Article Text

Abstract
Aim To review studies on hospital doctors' handovers to identify the methods and main findings.
Method A literature search of electronic databases Medline and Embase (via Ovid) was conducted against a set of inclusion criteria.
Results A total of 32 papers were identified. The most common methods of studying handovers were observations and interviews, which typically focused on the sign-out (ie, handover meeting). This is just one stage of the handover process: pre- and posthandover phases were rarely examined. Although providing useful descriptive information, the studies rarely evaluated the quality of handover practices. While communication is generally recognised as the critical component, there has been little training of this skill.
Conclusion The handover literature does not fully identify where communication failures typically occur or influencing conditions, thus hampering the design of effective handover training and tools. A systematic analysis of all the stages of doctors' handovers is required.
- Communication
- handover
- handover process
- hand-off
- patient safety
Statistics from Altmetric.com
Introduction
Handover in healthcare is not just the exchange of patient-specific information but transfers responsibility and accountability for a patient from one care giver to another.1 The information usually comprises the patient's current condition, recent changes, ongoing treatment, and developments or complications.
Handovers are a ‘high-risk’ process that can cause gaps in the continuity of patient care due to communication failures and can contribute to preventable adverse events.2 They represent a safety-critical organisational interface, susceptible to missing, inaccessible or forgotten information.3 The potential for errors to occur at handover is not unique to healthcare. High-profile accidents (eg, Piper Alpha,4 BP Texas City Refinery5) are industrial disasters with poor shift handovers as a causal factor. In healthcare, most handovers do not occur under ideal conditions, and clinicians may fail to allocate enough time to appropriately transfer patient data.6 Consequently, care givers involved may not get a full, accurate picture of a patient's condition,7 and it is only when the patient's outcome is affected that defects in the handover process are exposed.8 A high percentage of handover related incidents are found in malpractice claims,9 and surveys on the quality of handovers highlight the dissatisfaction of healthcare professionals about handover practices.10 11
Research on healthcare handovers is mainly on the nursing shift report.12–15 However, more attention is now being given to the handovers conducted by medical staff, due to working time directives (WTD), which increased shift work and hence more handovers between doctors. The quality of doctors' handovers is now regarded as a key area for improvement in patient safety.1 16–18 This review focuses on doctors' handovers in hospitals; either within a unit (cross-covering or shift changes) or between different disciplines or departments.
Method
The identification of articles relating to doctors' handovers involved searching Medline and Embase databases, via the Ovid system. Search terms, method and inclusion criteria are shown in figure 1.
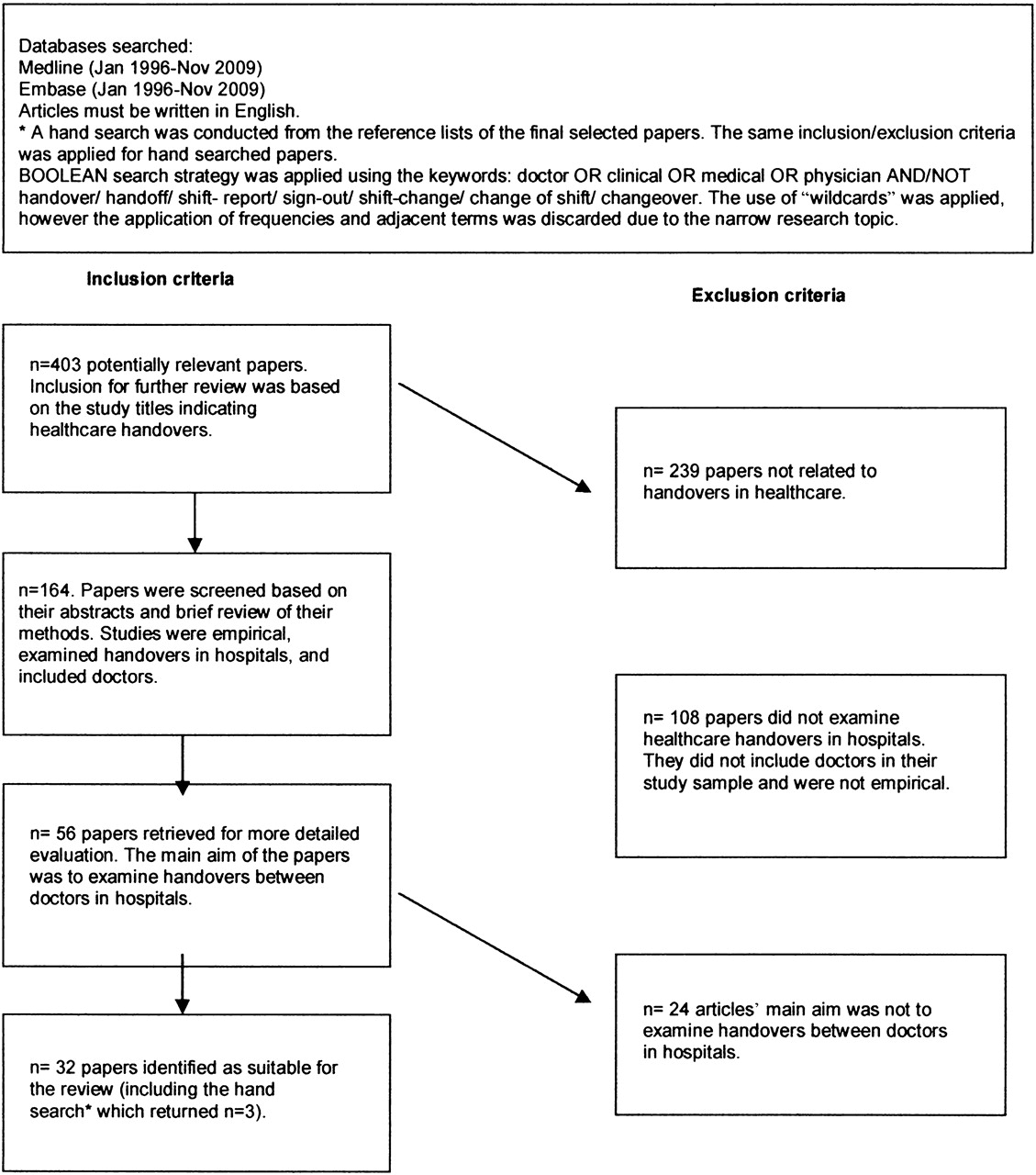
{kind=link}
Literature review search terms and inclusion/exclusion criteria.
Results
We identified 32 empirical studies examining hospital doctors' handovers addressing five main themes:
Doctors' handovers: content and process;
Communication failures during doctors' handovers;
