Article Text

Abstract
Objective To understand what patients and family members know about problems and failures in healthcare.
Design Qualitative, semistructured open-ended interviews were conducted with 39 patients and 80 family members about their experiences of incidents in tertiary healthcare. Nineteen interviews involved more than one respondent, yielding 100 interviews in total. Participants were recruited through advertisements in the national broadsheet and tabloid print media (43%), with the help of the health services where the incidents occurred (28%), through invitations sent out by two internet marketing companies (27%) and by consumer organisations (2%).
Setting Interviews were conducted in the homes of the respondents or over the phone. One participant emailed her responses to the questionnaire.
Results Analysis of the interview data revealed: (1) considerable knowledge on the part of patients and relatives about health service risks, problems and incidents; (2) the insight of interviewees into care improvement opportunities; and (3) challenges faced by patients and relatives when trying to negotiate their knowledge and insights with health service staff.
Conclusion Patients (and family members) need access to structured processes ensuring dialogue with health service personnel about perceived risks, problems and incidents. Such dialogue would reveal patients' and family members' questions and knowledge about improvement opportunities, and minimise the risk that their questions and knowledge are ignored.
- Health service incident
- incident management
- practice improvement
- patient involvement
- incident disclosure
- communication
- health policy
- never events
- near miss
- patient safety
- qualitative research
- teamwork
- patient-centred
- patient satisfaction
Statistics from Altmetric.com
- Health service incident
- incident management
- practice improvement
- patient involvement
- incident disclosure
- communication
- health policy
- never events
- near miss
- patient safety
- qualitative research
- teamwork
- patient-centred
- patient satisfaction
Introduction
In recent years, the ‘patients for patient safety’ movement has achieved global recognition for highlighting patients' role in maintaining healthcare safety.1 Health departments and patient safety agencies have since issued policy advice advocating ways for patients to monitor their treatments and assist clinicians in providing safe care.2 Alongside this, academic enquiry has begun to map out the ways in which patients can be and are involved in safety, and evaluate the outcomes of these initiatives.3 4 Overall, the literature recognises three overarching kinds of contributions that patients can make5 6: (1) patients can inform clinicians about how to fine-tune their personal clinical management plans; (2) they can monitor the progress and effects of their treatments; and (3) they can inform services about how to improve clinical practices.5
Whereas the first two of these contributions address the patient's own care, the third intervenes in clinicians' practices at a more general level. Patients may be comfortable with offering suggestions or feedback about their own treatments because that may be considered to be a logical component of their clinical treatment. Advising clinicians and services on how to change or improve their clinical care practice, on the other hand, is a different matter. Three general reasons have been offered to explain patients' apparent reluctance about giving practice improvement feedback.
First, patients are not always prepared to commit their time and energy to general care improvement. Patients have enough to worry about when they are ill, and they may not want to or have the energy to spend time solving the health service's problems. Second, questioning and advising healthcare practitioners about what they do may represent an unacceptable ‘extension of the patient's sick role’.7 ‘Speaking up’ about general safety issues2 may not come naturally, particularly in the case of patients for whom clinicians still represent traditional medical authority. Third, patients may be apprehensive about reporting general care or service problems when clinicians' and services' responses are unappreciative.8 Patients may not inform their care provider about safety problems and risks for fear that clinicians' sensitivity to such feedback may jeopardise their goodwill towards the patient.
To overcome these barriers, innovative approaches have been devised and trialled making it easier for patients to provide generalised feedback. One is ‘experience-based design’,9 now also referred to as ‘co-design’.10 These processes involve patients in one-on-one interviews, focus groups and ‘mirror discussions’ (patients seated in a circle talking about their care experiences with their clinicians attending as members of a silent audience11), yielding recorded accounts and immediate opportunities for staff reflection. These processes may assist in making patients feel it is legitimate to reflect on their general care experiences, relate positive as well as negative events and propose practice changes and improvements.
For patients who are harmed by a serious healthcare incident, providing feedback and receiving a response to their feedback becomes all the more important. The seriousness of the incident also makes confronting service staff or the treating clinician(s) more difficult.8 While many patients regard being ‘a good patient’ no longer as being passive and accepting,12 discussing a hospital-caused and potentially avoidable incident when suffering from a disease compounded by harm is likely to be challenging for most.13 If aspects of the incident become contested, patients may worry about and be burdened by the ‘enormous costs involved in disputes’14 that may arise over the causes and details of the incident.
