Article Text

Abstract
Objectives To describe how in-depth analysis of adverse events can reveal underlying causes.
Methods Triggers for adverse events were developed using the hospital's computerised medical record (naloxone for opiate-related oversedation and administration of a glucose bolus while on insulin for insulin-related hypoglycaemia). Triggers were identified daily. Based on information from the medical record and interviews, a subject expert determined if an adverse drug event had occurred and then conducted a real-time analysis to identify event characteristics. Expert groups, consisting of frontline staff and specialist physicians, examined event characteristics and determined the apparent cause.
Results 30 insulin-related hypoglycaemia events and 34 opiate-related oversedation events were identified by the triggers over 16 and 21 months, respectively. In the opinion of the experts, patients receiving continuous-infusion insulin and those receiving dextrose only via parenteral nutrition were at increased risk for insulin-related hypoglycaemia. Lack of standardisation in insulin-dosing decisions and variation regarding when and how much to adjust insulin doses in response to changing glucose levels were identified as common causes of the adverse events. Opiate-related oversedation events often occurred within 48 h of surgery. Variation in pain management in the operating room and post-anaesthesia care unit was identified by the experts as potential causes. Variations in practice, multiple services writing orders, multidrug regimens and variations in interpretation of patient assessments were also noted as potential contributing causes.
Conclusions Identification of adverse drug events through an automated trigger system, supplemented by in-depth analysis, can help identify targets for intervention and improvement.
- Adverse drug event
- automated trigger
- safety
- quality improvement
- patient safety
- healthcare quality improvement
- quality of care
- medication error
- adverse event
Statistics from Altmetric.com
- Adverse drug event
- automated trigger
- safety
- quality improvement
- patient safety
- healthcare quality improvement
- quality of care
- medication error
- adverse event
Harm from medical errors is a significant public health problem.1 2 A recent systematic review concluded that adverse events during hospital admission affect nearly 1 out of 10 patients.1 Harm from medical errors is financially costly,3 4 and can result in loss of trust in physicians and the healthcare system by patients and their families.2 Medication-associated events, known as adverse drug events (ADEs), constitute approximately 19% of all adverse events and are the most common source of patient injury, likely because drugs are the most common medical intervention.5 6
Children are at a particularly high risk for harm when a medication error occurs.7 They experience rapid and continuous developmental changes that affect the safety, metabolism and dosage of medications.8 Doses must be adjusted for a child's weight, change in body composition and stage of development.7 9 10 Many medications supplied to the pharmacy in standard adult dosage forms must be subdivided or diluted before administration to children. Infants and young children have limited physiologic reserves to buffer mistakes.11 Likely related to these factors, potential ADEs have been reported to be three times more likely to occur in children's hospitals than in adult hospitals.11
Most healthcare organisations attempt to detect and measure ADEs using voluntary incident reporting systems. However, often less than 5% of events are captured this way.12–16 Traditional retrospective medical record review identifies more events; however, it is expensive, labour intensive and often occurs long after the event.12 Trigger methodology was designed to detect adverse events more efficiently. It uses a structured search for “flags”, such as medications or laboratory values, to identify possible adverse events.15 17–21 Using a paediatric-specific trigger tool for focused manual chart review in 12 paediatric hospitals, Takata et al16 reported a mean ADE rate of 15.7 per 1000 patient-days. Automating the use of trigger tools with an electronic medical record has been shown to be even more efficient and allows for near real-time monitoring of all patients.12 14 22–25 Using a computerised surveillance system, Ferranti et al26 reported a rate of 1.6 ADEs per 1000 patient-days for paediatric patients. An ADE rate of 22.3 per 1000 patient-days was reported for three children's hospitals based on triggers identified in the electronic data repositories.27
Detection of ADEs is not enough to prevent them. Successful use of improvement methods to reduce ADEs requires understanding of their causes and patterns. Rapid identification and analysis may reveal patterns likely to cause future ADEs.15 This information can help prioritise and direct efforts to redesign systems to prevent future occurrences.28 29
We report on the in-depth analysis of the characteristics and causes of two common paediatric ADEs identified by an automated trigger system. We hypothesised that in-depth analysis of each event would provide information useful for identification of causal trends. In addition, we believed that the automated trigger system would identify significantly more ADEs than the hospital's voluntary safety reporting system.