Training and education: research to improve the quality of handovers;
Non-electronic communication tools;
Electronic sign-out systems and other IT solutions.
Two independent coders categorised each article into one or more of the above themes (see online Appendix 1: Table AI); the inter-rater reliability was κ=0.73.
Doctors' handovers: content and process
Research into doctors' handovers has generally focused on content and process by conducting questionnaire surveys, observations and, occasionally, critical incident interviews.3 19 20 Only one study (in US emergency departments)21 identified the stages used for change of shift handovers. Doctors' handovers were observed, and interview and questionnaire data were collected from clinical staff whose work could potentially be affected by these handovers. From the analysis, five stages of handover were proposed: anticipatory, preparatory, handover, immediate posthandover and the posthandover phase.
Junior doctors in two paediatric acute care wards completed a questionnaire assessing quality of the prenight shift handover. Items asked about the adequacy of the information received and where doctors retrieved any missing information. Based on 158 (81%) responses, Borowitz et al22 found that 31% of the residents indicated something had happened while they were on call that the handover had not prepared them for; and that the only variable influencing doctors' perception of preparedness for their night on-call was the quality of the handover. Despite handovers being a frequent activity between doctors, important information is often not transmitted. Bomba and Prakash23 examined doctors' shift changes by questionnaires, interviews and on-site observations. Inadequate handovers were related to medical record keeping (ie, illegible notes, lack of format or structure, errors or incomplete patient information), poor communication and lack of formal, systematic handover processes, especially for after-hours, on-call junior medical staff.
This lack of a formal system has been reported in other observational studies that have shown that there is often no designated handover time or place,24 or there was no formal requirement to attend handover.25 Medical handovers tend to be idiosyncratic.23 25 26 Residents surveyed at three hospitals reported no uniformity in how they signed out after their shift.27 Many signed out verbally ‘wherever and whenever’ they could find the cross-covering doctor. Similarly Laxmisan et al26 noted from observations in an emergency department (ED), that shift handovers were conducted based on incoming and outgoing doctors' preferences. Of 202 internal residency programmes in the USA, 55% did not consistently require both written and oral sign-out during handover,28 a finding that was replicated,29 30 with key clinical information available only two-thirds of the time in written or oral sign-outs of junior doctors. Such findings have led to calls for a more structured approach to doctors' shift handovers, although some argue that this would require a change in administration procedures and organisational culture.23
Content and process have also been examined by studying doctors' perceptions on current handover practices.31–33 Ye et al34 surveyed registrars (n=17) and consultants (n=33) working in three EDs and found that doctors perceived handovers as inaccurate, disorganised, confusing and as having incomplete information. The presenting problem, patient management, investigations undertaken and disposition plans were most commonly reported as the minimum information required from handover.
