Article Text

Abstract
Background: Intravenous (IV) medication errors are frequent events. They are associated with considerable harm, but little is known about their causes. Human error theory is increasingly used to understand adverse events in medicine, but has not yet been applied to study IV errors. Our aim was to investigate causes of errors in IV drug preparation and administration using a framework of human error theory.
Methods: A trained and experienced observer accompanied nurses during IV drug rounds on 10 wards in two hospitals (one university teaching hospital and one non-teaching hospital) in the UK. Information came from observation and talking informally to staff. Human error theory was used to analyse the causes of IV error.
Results: 265 IV drug errors were identified during observation of 483 drug preparations and 447 administrations. The most common type of error was the deliberate violation of guidelines when injecting bolus doses faster than the recommended speed of 3–5 minutes. Causes included a lack of perceived risk, poor role models, and available technology. Mistakes occurred when drug preparation or administration involved uncommon procedures such as the preparation of very small volumes or the use of unusual drug vial presentations. Causes included a lack of knowledge of preparation or administration procedures and complex design of equipment. Underlying problems were the cultural context allowing unsafe drug use, the failure to teach practical aspects of drug handling, and design failures.
Conclusions: Training needs and design issues should be addressed to reduce the rate of IV drug preparation and administration errors. This needs a coordinated approach from practitioners, regulators, and the pharmaceutical industry.
- human error theory
- medication errors
- intravenous treatment
Statistics from Altmetric.com

