Article Text

Abstract
Background Immunocompromised children are at high risk for central line-associated bloodstream infections (CLABSIs) and its associated morbidity and mortality. Prevention of CLABSIs depends on highly reliable care.
Purpose Since the summer of 2013, we saw an increase in patient volume and acuity in our centre. Additionally, CLABSIs rates more than tripled during this period. The purpose of this initiative was to rapidly identify and mitigate potential underlying drivers to the increased CLABSI rate.
Methods Through small tests of change, we implemented a standard process for daily hygiene; increased awareness of high-risk patients with CLABSI; improved education/assistance for nurses performing high-risk central venous catheter procedures; and developed a system to improve allocation of resources to de-escalate system stress.
Results The CLABSI rate from June 2013 to May 2014 was 2.03 CLABSIs/1000 line days. After implementation of our interventions, we saw a significant decrease in the CLABSI rate to 0.39 CLABSIs/1000 line days (p=0.008). Key processes have become more reliable: 100% of dressing changes are completed with the new two-person standard; daily hygiene adherence has increased from 25% to 70%; 100% of nurses are approached daily by senior nursing for assistance with high-risk procedures; and patients at risk for a CLABSI are identified daily.
Conclusions Stress to a complex system caring for high-risk patients can challenge CLABSI rates. Identifying key processes and executing them reliably can stabilise outcomes during times of system stress.
- Root cause analysis
- Quality improvement methodologies
- Patient safety
- Paediatrics
- Nosocomial infections
Statistics from Altmetric.com
Introduction
Patients receiving therapy for cancer, or undergoing haematopoietic stem cell transplantation (HSCT) for immunologic disorders, bone marrow failure syndromes, genetic syndromes or malignancy, are at increased risk of a bacterial infection.1 Patients receiving these therapies oftentimes have a central venous catheter (CVC) for medication administration, transfusions and frequent blood draws.2 Central line-associated bloodstream infections (CLABSIs) are among the most serious complications in children receiving chemotherapy and undergoing HSCT.3 CLABSIs lead to prolonged hospitalisation, intensive care admissions, prolonged antibiotic treatment and increased mortality.4 ,5 CVC maintenance care has been shown to be effective in reducing CLABSIs in adult and paediatric intensive care units, and in the paediatric haematology oncology patient population.4 ,6–9
Microsystem stress can arise from high patient volumes and acuity, which results in high nursing workload. High workload has been shown to be associated with suboptimal patient care,10 ,11 influence care provider’s decisions to perform various procedures12 and may lead to reduced patient satisfaction.13 High workload may also lead to poor nurse–patient communication,14 impaired nurse–physician collaboration,15 nurse burnout and job dissatisfaction.10 Additionally, poor staff adherence to CLABSI prevention practices and increased nursing workload are important risk factors to healthcare-associated infections.16–18
From July 2013 to May 2014, we saw a marked increase in patient volume and acuity in the Cancer and Blood Diseases Institute (CBDI) at Cincinnati Children's Hospital Medical Center (CCHMC). During this period, the CLABSIs rates more than tripled. We identified multiple elements, including system stress, which may have contributed to the increased CLABSI incidence, and rapidly implemented interventions to decrease the rate (table 1).
Identification, analysis and interventions to identify and mediate variables that may be associated with the increased CLABSI rate
Context
The CBDI at CCHMC includes both a Hematology Oncology (Hem/Onc) unit and a Bone Marrow Transplant (BMT) unit. The BMT unit consists of a 36-bed, highly complex intensive care environment. The BMT programme performs 95–110 transplants annually with the majority being allogeneic. Average length of stay varies based on the type of transplant and ranges from 25 to 70 days. The Hem/Onc unit has a capacity of 32 patient beds, providing specialised haematology, oncology and vascular malformation care to patients from infancy through adulthood. Approximately 350 new/relapse referral patients enter the cancer programme each year. The CBDI consists of 35 attending physicians, 15 fellows, 20 hospitalists and 30 nurse practitioners. The clinical team consists of 250 registered nurses (RNs) and 60 patient care assistants (PCAs), highly trained pharmacists, dieticians, pain management physicians, psychologists and physical and occupational therapists. Additionally, the CBDI includes the Patient and Family Wellness Center, consisting of child life specialists, school intervention specialists, integrative care, psychology, social work and behavioural medicine.
Local problem
Ten years ago, prior to the quality improvement work, the combined CLABSI rate of CCHMC BMT and Hem/Onc units was as high as 4.7 infections/1000 line days. Early on, the most significant intervention implemented was the CLABSI maintenance bundle, which combined a series of evidence-based practices around hygiene and care of the line and dressing. CLABSI rates were reduced to 3.05 infections/1000 line days. Over the next several years, an advanced bundle was developed in conjunction with a national haematology/oncology CLABSI focused task force that addressed the special care needs of the immune compromised paediatric population. The components and results of this collaborative were described by Bundy et al.6 The impact at CCHMC was demonstrated in calendar years 2011 and 2012 as reflected in the lowest rates realised by the units with a CLABSI rate of 0.62 infections/1000 line days for each year. Subsequently, the CLABSI rate from June 2013 to May 2014 increased by 300% to 2.03 infections/1000 line days.