Methods
Setting and organisational context
Cincinnati Children's Hospital Medical Center (CCHMC) is a large, urban paediatric academic medical centre with 475 registered beds and more than 27 000 admissions in fiscal year 2007. In 2002, the CCHMC developed a system to integrate clinical information that included computerised clinical order entry, clinical documentation, electronic medication administration record, data storage repository and advanced clinical decision support.
Voluntary safety reporting system
Until 2006, CCHMC used two main strategies to detect harm to patients. The first was an online voluntary safety reporting system. Employees were expected to submit reports for all incidents of potential and real harm. The reports were meant to be non-punitive and could be made anonymously. All reports were reviewed by members of the risk management department and sent to the appropriate unit manager.
Random medical record review
The second strategy, a random medical record review, was initiated in 2002. Each month, reviewers examined a random sample of 20 inpatient medical records for the presence of 15 specified trigger events.16 The reviewers also took note of any other recorded adverse events. However, they did not gather information on causes of ADEs.
Automated ADE detection programme
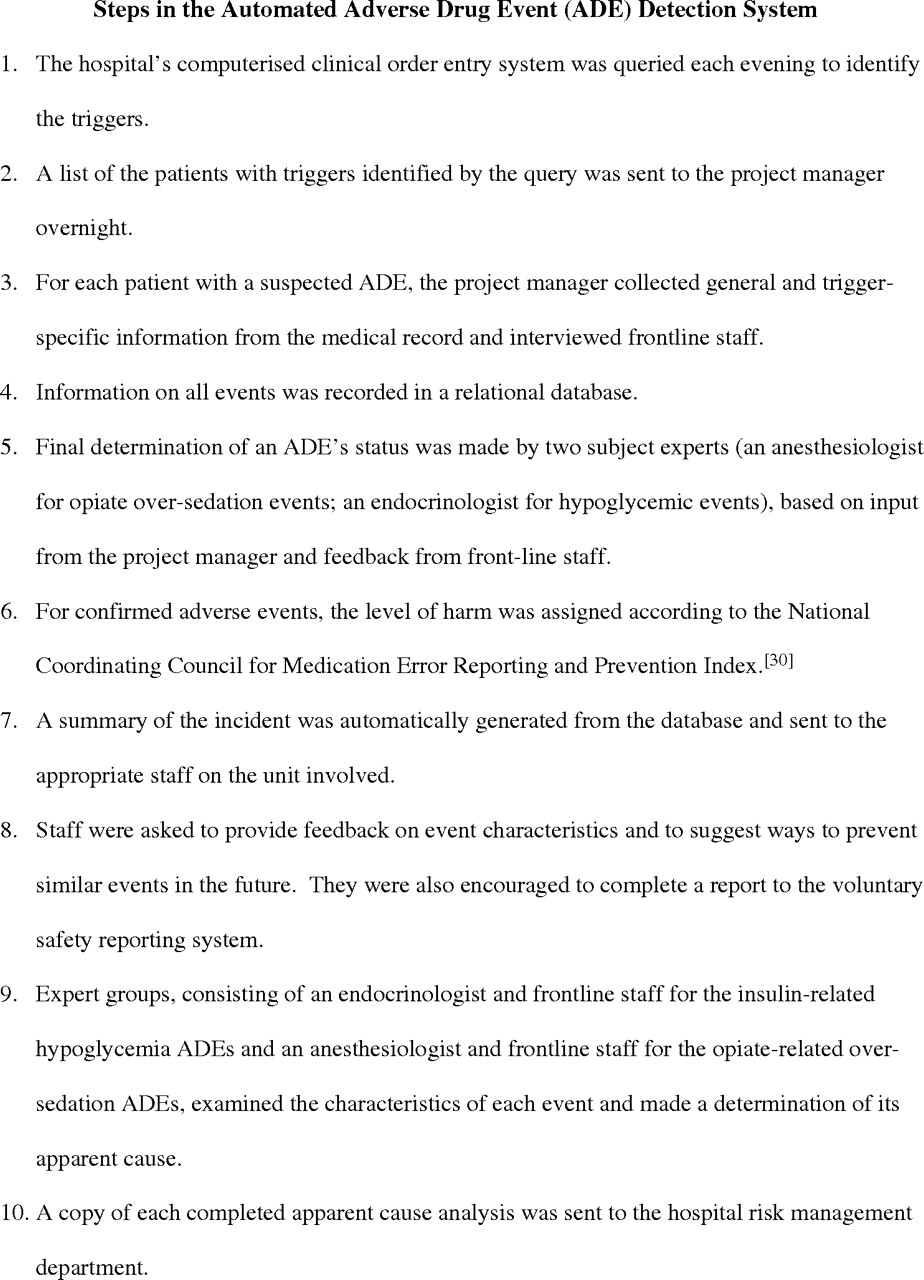
In July 2006, we combined the trigger tool approach with our clinical information system to establish an automated ADE detection programme. Local expert review of our voluntary safety reporting system data and manual paediatric-specific trigger medical record review data found opiate-related oversedation and insulin-related hypoglycaemia to be among the most frequent, potentially harmful ADEs detected. Thus, we initially focused our efforts on developing triggers and event analysis for these ADEs. Naloxone administration was chosen as the trigger for opiate-related oversedation. Administration of an intravenous glucose bolus while also on insulin was the trigger for insulin-related hypoglycaemia.