The intravenous (IV) administration of drugs is a complex process and errors frequently occur. For example, in a recent study on 10 wards in two UK hospitals we found that errors occurred in almost half the IV drug preparations and administrations, 1% of which were severe and 58% moderate.1 Box 1 summarises the main findings of this study. Similar rates of medication error have been reported in other studies.2–5 Anecdotal evidence indicates the harmful nature of IV errors.6,7
Box 1 Summary of results of ethnographic study on the incidence, types, and clinical importance of IV drug preparation and administration errors1
Incidence of errors
-
One or more errors occurred in the preparation and/or administration of 212 of 430 IV doses observed (error rate 49% (95% confidence interval 45 to 54)).
-
Preparation errors occurred in 32 IV doses (7%), administration errors in 155 doses (36%), and both types of errors in 25 doses (6%).
Potential clinical importance
-
Errors were potentially severe in three doses (1%), potentially moderate in 126 (29%), and potentially minor in 83 (19%).
Common types of IV drug errors
-
An error rate of 73% occurred when giving bolus doses (172 errors in 235 observed administrations). The most common error was giving bolus doses too quickly (163 of 172 (95%)), about half of which were judged to be of potential moderate severity.
-
An error rate of 14% occurred when preparing drugs that required multiple steps (50 errors in 345 observed multiple step preparations).
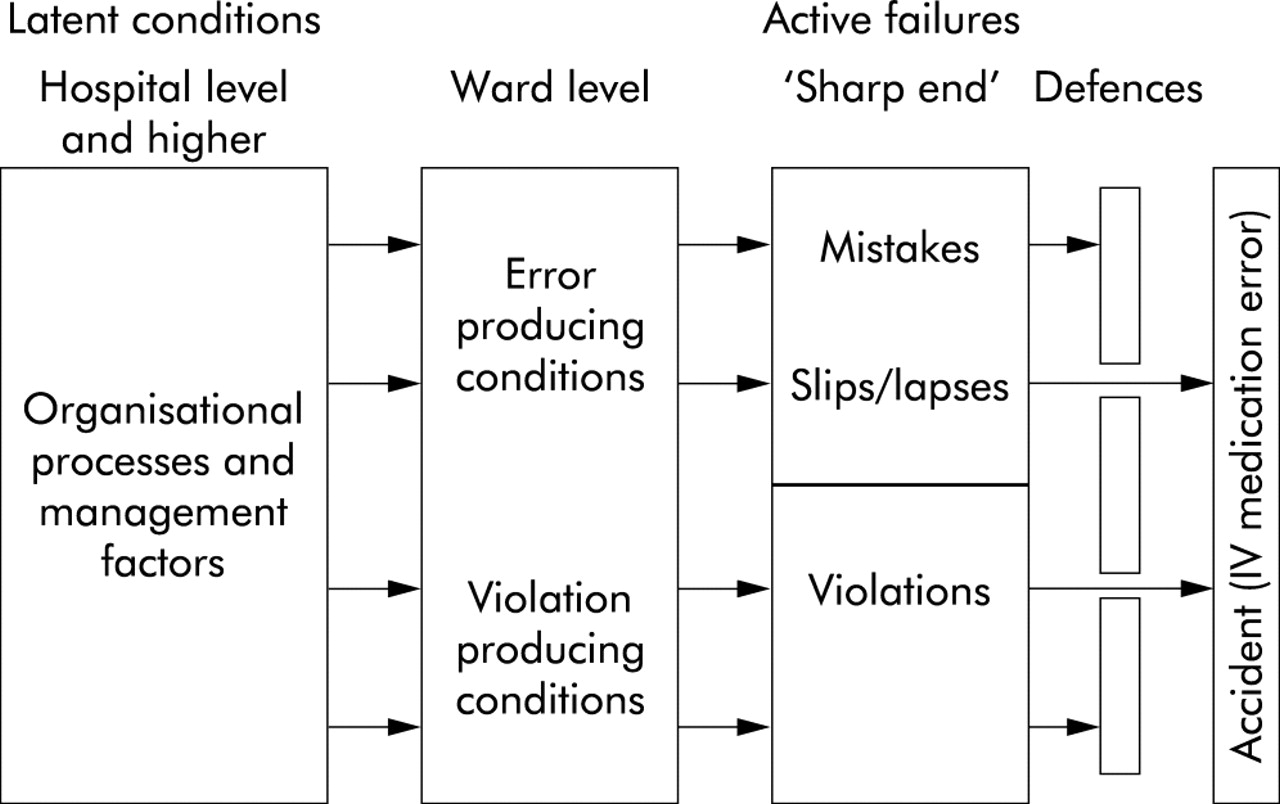
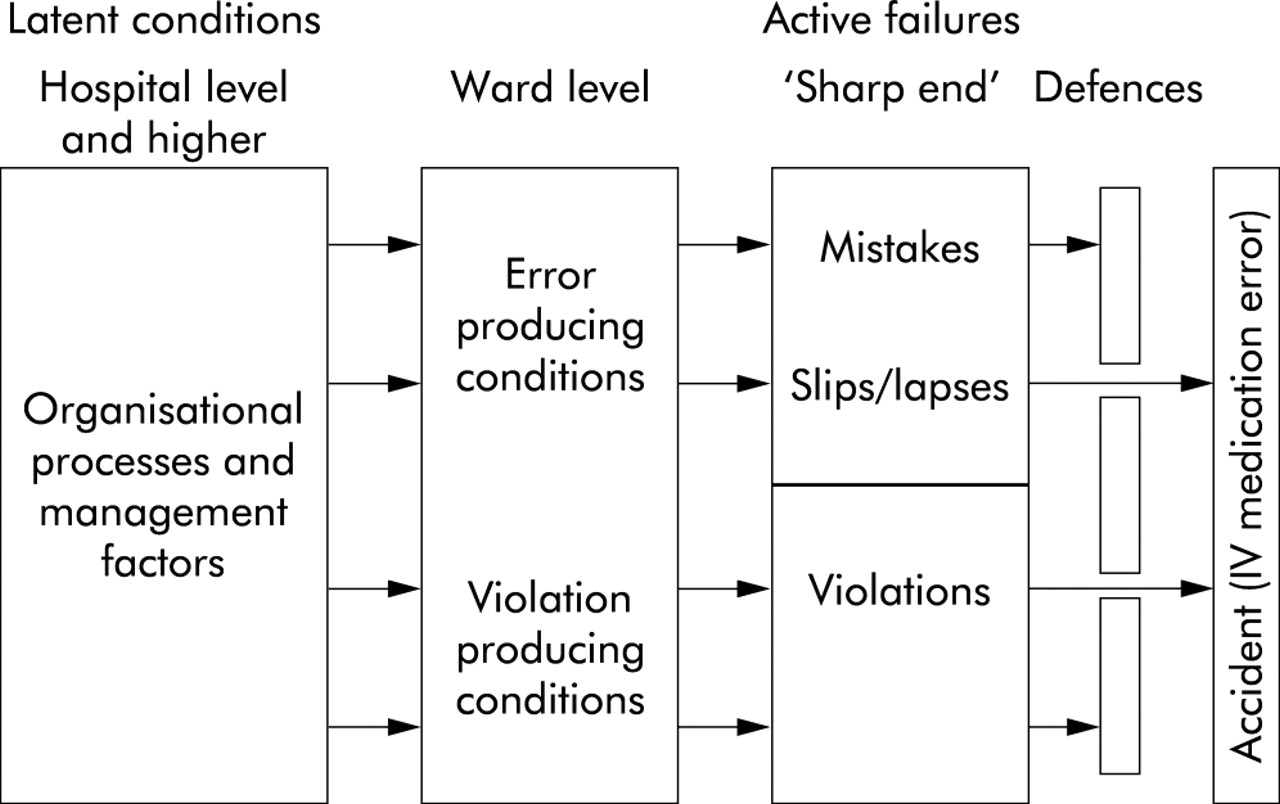
We do not know why IV errors occur. Investigating the causes of errors is the first step towards error prevention.8 Studies on adverse events in medicine have suggested that common causes of medication errors in general include equipment problems; communication problems; lack of training, experience and knowledge; faults in the system; and personal problems.9,10 To what extent such factors contribute to IV medication errors remains unknown. Human error theory is increasingly used as a theoretical base to investigate adverse events in medicine,10–14 but this approach has not yet been applied specifically to the study of IV errors. Investigations of large scale accidents in high risk industries found that the design of systems, pre-existing organisational