This last point takes on added significance when put in the context of findings indicating that patients regard incidents as happening with greater frequency, as being of greater severity and as more urgently requiring an explanation and practice improvement attention than their clinicians do.15 Given this gap between patients' and clinicians' perceptions of incidents, it is not surprising that adverse experiences in care have been found to ‘mute or mollify [patients' and relatives'] expressions of dissatisfaction with care’.16 Two questions arise at this point, and it is these that are at the heart of the present article: what kinds of information, questions and suggestions might patients be able to contribute to the practice improvement process, particularly when there is a suspected or acknowledged incident? And what type of process might ensure that matters of concern for patients are relayed to those in charge of practice improvement?
The study: background
Study aim and approach
The overall aim of the study was to map patients' (and, in the case of patients' death, relatives') experiences of healthcare incidents and incident disclosure communication. To this end, 100 semistructured, in-depth interviews17 were conducted between 2009 and 2010 with 119 patients and family members (some interviews were attended by more than one person).
Recruitment
Interview participants were recruited over two phases. The initial phase involved recruitment through participating health services. Health services identified patients who had recently experienced a healthcare incident. Inclusion criteria were that the incident was rated severe to very severe and occurred in or after 2008. The health service forwarded an envelope to the patient's address containing materials developed by the university research team: a study participation request, an information sheet, a consent sheet and a reply-paid envelope. The cover letter invited patients (and/or relatives) to notify the health service of their interest to participate in the study and consent to be contacted by the research team. The health service then forwarded the replies received to the research team who contacted those who responded to the health service mail-out by phone. This approach led to 36 participants being recruited, yielding a total of 28 interviews (some with multiple interviewees).
The second recruitment phase targeted participants via an advertisement in the national print media and a general invitation sent out by internet research companies. This strategy ensured that the study was not fully reliant on health services' views regarding interviewee suitability, offering patients and families themselves the opportunity to opt into the study. The print advertisement campaign yielded 43 interviews with 56 interviewees. The internet research companies' invitation included a brief on-line questionnaire with the aim of identifying potential participants' reasons for opting into the study. In all, 27 people satisfied the recruitment criteria and were interviewed. Consumer organisations were asked to circulate flyers on their websites and at public forums seeking interested individuals in a similar approach to the print media advertisement. This produced two suitable interviewees.
Data collection
All interviewees were contacted prior to the interview to ascertain eligibility for the study, clarify the study aim, obtain consent and agree to the type of interview (face-to-face (and/or video-filmed) or over-the-phone). Fifty per cent of the hundred interviews were conducted face-to-face in the participants' homes. Interview times ranged from 20 min to 3 h. All interviews were audio recorded digitally to facilitate transcription. Interviews were conducted by researchers with extensive healthcare and communication experience to deal with the sensitive and often clinical–technical nature of the subject. While this service was never requested, counselling was routinely offered to participants to manage any additional or postinterview distress caused by participating in the study. One interviewee responded via email to our interview schedule.
Data analysis
The interviews were transcribed verbatim. Because the interviews involved much emotion,18 participants were not asked to read and validate transcripts. Using ‘open coding’,19 analysts (RI, SA and KB) coded transcripts by identifying issues to which interviewees devoted special and extended attention. These issues were classified as themes.20 Themes were imported into and reconciled in QSR NVivo (Qualitative Solutions and Research Pty. Ltd. Version 9), a code-and-retrieve computer software package. Few of the analysts' codings required reconciliation, most functioning to complement or refine agreed codings. Entering the themes in NVivo enabled compilation of the original transcript segments (quotes) belonging to individual coded themes. This procedure also made visible the significance of the theme by revealing the total number of transcript quotes linked to a particular theme (in some cases hundreds), the intensity of the quotes' discourse (eg, ‘angry’, ‘disappointed’) and the number of subthemes linked to a theme (ie, the greater the number of subthemes, the greater the theme's overall significance). The resulting NVivo network of themes enabled identification of three main thematic domains, each with a number of ancillary themes.
Ethics approval
Human research ethics approval was obtained from the universities that were part of the project consortium and from all the health services that participated in the study. The consortium's lead university's approval code is UTS HREC 2008/300. Participants signed and sent back informed consent sheets before their interviews took place.