Methods
At the end of May 2014, we established a multidisciplinary CLABSI oversight task force consisting of key stakeholders, including senior hospital leadership, physicians, nursing leadership, RNs, Infection Control, Vascular Access Team members and PCAs. The team's focus was to identify and mitigate potential underlying causes of the increased CLABSI rate through analysis of current and historical CVC care practices; review of published recommendations and guidelines; quantitative and qualitative analysis of patient, environment, and healthcare delivery system variables; and rapid implementation of interventions based on plan-do-study-act (PDSA) testing. This analysis, PDSA testing and rapid intervention occurred over a 2–3 week period.
Assessment of patient-specific variables
Prior to May 2014, the nursing and physician team did not pre-emptively identify patients with CLABSI risk factors, and all CLABSIs were reviewed twice weekly by the CBDI CLABSI prevention team. In order to determine variables associated with CLABSIs, we performed an in-depth analysis on all infections within the previous year, and conducted qualitative nursing interviews to determine patient variables that may be associated with failures in the current line care standards.
Forty-one patients (21 Hem/Onc and 20 BMT) were diagnosed with a CLABSI from July 2013 to May 2014. Sixty-seven per cent (14 of 21) of Hem/Onc patients with a CLABSI were diagnosed with acute myeloid leukaemia (AML), relapsed AML, infant acute lymphoblastic leukaemia (ALL) and high-risk recurrent neuroblastoma (patients with these diagnoses represent 17% of our oncology population). Seventy-one per cent (15 of 21) of oncology patients with a CLABSI had an absolute neutrophil count (ANC) of less than 500, 62% (13 of 21) had received blood products in the 72 h prior to development of a CLABSI and 24% (5 of 21) had underlying skin integrity issues, including skin breakdown. There was no significant association with underlying diagnosis and development of a CLABSI in the BMT population. Fifty per cent of patients (10/20) developed a CLABSI prior to stem cell engraftment while neutropenic and 80% (8/10) of BMT patients that developed a CLABSI after engraftment had graft versus host disease (GVHD) at the time of infection (see online supplementary figures S1–S4). Qualitative discussions with the nursing staff identified patient behavioural issues, such as aggression, as a risk factor for sterile field contamination during line and line dressing changes. Additionally, they identified dressing and line complications (eg, broken lines) as a potential factor that could increase risk to a CLABSI.
Intervention: rapid identification and analysis of CLABSIs and variables associated with CLABSI
Based on our analysis, we identified the following variables to be associated with CLABSIs: GVHD (gut or skin), patients within 15 days after stem cell transplant, high risk neuroblastoma, AML, relapsed ALL, dressing/line concerns or issues within the past 72 h, the most recent ANC <200, fever >38 in the last 48 h and patients with behavioural issues. Patients with these complications constitute between 10% and 20% of the patients on each floor at any given time, and patients with these issues were designated as ‘high-risk for CLABSI’.
High-risk patients were discussed during daily shift changes, which heightened awareness across the nursing team. The provider team was also informed of the high-risk patients who were fully evaluated during multidisciplinary rounds. Risk factor identification enabled the team to move beyond mitigation and into the realm of prediction. Patients with factors identified as being high risk were identified as ‘CLABSI watchers’. Once identified, pre-emptive measures were determined and implemented. For example, a patient with frequent dressing changes due to dry, scaly skin triggered a consult with the hospital's dedicated vascular access team.
Additionally, the CBDI CLABSI prevention team performed immediate preliminary investigation upon electronic notification of each positive blood culture. Both the medical and nursing teams were alerted, allowing for early intervention in the event of issues with prevention standard compliance and/or associated medical issues requiring attention.
Identification of variables that may be associated with increased CLABSIs from frontline staff
We conducted a failure mode and effect analysis (FMEA) with RNs, PCAs and unit leadership through small group qualitative discussions to identify potential causes of the increased CLABSI rate, and to potentially identify stressors to our healthcare delivery system. Our key learnings were that frontline staff felt a substantial rise in workload from the increased patient acuity and census; that patients enrolled in a phase I study required additional time and efforts; and that non-English speaking families needed interpreter services, which required additional time to overcome communication barriers. Float nurses and recent nursing graduates identified dressing and line changes as the most complicated procedures, requiring additional assistance, and some staff felt uncomfortable asking for help with procedures.
From these small group settings, we determined that high acuity patients, phase I patients and non-English speaking patients put additional stress on the healthcare delivery system; many providers required additional education and instruction on line care; and many providers felt uncomfortable asking for assistance.