factors and the conditions, conventions and procedures for the use of technology place human operators in a position in which human errors can result in disasters. Based on such research, Reason developed the model of organisational accident causation (fig 1).12 Actions at the “sharp end”—for example, the administration of the wrong drug—are the final triggers of an accident. Analysing such active failures reveals the working conditions (error and violation producing conditions) at the time of the accident and the organisational processes and management decisions which contributed to the accident.
{kind=link}
Reason’s four stage model of human error theory (adapted from reference 12). Human errors (mistakes = failures at the planning or problem solving stage of a task, slips/lapses = failures at the execution stage of a task); violation = deliberate deviation from safe operating practices, recommendations or guidelines, but no intention of adverse consequences.
Interviews and document review are commonly used to analyse the causes of adverse events,10,13,14 but these methods rely on adverse events being documented or reported. Previous research and pilot work has shown that nurses are often unaware of the occurrence of medication errors.15,16 An ethnographic approach combining several methods, including observation of actual practice and interviews, provides an insight into the behaviour of which participants themselves may be unaware.17 It overcomes the discrepancy between what people say and what they actually do.18 This research methodoffers the advantage that the context can be explored at the time of the error and many of the conditions which contribute to errors, as outlined by human error theory, can then be identified in this context.
We conducted an ethnographic study to investigate IV drug errors in two UK hospitals. A detailed analysis of the incidence, types, and clinical importance of the IV drug errors has been reported elsewhere.1 Here we report the identification of causes of IV drug preparation and administration errors using human error theory as a framework.