Communication failures during doctors' handovers
While poor communication has generally been cited as the root cause for inaccurate information transfer in handovers, resulting in almost 60–70% of sentinel events,6 little research has scrutinised types of failures. Arora et al19 interviewed 26 junior doctors who had been on-call one night using the critical incident technique20 to examine whether communication failures during verbal and written handover may have resulted in any patient harm. Communication problems included content omissions, failure to communicate the rationale of a decision, and a tendency not to discuss anticipated problems. A lack of face-to-face communication is a factor in critical medical incidents35 36 with failures to capture errors during information transfer.
Cultural, environmental and human factors affect the effectiveness of information transfer during doctors' handovers.3 37–39 Organisational factors, such as the lack of designated times and locations for handover, often lead to interruptions, which can affect the quality of information transfer. Tokode et al24 surveyed general surgical units in 17 hospitals. Problems in information transfer were often caused by interrupted handovers, a lack of designated time for handover and a mismatch with junior and senior doctors' work hours, such that senior consultants were not always able to attend handover and thus provide feedback to junior doctors.
Communication barriers were revealed in doctors' perceptions of the quality of handover between ED and internal medicine units.3 Semistructured interviews showed that patient handovers between units were seen as a ‘grey zone,’ full of ambiguity and uncertainty. Poor communication practices, such as incomplete and omitted information, caused this problem, because ED doctors and in-patient doctors had conflicting information expectations stemming from their contrasting approaches to patient care. Other failures in information transfer can occur during the sign-out (ie, end of shift) of the outgoing doctor.28–30 Arora et al40 reported that 1876 of 6942 medication chart entries contained discrepancies with the junior doctors' sign-out report. These were mainly information omission (eg, information from medication lists were not included in the sign-out report). In contrast, Wilson et al's41 observational-interview study of a paediatric ward found that the discussions of diagnoses and treatments during handover served as an opportunity to check that important jobs had been completed. Thus, handovers can contribute to an organisation's resilience42 43 because they provide clinicians with an opportunity to capture any errors or threats to patient safety.
Training and education: research to improve the quality of handovers
With the implementation of WTDs, more junior doctors are conducting shift handovers,1 17 18 44 45 but rarely receive formal handover training.45 46 Since many junior doctors feel unprepared, or their handovers are viewed as poor quality,45 it has been suggested that formal training is essential.36 45
Horwitz et al46 developed an oral sign-out curriculum for junior doctors in internal medicine that makes participants aware of: the importance and consequences of poor sign-out, the ideal content (both written and oral), and the SBAR briefing tool (situation, background, assessment, recommendation47). This led to a new verbal sign-out tool: SIGNOUT (sick, identify data, general hospital course, new events, overall health status, upcoming possibilities with plan, tasks to complete, any questions) that has been tested with junior doctors and medical students. Each participant signed out a patient on their list to a ‘receiving’ doctor, then gave feedback on the quality of sign-out (ie, structure, clarity, and omitted or irrelevant information). The training was generally well received, and the mnemonic tool was regarded as useful and comfortable. However, despite feedback after each sign-out, the junior doctors still struggled to remember to provide anticipatory guidance or to read back instructions to the sender.
Similarly, Arora and Johnson48 proposed a model for developing a standardised handover protocol to train junior doctors and registrars. This would enable doctors to become aware of each other's roles and perceptions of the task. A comprehensive understanding of the content of the handover was needed, in order to create a standard checklist. As an alternative to developing support tools, some researchers have assessed how taking part in ward rounds may affect doctors' oral handover skills. Stiles et al49 surveyed junior doctors' and registrars' (n=25) perceptions of the quality of morning report as an educational tool to aid handover. All the doctors surveyed believed that a consultant's presence was critical to education at handover morning report, and 84% believed this report would benefit from senior registrar led discussions. Fassett and Bollipo50 also surveyed junior doctors' perceptions of morning medical handover report and noted similar findings.