Assessment of variables that may be associated with microsystem stress
To quantify the microsystem stress the nurses discussed, we evaluated multiple healthcare delivery system variables from July 2011 to May 2014 including number of new patients, new regional and international referrals, number of active phase I patients, average daily census (ADC), average daily float nurse hours, number of chemotherapy doses administered and number of transplants. We also evaluated nursing staff experience on the units through analysis of RN by analysing RN licensed years.
From fiscal year 2013 (July 2012–June 2013) to fiscal year 2014 (July 2013–June 2014) the average daily float nurse hours increased from 43 to 104 h per day; monthly ADC increased from 52 to 63; the number of new relapsed refractory oncology patient referrals went from 3.6 to 6.9 per month; and the number of active phase I patients went from a median of 14 to 25 (see online supplementary figure S5). During the same time our average monthly international referral rate went from 0.5 (range 0–1) to 2.2 (range 0–8). From 2012 to 2014, with sustained growth, the percentage of RNs with less than one licensed year increased from 15 to 33.
Intervention: system stress mediation and CVC line care
CVC line care
A strong emphasis was placed on CVC care practice re-education for all CBDI RNs with special attention centred on CVC line maintenance. The education was delivered by a core group of experienced nurses to all staff and float RNs within a 3-week timeframe. A more in-depth CVC formal session was administered to the inpatient RNs, starting with those hired during fiscal year 2012. During the formal session there were a total of four hands-on demonstration stations focusing on peripherally inserted central catheter dressing changes, CVC tunnelled lines and accessing/de-accessing CVC implanted ports. Proper hand hygiene, personal protective equipment and sterility were emphasised at each station along with the proper surface selection to set up the sterile field.
Two-person dressing changes
A CVC dressing change is a sterile and meticulous procedure that can be complicated by patient and environmental factors potentially leading to CLABSIs. The nursing groups identified dressing changes as the most complicated and difficult procedure to perform with the highest risk of contamination. Historically, the need for a second person during a dressing change was determined based on difficulty, patient's ability to cooperate or RN comfort level with the procedure. To promote adherence to the dressing change procedure, the requirement of having a second nurse with all CVC dressing changes was implemented. During the two-person dressing change procedure, an experienced RN assists the patient's assigned RN with the CVC dressing change. This is a non-punitive and non-judgemental encounter. The second RN monitors adherence to the procedure and provides both coaching and praise. Compliance with the two-person dressing change increased to 100% within the first month of intervention.
Safety coach
Safety coaches (SCs) are experienced RNs committed to safety and accountability, who perform continuous real-time behaviour-based monitoring and coaching. Our FMEA revealed nursing concerns and uneasiness over asking for help with complicated procedures. To mediate this concern, we adjusted the responsibilities of the SC to be more proactive. During each shift, the SC proactively approached each RN on the unit to discuss upcoming procedures and volunteered to help. When needed, the SC and bedside RN completed the procedures together, including two-person dressing changes.
Increased frequency of CLABSI prevention standards rounding
CLABSI prevention standards rounding was initiated in December 2013 and included unit leadership, unit-specific CVC champions and senior nurses. Rounding consisted of evaluating on a weekday basis the following defined components of CVC care: CVC dressing integrity, completion of cap and line changes within specified policy defined timeframes and presence of passive alcohol impregnated devices on all open ports on the line. After the increase in CLABSIs in May 2014, rounding increased to 7 days a week.
Additional experienced nursing hours in times of high stress
After June 2014, we continued to monitor system stressors in real time including ADC, float nurse hours, active phase I patients in the CBDI, regional and international referrals, number of new relapsed/refractory oncology patients, number of monthly HSCTs and daily subjective microsystem stress assessment provided by the charge nurse. Through small, qualitative testing, we determined that additional nursing support from experienced paediatric haematology/oncology/BMT nurses significantly helped during times of increased acuity and census. To encourage additional hours from seasoned nursing staff, increased bonus pay was provided as an incentive for nurses with cancer expertise to work extra shifts during high census and acuity periods.
Assessment of patient hygiene
Preventative measures including proper oral care and daily bathing, specifically chlorhexidine gluconate (CHG) bathing, are recommended to decrease the risk of developing a CLABSI.19–21 We evaluated compliance with oral care and daily bathing from January to May 2014; the median percentage of patient compliance with oral mouth care was 13% and with daily bathing was 16%.