Results
Study sample characteristics
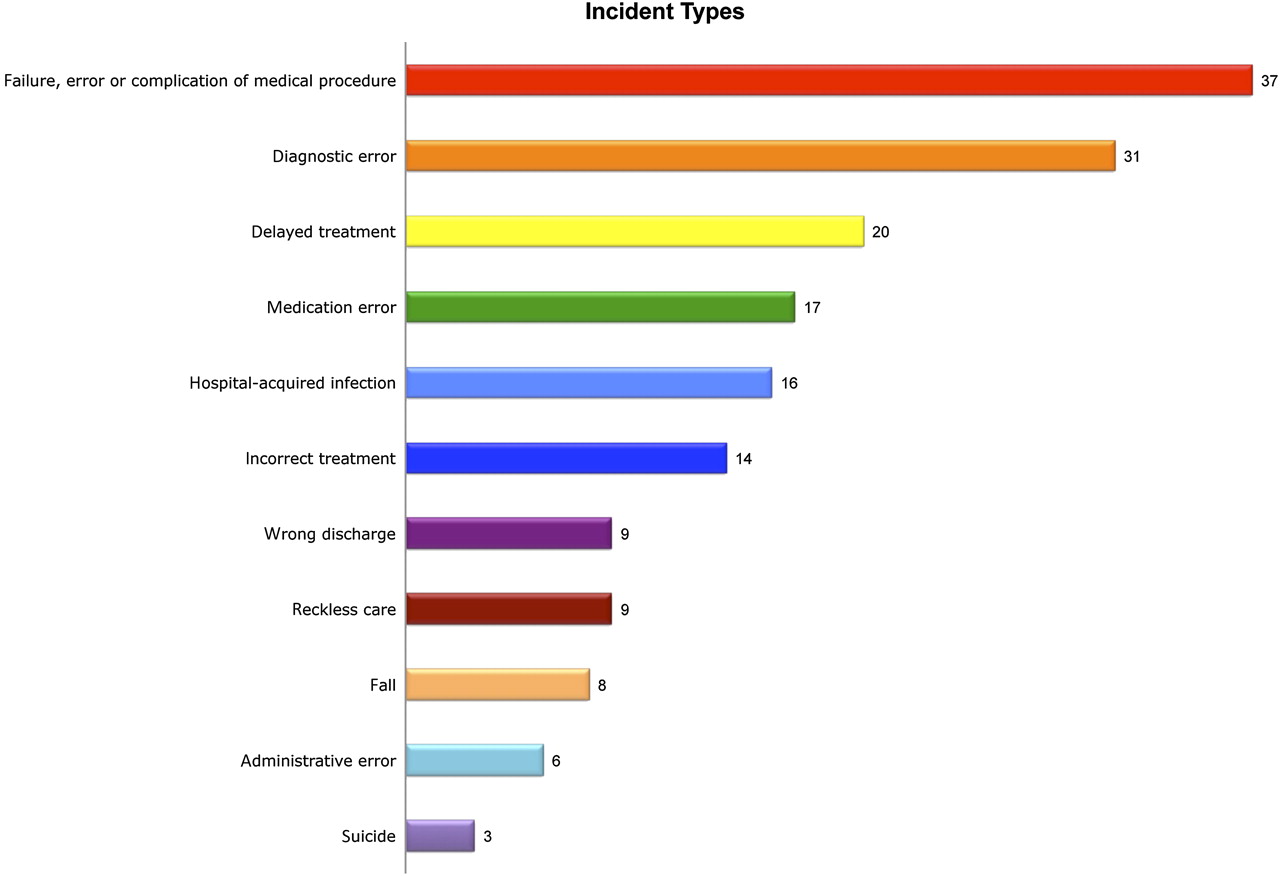
The study involved patients ranging from 4 days to 94 years old with an average age of 57.9 years. Using clinical severity criteria,21 incidents were categorised as very serious (death, permanent or long-term harm) in 77% of cases, serious (short-term serious harm) in 15% of cases and less serious (low level or short-term harm) in the remainder of cases (8%). The incidents discussed in the interviews were mostly failures, errors or complications of medical and surgical procedures (37), diagnostic errors (31), delayed treatment (20), medication errors (17) and hospital-acquired infections (16) (figure 1). The gender profile of patients involved in incidents included in the study (54% males) is close to that of the general patient demographic in Australia (51% males). Most interviewees (46) were from New South Wales; 23 were from Victoria and 23 from Queensland.