METHODS
Setting
Some of the methods used in this study have been reported in detail previously.1 Briefly, a purposive sampling strategy was used to collect data in a range of different hospital settings. Ten wards (including intensive care, paediatrics, surgery, cardiology and nephrology) were studied in two hospitals (a university teaching hospital and a non-teaching hospital) in the UK. Both hospitals operated a typical ward pharmacy service19 in which doctors wrote prescriptions on formatted inpatient drug charts and nurses used the charts to determine the doses to be given and to record the administration of drugs. Pharmacists visited wards each weekday to order drugs that were not stocked on the ward and to review the appropriateness of prescribing. IV medication in general was prepared and administered on the wards by nursing staff, with the exception of cytotoxic medication which was prepared centrally by the pharmacy department. Nurses had to attend a one day IV training course before they were allowed to administer IV medication. An IV drug administration guide outlining instructions for drug preparation and administration was available on the ward at each site.
Data collection and analysis
The human error framework for data collection and analysis was adapted from methods used to investigate clinical incidents.11 Data were collected on 6–10 consecutive days, including weekends, on each ward between June and December 1999. One of us (KT), a pharmacist trained and experienced in observation based medication error research, accompanied nurses during IV drug rounds. An IV medication error was defined as any deviation in the preparation and/or administration of the IV medication from the doctor’s prescription, the hospital’s IV policy, or the manufacturer’s instructions. We presented the study to staff at ward level as a research project investigating common problems of IV drug preparation and administration. This disguised, observation based method has been shown to be valid for identification of medication errors.20 Permission to observe was obtained from each individual nurse.
The observer recorded details of each IV drug preparation and administration. Additional information came from observation and talking informally to staff. Observations were guided to record information on the chain of events that led to the error and the actions of those involved. Protocols which have been used for interviews in previous studies were applied to the observation technique used in the present study.11 The researcher intervened in a discreet and non-judgmental manner when she became aware that an erroneous medication likely to cause harm to the patient was going to be administered. These incidents were still included as medication errors. The researcher’s records were checked and completed for each IV drug within 24 hours of leaving the ward. Notes of observation and conversation for each error were transcribed and read by both authors. Reason’s four stage model of human error theory12 and the framework of categories developed by Vincent et al11 formed the basis for coding the data (fig 1); the categories were adapted to the analysis of IV drug preparation and administration errors.16 Data were coded by KT and coding was checked by NB. Disagreements were discussed and resolved. Each case of IV medication error was analysed to identify the main active failure and the factors contributing to this error.
Active failures were categorised as human errors (slips/lapses and mistakes) or violations, defined as follows:
-
Slips or lapses were failures in the process of executing a task. The observed healthcare professional had an adequate plan, but the action did not proceed as intended because of recognition, attentional, memory, or selection failures.
-
Mistakes were failures at the planning or problem solving stage of a task.
-
Violations were deliberate deviations from safe operating practices, recommendations or guidelines, but with no indication that any adverse consequences were intended.
Error and violation producing conditions were defined as factors at the ward level which led to active failures. Latent conditions included any underlying organisational and management failures which contributed to error and violation producing conditions. The use of human error theory as our theoretical base allowed us to explore systematically the chain of events leading to IV drug errors. From these data the main causes of errors were identified.
Ethics committee approval was obtained from both study hospitals. The study was also approved by ward managers as well as nursing and pharmacy directorates.
RESULTS
One hundred and thirteen nurses were observed on 76 study days. A doctor was observed on one occasion when he took over drug administration from a nurse. A total of 483 IV drug preparations and 447 drug administrations were observed and 265 errors were identified. A main active failure was identified in 256 (97%) of the errors. There were 25 (10%) slips and lapses, 60 (23%) mistakes, and 171 (67%) violations.
Slips, lapses and mistakes
Most drug preparations followed the same procedure—namely, injection of a solvent (about 10 or 20 ml) into the drug vial and drawing up the dissolved drug. Slips included the failure to notice that a drug had not dissolved completely or misreading a drug label. For example, a nurse drew up the whole content of a heparin vial which would have resulted in a five times overdose. When the observer pointed out the error the nurse said: “No, there are 25 000 units in the whole vial”. After checking the label on the vial she said: “I am sure that I had a vial with 25 000 units in 5 ml last time” (A34, general medical ward, university teaching hospital). Mistakes frequently occurred when the preparation or administration of the drug involved uncommon procedures. A typical example was the preparation of a multivitamin drug which required two components supplied in two separate vials to be mixed. The nurse administered only one of the vials. She explained to the observer: “I saw vials 1 and 2 but I thought number 2 was the diluted version of number 1, therefore I administered number 2” (D31, coronary intensive care unit, university teaching hospital).