Intervention: 1-2-3 initiative
Based on the evidence of daily CHG bathing19 ,22 and adequate oral hygiene,21 ,23 ,24 we aggressively addressed activity of daily living (ADL) compliance. To improve compliance, the ADL 1-2-3 initiative was adopted: one CHG bath and linen change daily, at least two out-of-bed activities per day and oral care three times per day. Using the process improvement methodology through PDSA testing, a standardised ADL process was developed involving all providers. Interventions included addressing 1-2-3 compliance during multidisciplinary rounds, creating accountability among staff, creation of an algorithm and order set for oral care and daily text message reminders. The physician team took an active role in 1-2-3 compliance, and discussed it daily during rounds. Additionally, the physician team assisted in understanding and mitigating barriers to compliance in non-compliant patients.
Assessment of environmental factors
We evaluated additional environmental variables, including room cleanliness. We identified an increase in dust on infant and toddler climber cribs delivered to the unit as well as frequently cluttered patient rooms. Additionally, compliance with daily linen change was 40% prior to May 2014.
Intervention: environmental factors
Working with environmental services (EVS), we developed a sustainable bed and room cleaning process. Compliance with the revised room cleaning plan was sustained at 100% compliance through biweekly assessments of cleaning compliance, weekly assessments of EVS staffing and collaborative review of EVS barriers to perform daily responsibilities. Additionally, the BMT unit developed a plan to change cribs on a monthly basis due to the extended length of stay for patients. Finally, daily linen change was included in the 1-2-3 initiative and compliance with daily linen change increased from 40% to over 90% from July to August 2014.
Assessment and abandonment of recent practice changes
We evaluated several practices that were introduced after we reached historic CLABSI lows in 2011 and 2012. Each intervention was evaluated closely, and both were abandoned to make line care practices similar to those in 2012.
Line coiling
In July 2013, coiling of the central line under patient dressing was instituted. Discussion with patients and nursing staff revealed concerns of line contamination and poor cleaning of the line prior to placing it proximal to the central line insertion site. Owing to these concerns, the practice of line coiling under the CVC dressing was abandoned in June 2014.
Blood sparing
Blood sparing is a procedure that uses a closed system to return blood waste to patients to potentially decrease the need for blood transfusions. Because of concerns of contamination during the set-up of the blood sparing system, we reverted back to our previous practice—using blood sparing for patients less than 10 kg and for Jehovah Witnesses, in June 2014.
Analytical methods
CLABSIs were measured as the number of CLABSIs per 1000 inpatient CVC days.7 CLABSIs were defined by the National Healthcare Safety Network (NHSN) 2014 criteria.25 Specifically, a CLABSI was defined as a laboratory-confirmed bloodstream infection when a central line is in place for >2 calendar days from the date of the event, the infection was not present on admission and there was no other source of infection documented. All CLABSIs were independently reviewed and classified according to NHSN criteria by the Division of Infection Control.
Wilcoxon Rank Sum Test was used to compare continuous variables between two time periods and statistical process control methods were used to monitor changes in care processes and health outcomes. T charts were used to evaluate the days between events (CLABSIs) and U charts were developed and updated monthly for CLABSI rates. We established a mean, illustrated as the centreline on all control charts with upper and lower control limits. Standard industry criteria were used to determine if observed changes in measures were chance random variation (common cause variation) or due to a specific assignable cause, in this case the intervention (special cause variation).26 ,27 Annotated run charts were updated weekly for 1-2-3 compliance. A median centreline was established, and non-random variation was determined through standard run chart rules.28
Human subjects protection
The present initiative fell within the CCHMC Institutional Review Board's guidance for quality improvement projects that did not constitute human subjects research.
Results
Root cause analysis and FMEA interviews occurred in May 2014, and the majority of the system-wide interventions occurred in early June. The study period of the new interventions was from 1 June 2014 to 31 May 2015. The current CLABSI prevention measures are shown in figure 1.

Current CLABSI prevention measures in the CBDI (May 2015). ALL, acute lymphoblastic leukaemia; AML, acute myeloid leukaemia; ANC, absolute neutrophil counts; CBDI, Cancer and Blood Disease Institute; CHG, chlorhexidine gluconate; CLABSI, central line-associated bloodstream infection.