The steps used to detect ADEs are shown in figure 1. A report of each confirmed incident was sent to the appropriate staff on the unit involved. Attached to the event summary was a feedback form designed to gather information on event characteristics and allow staff to suggest ways to prevent similar future events. The team revised the feedback process and form over a 15-month period.
{kind=link}
Data collection
Data were collected on naloxone triggers identified from July 2006 through March 2008 and dextrose triggers identified from December 2006 through March 2008. The number of reports to the voluntary safety reporting system from July 2006 through March 2008 was also examined.
Analysis
Descriptive patient and hospital characteristics were determined for each ADE. The positive predictive value of each trigger was defined as the number of times a specific trigger independently identified an ADE divided by the number of times a trigger was identified.16 The number of ADEs reported in the voluntary safety reporting system within 24 h was compared with the number of confirmed adverse events identified through the automated ADE detection programme. The apparent causes of ADEs were examined to help pinpoint targets for intervention and improvement.
Human subject protection
The institutional review board approved this project as part of the hospital's quality improvement activities. Written informed consent was not required, provided that no individual patients or providers were identified.
Results
Insulin-related hypoglycaemia
Fifty triggers of glucose bolus while on insulin were identified (table 1). Thirty triggers were determined to signal actual ADEs, resulting in a positive predictive value of 60%. Only 2 of the 30 ADEs (6.7%) were reported using the traditional voluntary safety reporting system before contact by the project manager. The harm was temporary for all patients.
Adverse drug event and patient characteristics
Most events occurred in an intensive care unit and 47% (14/30) of patients had diabetes (table 2). Fifty-seven per cent (17/30) of patients showed decreasing glucose levels before the event without corresponding insulin adjustment. Two (6.7%) of the events resulted from a dosing or administration error.
Insulin-related hypoglycaemia adverse drug event characteristics
After examining the event characteristics, the experts determined the most likely causes of the ADEs to be lack of standardisation in insulin-dosing decisions. They noted that practice varied regarding when and how much to adjust the dose of insulin in response to changing glucose levels. In their opinion, patients receiving continuous-infusion insulin were at increased risk, as were those on dextrose via parenteral nutrition only. Dosing errors and administration errors were found not to be a significant cause.
Opiate-related oversedation
Fifty-nine triggers of naloxone administration were identified (table 1). Thirty-four were determined to signal actual ADEs, resulting in a positive predictive value of 57.6%. Only three (8.8%) of the ADEs were reported in the voluntary safety reporting system before contact by the project manager. Forty-seven per cent (16/34) of events occurred in patients less than 2 years of age. The harm was temporary for 97% (33/34) of patients.
Most of the events occurred in an intensive care unit, the operating room or the post-anaesthesia care unit (table 3). Fifty per cent (17/34) of events occurred on the evening shift. Fifty-six per cent (19/34) of the patients had a surgery and, for these patients, all ADEs occurred within 48 h of surgery. The pain team was involved in the care of 35% of patients (12/34).