Non-electronic communication tools
Handover tools (eg, standardised cards) have mainly been explored using observations and questionnaires. Lee et al51 compared the use of a new sign-out card with other non-standardised methods. Over the course of 92 days, 19 junior doctors participated (10 allocated to the sign-out card intervention group and nine controls). Participants completed a questionnaire about the quality of sign-out they had received after a night of being on-call and left their completed sign-out sheets after each shift for comparison. Those using the sign-out card were less likely to omit patient information such as patient code status (74% completed in the intervention group versus 22% in the control group). Also, poor sign-out was reported by 5.8% of the interns in the intervention group and 14.9% of the control group. Determining the full effects of Lee et al's sign-out tool is hampered because they did not describe the types of non-standardised sign-out methods for the control group.
Bharba et al52 examined effective handover methods using a simulated handover scenario during which five senior house officers performed one-to-one handovers of patients verbally, in writing or with preprepared handover sheets (oral and written). Less patient information was omitted when handover sheets were used compared with when information was only spoken. Although this is one of the few studies using objective measures, it was conducted in a quiet room and so would need to be replicated under more realistic clinical handover conditions.
Tools such as mnemonics have been tested, as they can act as a common language for critical information, thus increasing the likelihood of information retention.47 53 54 Situational briefing techniques (eg, SBAR) have been used to give a standard communication framework for handovers.47 53 They may improve efficiency by aiding anticipation of what information will be required and the level of detail.55 The WHO54 specifically suggests using SBAR as a means of standardising handover practices. Other mnemonics include JUMP,25 where the doctor handing over states the jobs outstanding, the unseen patients, medical contacts and patients to be aware of. The usability of the JUMP mnemonic has yet to be tested, and like other mnemonics for example SBAR, further studies are needed to examine their effectiveness in healthcare.
Electronic sign-out systems and other IT solutions
Efforts to improve handovers have looked to information technology (IT) solutions.35 38 41 56 These have mainly concentrated on the sign-out report. However, computerised tools should be designed to aid communication between doctors, during handover preparation, as well as the handover itself and subsequent activities. These electronic solutions are designed to improve the accuracy of information transfer, but do not take into consideration the behavioural aspects and, therefore, do not always assess all the functions of handover. In an interview study, Sharit et al36 found that some doctors believed that IT solutions for handover were adopted for the sake of employing new technology, without improving communication.
Discussion
This review highlights the pervasive problem of poor information management and communication during, or in preparation for handover which can create a high-risk situation for error.3 A better understanding of types and causes of communication failures would inform risk-management practices. The reviewed studies suggest that well-designed tools to aid preparation of key information and communication at handover are needed. However, caution is required in adopting IT solutions that do not consider the interpersonal functions of handover.
Second, the review revealed a lack of training for doctors (especially juniors) on how to conduct handovers30 45 and an absence of detailed guidelines. This results in a lack of uniformity in procedures, and differing perceptions of ideal handover techniques, as well as distrust of information received and unprofessionalism45 57 within careteams. Nonetheless, some recommendations58 have been made by clinicians on how to provide handover, such as training in the beginning of an internship.29 45 This should provide a forum for junior doctors to discuss their perceptions of handovers and related policies, and offer opportunities for practice and feedback.
While a formal quality assessment59 of the studies was not undertaken due to the developmental nature of this field, most studies would not have achieved a high rating. Current methods used to examine handovers, that is observational, interview or questionnaire, provide a basic understanding of doctors' perceptions of handover practices but do not always assess the quality of handover or evaluate interventions. A recent systematic review on US doctors' handovers60 shows that many studies (including some that have been identified here) do not meet adequate quality assessment criteria.61 Handover research should focus on measurement of risk, adopt more rigorous designs and test interventions.62
Finally, handover encompasses more than just information exchange: it is the transfer of accountability and responsibility, and a teaching opportunity. Moreover, it provides clinicians a chance to interact socially and enables error trapping.63 Handovers should be regarded as components of organisational resilience, and should encompass the activities that are conducted before, during and after the handover in order to examine how technology or other information tools can enhance the process.21 38 41
There is no comprehensive documentation of the activities that doctors engage in prior to, during and after handovers, and the associated artefacts (eg, patient records, whiteboards). We are currently conducting a hierarchical task analysis (HTA) on doctors' handovers in acute medical admissions units.64 This involves decomposing the handover process into subtasks and producing a graphical representation to give a detailed description of the process, and to locate potential risks.
Conclusion
This review found that surprisingly little research has investigated the strengths and weaknesses of doctors' handovers in hospitals. A better understanding of this safety-critical task would help to highlight where failures of communication are likely to occur and enable more effective approaches to standardising handovers.
References
Supplementary materials
Web Only Data
Files in this Data Supplement:
Footnotes
Funding This work is supported by a PhD studentship from the Scottish Funding Council, (Scottish Patient Safety Research Network).
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.