Compliance with the 1-2-3 initiative
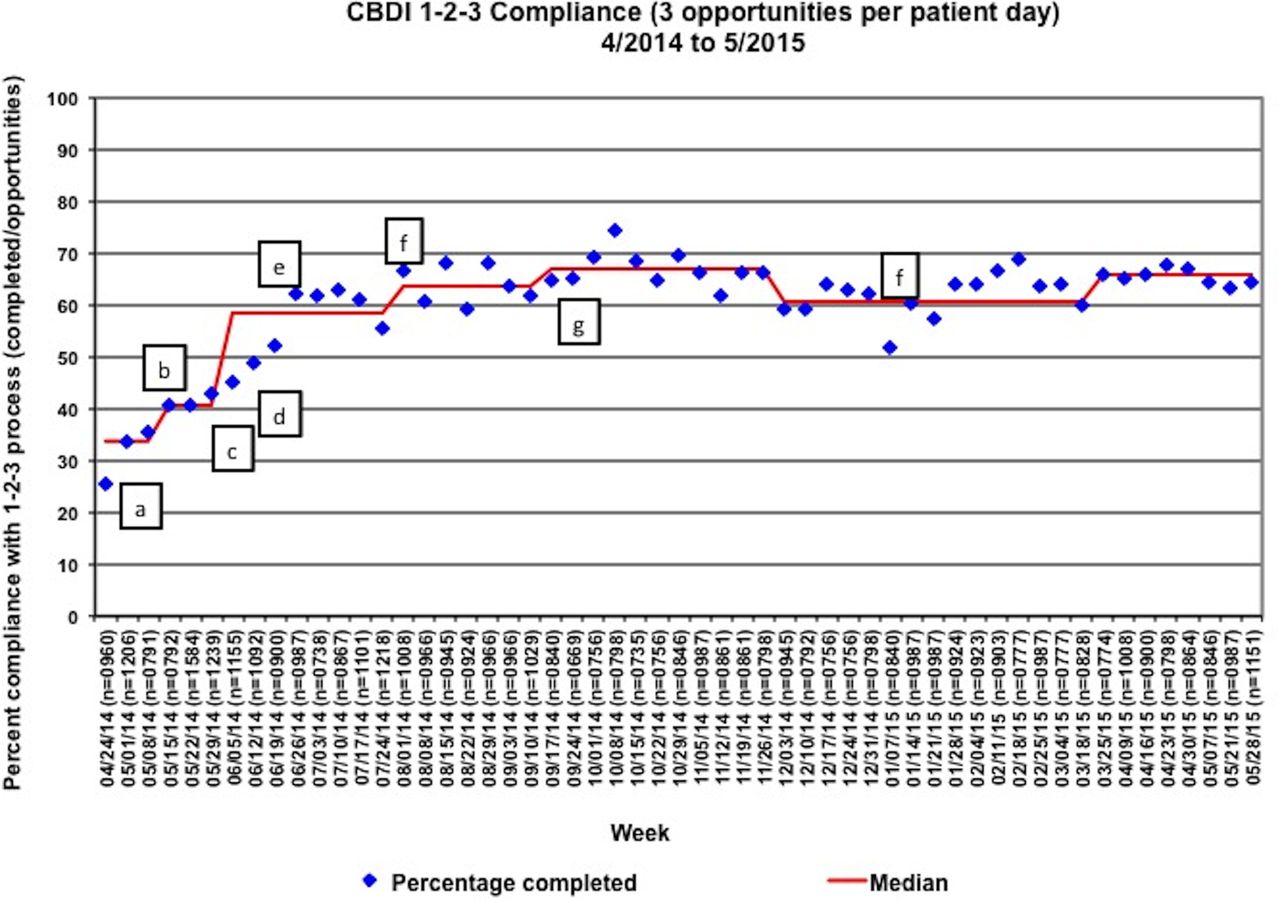
Our baseline compliance with the 1-2-3 initiative was 25%. With our interventions we increased our median compliance to 70% within 3 months, which was sustained through 2015. The greatest impact on compliance was related to text message reminders about completing the 1-2-3 components, designated roles and responsibilities, early engagement with family members and physician discussion with non-compliant patients (figure 2).
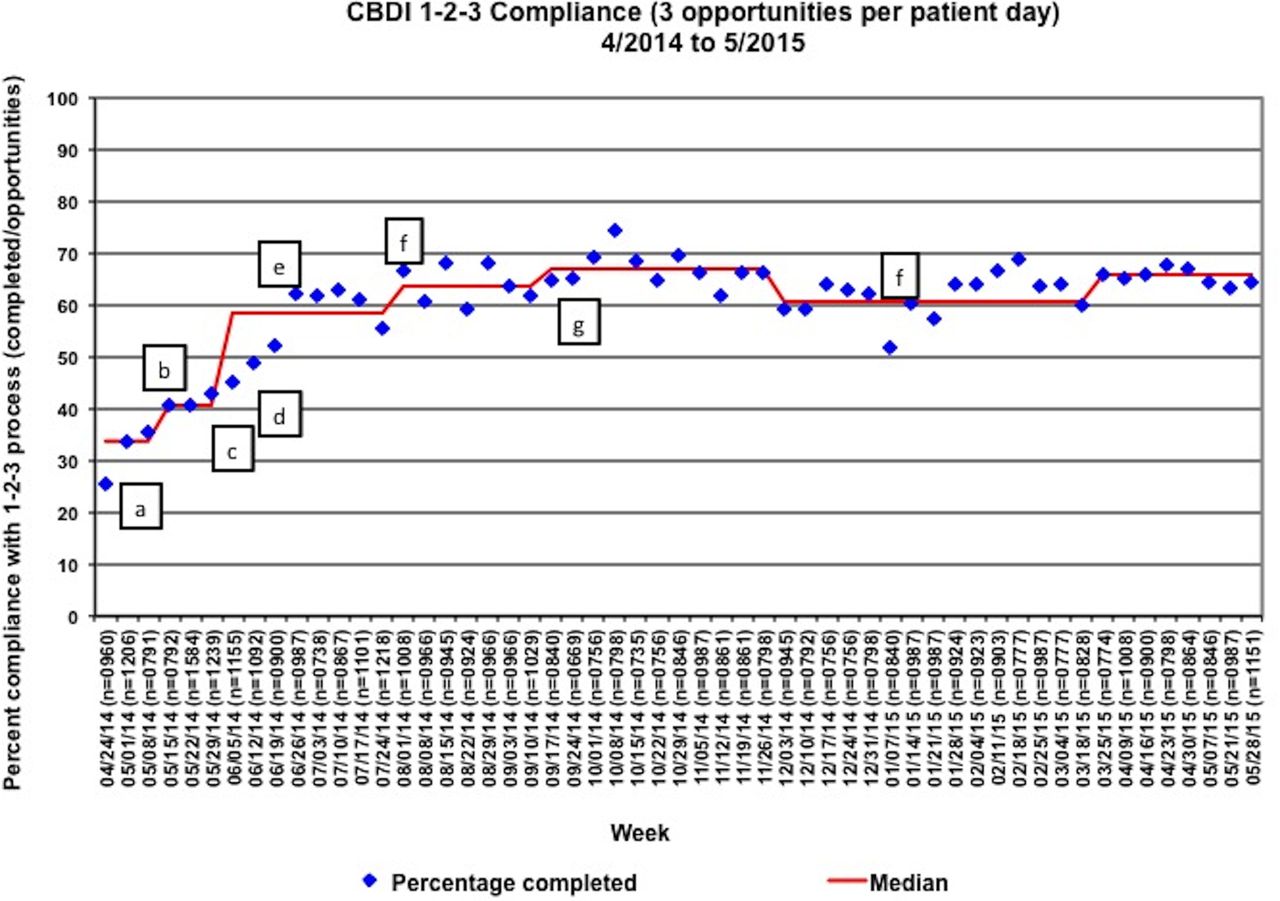
Compliance with the CBDI 1-2-3 compliance process (three opportunities per patient) from April 2014 to May 2015 (standard 1, line run chart). The 1-2-3 process included (1) daily chlorhexidine gluconate (CHG) bathing and linen change, (2) out of bed and active twice daily and (3) three times daily oral care. Each component of the 1-2-3 process was measured in an all-or-none manner. Patients had three opportunities per day and compliance was measured as percentage compliance (number of completed components of 1-2-3/number of opportunities). Timing of interventions: (a) adoption of 1-2-3 process; (b) initial plan-do-study-act (PDSA) testing, with family inclusion, to understand barriers to compliance; (c) staff education on components of 1-2-3; (d) creation of roles and 1-2-3 compliance accountability; (e) twice daily phone reminder PDSA testing followed by implementation; (f) physician team discussion of 1-2-3 on daily rounds, and noncompliance mitigation; (g) spread of patient care attendant CHG bathing role; (h) dental team and pain team engagement in understanding barriers to compliance. CBDI, Cancer and Blood Disease Institute.
Two-person dressing change compliance went from 10% compliance to 100% compliance in the first two weeks of June. This has been sustained and is standard of care in the CBDI. All high-risk procedures are discussed and assistance is advocated at daily sign-out. Rapid changes to the allocation of RNs to meet the increased demand also occurred in June and July.