Opiate-related oversedation adverse drug event characteristics
The expert group believed the association of ADEs with surgery was important and that lack of standardised pain management in the operating room and post-anaesthesia care unit could be a cause. They noted multiple services writing orders, multidrug regimens and variation in interpretation of patient assessments as potential contributing causes. The expert group also believed variation in practice within 8 h following extubation likely caused some events.
Discussion
We confirmed our hypothesis that harm identified by triggers would provide an opportunity for in-depth analysis of each event to identify causal trends. Conducting an in-depth analysis immediately after each event is a critical step towards future improvements that will be reliable and sustainable. By detecting events within 24 h, the project manager was able to speak with frontline staff while details were still fresh in their memories and to identify and retrieve missing data. Detection of a large number of a particular ADE yielded more information regarding event characteristics, leading to a more sophisticated understanding of causes. This approach also removed the potential bias of studying only events that staff chose to report.
These two ADEs were chosen for initial focus by an adverse event steering committee, composed of representatives from many hospital departments involved in patient safety, based on high volume and risk to patients. To allow for efficient resource utilisation, it was important to develop triggers with a high positive predictive value. Testing was based on a framework of real-time detection and analysis. Naloxone was found to be effective as a trigger. Abnormally low glucose was tested as a trigger but rejected because of its low positive predictive value. Eventually, the committee selected glucose bolus while on insulin. Members were aware that neither trigger was 100% sensitive; however, they believed that substantial information could be gained from an analysis of the detected events.
Detection alone is not sufficient to reduce ADEs. The next step in effective use of trigger tools should be to identify targets for intervention and improvement. Event characteristics may identify specific units, times of day or other factors associated with adverse events. Furthermore, detailed analysis may reveal common themes and hypotheses about system redesign interventions to prevent future events. For example, more than 50% of the children with insulin-related hypoglycaemia were non-diabetic patients. Hyperglycaemia has been shown to be associated with increased mortality in the paediatric intensive care unit and, therefore, an increasing number of children are being managed with insulin drips.31 Our in-depth analysis revealed that this is an area where we need to make changes.
Based on the results of the analysis, redesign interventions can be put into place in the context of a system focused on high reliability and preoccupation with preventing harm.32 This is the strategy that we are now testing with improvement teams for the first two automated triggers. Once successful, we will charter other teams to focus on harm identified by other triggers, based on the frequency and severity of harm detected.
Consistent with previously published results,16 27 the automated trigger system identified more ADEs than the voluntary safety reporting system. For example, the large number of oversedations in the immediate postoperative period was not evident in the voluntary reports but was revealed via the automated trigger system. Improved detection is particularly important in paediatrics, where the reported rate of ADEs is higher than that for adults11 and, therefore, the potential for harm is likely greater.
A limitation of the use of triggers is that they can only identify harm detected through a data point captured by the electronic health record, such as a laboratory value or order. Thus, we will have missed ADEs not associated with a specific trigger. Future trigger systems might include trended data in addition to single data points. Institutions focused on decreasing as much harm as possible may want to continue other forms of event detection, such as voluntary safety reporting and chart review. Also, our study occurred in a single large children's hospital and our results may not be generalisable to other settings. Event detection and improvement require a major commitment of personnel time and resources. Many institutions, like the CCHMC, pursue these efforts as part of their mission to improve quality, but some institutions in very resource-constrained environments may struggle. However, given the cost and quality implications of adverse events, healthcare systems should consider the investment.
In summary, an in-depth analysis of ADEs allowed us to identify their apparent causes. Our experiences may serve as a model for others to build on. Systems to increase ADE detections, including automated event-detection systems, can allow for this in-depth analysis. This increased event detection, combined with analysis of common causes and subsequent improvement interventions, may have the potential to decrease harm.
Acknowledgments
The authors would like to thank Brian Jacobs for his efforts in getting this project started and Arthur Wheeler, David Repaske, Deborah Cornish-Vermaire and Stacey Niehaus for their help in completing it.
References
Footnotes
Funding This work was funded, in part, by a grant from the Agency for Healthcare Research and Quality (grant number U18HS016957). The funding source had no involvement in the study design; collection, analysis or interpretation of the data; writing of the report; or decision to submit this paper for publication.
Competing interests None.
Ethics approval This study was conducted with the approval of the Cincinnati Children's Hospital Medical Center.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Quality lines