei and Greg Fitz.
References
Footnotes
Competing interests None.
Ethics approval This study was conducted with the approval of the University of Texas Southwestern Medical Center and Parkland Health & Hospital System Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Editorial
- Quality lines