CLABSI rate
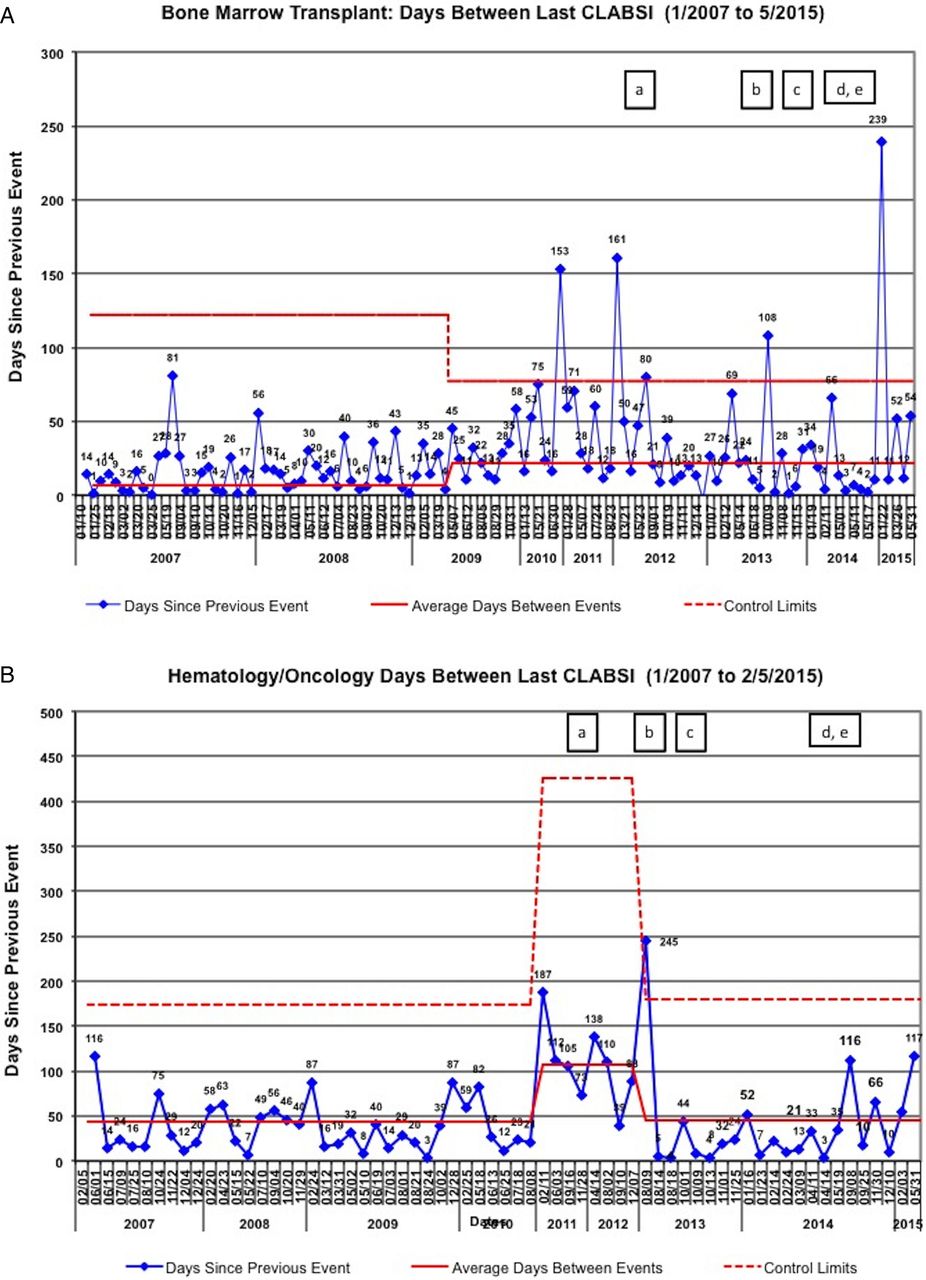
The CLABSI rate from June 2013 to May 2014 was 2.03 CLABSIs/1000 line days. After implementation of our interventions in late May and early June, the CLABSI rate from June 2014 to May 2015 decreased to 0.395 CLABSIs/1000 line days (p=0.008) (figure 3). Six of the eight patients (75%) that had a CLABSI after implementation intervention were identified as high risk prior to infection. After implementation, the BMT and Hem/Onc units sustained prolonged times between CLABSIs of 239 days (figure 4A) and 116 days (figure 4B) respectively.

Central line-associated bloodstream infection (CLABSI) rate in the Cancer and Blood Disease Institute (CBDI) from July 2011 to May 2015 using National Healthcare Safety Network (NHSN) 2014 criteria (U chart). (a) Period of historic low CLABSI rate, 2011–2012; (b) acute increase in census, phase I patients, relapsed refractory patients, national and international referrals; (c) increased percentage of floating and inexperienced nursing; (d) assessment of variables associated with increased CLABSI rate; (e) implementation of identification of high-risk patients, improved daily chlorhexidine gluconate bathing/oral care compliance, increased awareness of high bloodstream infection-risk patients, assistance for nurses performing high bloodstream infection-risk procedures, system to improve allocation of resources.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Days between last central line-associated bloodstream infections (CLABSIs) on the (A) Bone Marrow Transplant unit and (B) Hematology Oncology unit from January 2007 to May 2015 (days-between T chart). The interventions described herein were initiated in June 2014. CLABSIs were determined using National Healthcare Safety Network (NHSN) 2014 criteria. (a) Period of historic low CLABSI rate, 2011–2012; (b) acute increase in census, phase I patients, relapsed refractory patients, national and international referrals; (c) increased percentage of floating and inexperienced nursing; (d) assessment of variables associated with increased CLABSI rate; (e) implementation of identification of high-risk patients, improved daily chlorhexidine gluconate bathing/oral care compliance, increased awareness of high BSI-risk patients, assistance for nurses performing high BSI-risk procedures, system to improve allocation of resources. CLABSI, central line-associated bloodstream infection.