Error producing conditions
Table 1 gives a detailed breakdown of 136 factors which contributed to mistakes, slips and lapses. Handling and design of technology were by far the most common, contributing to 67 (79%) and 27 (32%) human errors, respectively. Lack of knowledge of preparation or administration procedures were frequent failures in handling technology. On a neonatal ward incorrect procedures were used to measure very small volumes of <1 ml of drug solution. The drug solution contained in the hub of the syringe was also administered to the patient which resulted in a two to three times overdosage.21 Lack of knowledge of correct preparation procedures contributed to the error involving the multivitamin preparation outlined above.
Error producing conditions (n=136) relating to 85 human errors (mistakes, slips and lapses)
A dosing error due to incorrect preparation procedures handling a Monovial is described in box 2. Lack of knowledge of how to handle electronic infusion equipment was also observed once. The nurse on the neonatal intensive care unit showed KT how to set up a particular syringe driver for an infusion of caffeine. She explained: “You measure the length of the syringe, multiply the length by three to calculate the appropriate infusion rate.” She then set up the syringe driver in this way. This resulted in an infusion time of 3 hours instead of 20 minutes because the measurement of the length of the syringe should have been divided by three (E33, neonatal intensive care unit, university teaching hospital).
Box 2 Examples of error producing conditions
Handling technology: lack of knowledge of preparation procedure and complex design of technology
A nurse prepared a prescribed dose of 250 mg imipenem from a Monovial containing 500 mg imipenem. She connected the vial directly to an infusion bag, transferred fluid into the vial from the infusion bag, dissolved the drug, and transferred about half of the reconstituted drug solution back into the infusion bag (B24, renal ward, university teaching hospital). Comment: This was likely to result in the patient receiving an incorrect dose.
Handling technology: lack of communication between nurses and inadequate use of technology
Two nurses were on the late shift; one carried out the oral drug administrations and selected all the drug charts of patients who were due to receive IV medication, and the other handled the IV drug administrations. Two drug charts belonging to patients who were due to receive IV medication were placed next to a pile of drug charts of patients who had already received their IV medication. Neither nurse realised that these patients still had to have their medication. (G69–71, general surgical ward, non-teaching, general hospital).
The design of the technology itself—such as complicated drug vial presentations, preparation or administration equipment—was the second most common error producing condition. As outlined above, the small label on the heparin vial made it difficult to distinguish different strengths of the drug, contributing to selection of the wrong vial. Lack of knowledge in handling technology and design of technology were frequently observed to contribute to the same error. This is illustrated by the case involving the multivitamin preparation in which the two different types of vials containing the two components were almost identical in appearance. The design did not indicate that the two vials had to be mixed before administration. The complex design of the syringe driver, which required the infusion rate to be calculated by measuring the length of the syringe, contributed to the wrong administration rate being set.
Medication was omitted because of failures in communication in 14 errors (16%). This occurred when patients were transferred between wards and information on drug administration was not communicated. Communication problems between doctors and nurses included ambiguous hand written prescriptions. These cases also indicated failures in adequately using and checking patient’s drug charts (box 2).
High workload and distractions when carrying out several tasks at the same time were observed in 13 errors (15%). On an intensive care unit a patient’s continuous infusion of adrenaline ran out. There was a delay of about 10 minutes before the new preparation was ready for administration. The patient required a bolus dose of adrenaline and midazolam in the meantime. The nurse responsible for this particular patient explained to the senior nurse that she had not paid attention to the infusions as a ward round had been going on. There was a lack of supervision of the nurse who was an agency nurse and had returned to clinical work during the previous 6 months after working in industry for several years (I21, intensive care unit, non-teaching, general hospital). Similarly, a lack of supervision of student nurses was identified in a few cases.
Patient related factors included a lack of venous access or unwillingness to cooperate with drug administration.
Violations
Most violations (n=168, 98%) were fast administration of bolus doses (injections administered faster than the recommended speed of 3–5 minutes); in 116 cases (69%) the bolus dose was given in less than half the recommended time. The majority of bolus dose errors were judged to be clinically significant.1 Conversations with nurses showed that they knew the correct speed of administration but deliberately deviated from these guidelines. A typical comment was: “I do not take as long as [3 minutes]” (H19, general medical ward, non-teaching hospital). More than two thirds of observed bolus doses (n=168, 72%) were administered too fast, suggesting that these were routine violations, “cutting a corner whenever the situation allows this”, as Reason puts it.12
Violation producing conditions
Nurses explained that fast administration of low doses was without risk. A typical comment (which also shows confusion over the source of risk) was: “I am quite happy to give 80 mg [furosemide] as a bolus but I would administer 250 mg as an infusion” (A31, general medicine, university teaching hospital). However, the lack of knowledge about medication by nurses sometimes led one to question the validity of their risk assessment.
Examples of poor supervision were seen when nurses not qualified to carry out IV drug administrations were taught. A junior nurse took more than 3 minutes to administer a bolus dose, a senior nurse laughed at her and told her: “You should give the drug over 3 minutes not over 30 minutes” (A29, general medical ward, university teaching hospital). In some cases, especially on the paediatric and neonatal wards, the administration of small volumes over more than 1 minute was technically difficult.
Latent conditions
Lack of appropriate training and design issues were identified as the two main latent conditions. Unlike the theoretical background, the practical aspects of IV drug preparation and administration were neither formally taught nor assessed in the two study hospitals. Nurses in general learnt how to prepare and administer IV medication from each other on the wards (box 3). There were no guidelines regarding content and quality of such training; in particular, uncommon preparation procedures did not seem to be covered. Pharmacists were not directly involved in the preparation or administration of IV medication on the wards and knew little about the practical problems encountered (box 3). Nurses seemed to pass on bad practice, so deviations from guidelines—such as the fast administration of bolus doses—became accepted practice, creating a cultural context of unsafe drug use. Most wards had no separate room or a dedicated area for drug preparation. IV medications were prepared in the middle of a busy ward and nurses were frequently interrupted and distracted during the process. Overall, safe handling of IV drugs had a low priority in the two hospitals studied.
Box 3 Examples of latent failures
Lack of training
KT: “What kind of training have you undergone [in IV drug preparation and administration]?” Nurse: “I have attended a one day study day where we had a lecture by a pharmacist mainly on pharmacological issues of drugs and then did calculations, this has been quite useful. I was supposed to be supervised in preparation and administration for a week at least, but this has been done only a few times” (G28, general surgical ward, non-teaching, general hospital).
Lack of involvement of pharmacists
KT: “Do you know about this preparation problem [preparation using Monovials (box 2)]?” Pharmacist: “Ward pharmacists do not know what is supplied to the wards and therefore we don’t know about the problems that the ward staff might have with preparations” (observer’s notes on a conversation with the ward pharmacist of the renal ward, university teaching hospital).
We identified a range of design failures of technology including ambiguous labelling of ampoules and complex design of drug vial presentations and infusion equipment. Two latent conditions contributed to this situation: (1) pharmacists were unaware that they supplied drug products which created problems and (2) the pharmaceutical industry developed and produced drugs and equipment which did not support safe use.
DISCUSSION
We have explored the causes of IV drug errors using a framework of human error theory. Observation of actual practice has shown that IV drug errors are not only caused by the immediate individual act, but a range of organisational and managerial issues—including training, cultural context, choice of product, purchasing policy, and design of technology—also contribute to errors.