From June 2014 to May 2015, after the interventions were implemented, the number of new relapsed/refractory patients remained stable at a median of eight patients per month; the number of international referrals increased to 4.5 referrals per month; the ADC remained elevated between 60 and 65, although it was slightly down from the peak of 75 in April 2014; active phase I patients in the CBDI remained elevated at a median of 30 per month; and the average daily float nurse hours deceased dramatically from over 200 per day to a median of 50 h per day (see online supplementary figure S5). The decrease in float nurse hours has been accomplished through a slight decrease in the ADC, aggressive hiring of new staff and the incentivised programme for senior nurses to work extra during times of high census and acuity.
Subjective surveys of the RNs after the interventions were largely positive. The RNs felt that their understanding of high-risk procedures improved, and the SC role allowed them assistance with high-risk procedures without feelings of inadequacy.
Discussion
From June 2013 to May 2014, we saw an increased CLABSI rate in the CBDI, possible related to increased microsystem stress. We rapidly identified and mitigated potential underlying drivers to the increased CLABSI rate. After implementation of the interventions, the CLABSI rate decreased nearly 70% from 2.03 CLABSI/1000 line days (June 2013–May 2014) to 0.39 CLABSIs/1000 line days (June 2014–May 2015) despite several continued stressors to our healthcare delivery system. Potentially, these interventions prevented 32 additional CLABSIs; healthcare costs of US$2 000 000; 640 additional hospital days; and 2–4 deaths.4 ,29
Although it is very difficult to measure the impact of any one intervention with improvement, we believe that system stress mitigation was vital in decreasing our CLABSI rates. Hugonnet et al30 found that decreased RN staffing in critically ill patients is associated with increased infection risk and concluded that a substantial amount of all infections could be prevented by maintaining staffing at a higher level. These findings have been reproduced in the surgical, intensive care and paediatric patient populations.31–33 Additionally, the composition of the nursing staff, including a higher float nurse-to-patient ratio, has been shown to increase the risk of CLABSIs.33 Neuraz et al,34 through a multicentre analysis in adult intensive care units, showed poor outcomes to be associated with increased patient-to-physician ratios, high patient turnover and high numbers of procedures performed by staff. Additionally, high workload and provider stress have been shown to negatively impact patient care.35–37 A microlevel approach to understanding the cause of system stress and mitigating the negative impact can improve patient safety.38 The analysis and interventions should be multidisciplinary, involving healthcare professionals who order the insertion and removal of CVCs, those personnel who insert and maintain intravascular catheters, infection control personnel, physician providers and managers. Healthcare leadership should periodically assess knowledge of and adherence to guidelines for all personnel involved in the insertion and maintenance of CVCs. Additionally, microsystem leaders should ensure appropriate nursing staff levels in areas with high-risk procedures and interventions.16
There are several limitations to this work: too few data points between stressors and CLABSIs to associate causation; difficulty in associating any one intervention with the improvement, as we implemented multiple interventions in a short period of time; and inability to evaluate the impact of blood sparing practice abandonment on the overall transfusion rate secondary to the heterogenecity of our patient population. Finally, we are unable to calculate the impact of the decreased average daily float nurse hours and decreased ADC on the CLABSI rate. The decrease in float staff hours on the units was due in large part to our mitigation strategies.
We believe that the findings from our work are transferrable to other institutions experiencing increased system stress from changes in staffing, increased census and/or acuity. We believe that hospitals should provide mechanisms to provide greater staffing assistance and systems responsive to acuity and census fluctuations, to improve safety and quality of patient care.
Acknowledgments
The authors wish to thank the physicians, nurses, patient care assistants, nurse practitioners, hospitalists, fellows and staff at Cincinnati Children's Hospital Medical Center, and especially the patients and their families. The authors thank Dr John Perentesis and Dr Stephen Muething for their guidance and support of this work. They also wish to thank Sheryl Bloomer, Kathi Kramer, Shawn Mock, Shivonne Kimiyalocts, Crystal Doughman, Kelly Mulligan, Angela Bell, Tammy Otis, Connie Koons, Alyssa Rickert and Miranda Flemming. This report employed the SQUIRE publication guidelines for reporting healthcare quality improvement research.39
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online figures
Footnotes
Contributors CED, JH, LF, DH and KD conceptualised and designed the study, drafted the initial manuscript and approved the final manuscript as submitted. DB and EO designed, carried out and tested various components of the CLABSI prevention measures, assisted in the collection of data, reviewed and revised the manuscript and approved the final manuscript as submitted. TB provided statistical support, assisted in the collection of data, reviewed and revised the manuscript and approved the final manuscript as submitted. RN, SJ, JH, MJG, SMD, UK and JS directly supervised this improvement project with critical direction throughout implementation, critically reviewed the manuscript and approved the final manuscript as submitted.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.