Our study confirms earlier concern about nurses’ lack of training in handling IV medications.22,23 Clinical pharmacists have been identified as the key health professionals to ensure safe medicine use.24 The current ward pharmacy system with daily visits to the clinical areas19 places the pharmacist in a good position to recognise training needs and to address them. Such a multidisciplinary team approach may create a cultural context which supports safe drug use. Pharmacists should also anticipate problems with certain drug vial presentations or complex preparations. In our study these functions did not seem to happen, and pharmacists need to be more engaged with ward practice.
Attempts to reduce the harm caused by IV errors in the past have focused on restricting choice and removing from the nurse the task of making up the drug. Restricted supply of strong potassium chloride to reduce medication errors was recommended a quarter of a century ago,25 and stocking only one strength of morphine ampoules on paediatric wards has been successful in preventing errors involving the selection of the wrong ampoule.26 Other changes to reduce medication preparation errors include the central preparation of IV medication,25 but the evidence base for the success of such a service is currently weak.27–30
Design issues such as ampoules which look similar31,32 and the complex design of infusion pumps33 have previously been recognised as risk factors. We have also shown that the failure to handle complex drug vial presentations correctly resulted in medication errors. Our study again shows that the manufacturer’s role should be to supply products with a high safety standard when in general use.
Key messages
-
Guidelines on the safe speed of injection of bolus doses were deliberately violated because of a lack of perceived risk, poor role models, and available technology. This contributed to a cultural context which allowed unsafe drug use.
-
Mistakes occurred when drug preparation or administration deviated from common procedures because of a lack of knowledge of these special procedures and the complex design of the technology.
-
The practical aspects of IV drug preparation and administration were insufficiently taught at the hospitals studied. Pharmacists knew little about the practical problems at ward level.
-
A coordinated approach from practitioners, regulators, and the pharmaceutical industry is needed to address training needs and design issues.
The application of concepts and techniques of human error theory to problems in medicine was suggested in the 1970s34 but the pharmaceutical industry does not really seem to have espoused the approach. One way forward for the industry would be to apply a framework of human error theory at the product design stage, including consultations with clinical practitioners and observations in practice. The licensing process should also consider any differences between the product used in trials and the final presentation. In addition, the use of the product needs to be formally assessed during post-marketing surveillance.
The ethnographic approach using a practitioner as observer offered several advantages. We could identify deviations from practice that staff themselves did not notice and would not have brought up at interview, and we did not have to rely on their memory or fear their censoring of the data. We did not have to use records designed for a different purpose. We chose two contrasting hospitals and a careful cross section of wards; it is recognised that the generalisability of these findings has yet to be established, but the authors have worked in several hospitals and think the findings not uncommon. There is often concern that observation changes practice but there is little evidence of this in practice.20 On the other hand, while conversations with staff were part of the study methodology, we did not interview them in depth and some personal factors, such as those that have been shown to contribute to prescribing errors,13 may have been missed.
As is often the case with error, it is not those who make the error who should be the focus but the whole system of work and technology around them. While nurse training would have some effect on errors, it needs to be linked to prescribing policies, purchasing of medicines, and pharmacists who are aware of technologies and medication presentations available on their wards. However, in this case responsibilities also spread outside the National Health Service (NHS) to the pharmaceutical industry, who could do more at the design stage to reduce errors and to monitor and develop the use of their products. No single act will significantly reduce the incidence of IV errors; there needs to be a coordinated approach from practitioners, regulators, and the pharmaceutical industry.
Acknowledgments
KT received a grant from the School of Pharmacy, University of London. The authors are indebted to the staff of the two study hospitals for their enthusiastic support.
REFERENCES
Footnotes
-
See editorial commentary, pp 326–7
-
This study was funded by The School of Pharmacy, University of London. The sponsors had no influence on study design, data collection, data analysis, data interpretation, or writing of the report.
-
The study was designed by both authors. KT collected the data and analysed it with NB. The final report was written by both authors.
-
Conflict of interest: none declared.
Linked Articles
- Commentary
- Action points