{kind=link}
Incidents discussed by patient and family member interviewees. Note: The number of incidents in this diagram (170) exceeds the number of interviews (100), because many of the interviews presented accounts of more than one incident.
Findings
The analysis of the interviews yielded three overarching thematic domains: ‘risks and incidents inherent in care’, ‘ways of minimising those risks’ and ‘negotiating our concerns with clinicians and/or the service’. With regard to the first domain, interviewees' knowledge of service risks manifested in four ways. First, interviewees spoke in some detail about what they realised may have been unpreventable incidents. They showed awareness of the complexity of providing clinical care and how this complexity could cause problems and adverse outcomes for which no one could and should be held responsible. Second, interviewees revealed awareness of substandard clinical care and the incidents that this could entrain. This pertained to clinicians forgetting to do critical things or (in the eyes of the interviewees) regarding critical things as unimportant or unnecessary. Third, patients and family members commented on repeated problems resulting from disorganised care posing unresolved risks. They saw these risks as endangering care and as requiring urgent attention to ensure better care design and service planning. Finally, they spoke about problems and incidents which they regarded as having been caused by unreasonable (sometimes referred to as ‘reckless’) care (table 1).
Perceiving safety risks inherent in care
Besides commenting on the nature and unfolding of service risks and incidents, interviewees also discussed how clinicians might resolve and prevent them. Under this second overarching thematic domain, interviewees revealed ways of ensuring their own safety, improving the organisation of care, strengthening incident investigation processes and bolstering incident disclosure (table 2). The findings indicate that patients and relatives can be articulate about how practitioners may limit patient safety risks and that they can provide useful input into how the service deals with specific risks and problems.
Proposing ways of strengthening safety
The third and final thematic domain relates to how patients and family members negotiated these ideas and experiences with their clinicians and health service representatives. Overwhelmingly, patients and family interviewees felt that they failed to be heeded. Their concern was that this lack of impact on the practices and thinking of practitioners could have had or did indeed have disastrous consequences. Some felt that their input was ignored, while others felt it was belittled. Interviewees commented that questioning clinicians about their actions, choices and decisions was an ongoing challenge. As the quotes in table 3 show, several interviewees reported that their attempt to challenge or change care practices led to conflict. Conflict, in turn, led patients and family members to doubt the clinicians' ethical stance, to withdraw from what was deemed to be unsafe care and at times to mobilise institutions external to health (such as the Ombudsman, the media or lawyers) to force the health service to share information or acknowledge shortcomings (table 3).
Communicating safety concerns to clinicians
Discussion
The findings outlined above reveal that patients and family members had many questions about and insights into service shortcomings. Admittedly, some of these questions and insights were initiated or fuelled by comments made by clinicians not immediately involved in the care. Nevertheless, interviewees offered ideas about how to improve their own safety, how to better organise the care provided, how to conduct incident investigations and how to practise better incident disclosure. As the analysis and quotes presented in tables 1 and 2 reveal, interviewees distinguished unpreventable incidents from incidents following on from organisational risks that remained unresolved, incidents resulting from substandard instances of care provided by individuals or teams, and incidents resulting from unreasonable or reckless care. This incident typology crystallised interviewees' responses to what was for them the most critical question to be addressed following an incident: would they, their clinicians or anyone else have been able to prevent or avert the incident had they acted or known how to act differently?
Taken together, these findings offer ground for optimism about the benefits of involving patients in addressing failures and errors. Their questions and understandings about incidents can play an important role in navigating through the aftermath of incidents and in targeting practice improvement. On the other hand, evidence of patients' troubled attempts to negotiate their concerns and ideas with their health service again dampens our optimism. When serious incidents happen, and patients' feedback and advice may pertain to clinical practice improvement on a broad scale, the principle that ‘patients' potential contributions to their safety can be regarded as compatible with, rather than indicative of a lack of, trust’ (p 409)22 may not apply. These latter findings indicate that patients' and relatives' concerns about the broader aspects of care and safety need carefully structured elicitation. This is particularly the case when these concerns are at risk of being muted by the need experienced by patients and relatives to contain difficult memories, or by their fear of losing their clinicians' sympathy and support.
Overall, interviewees felt that more interactive approaches to care planning, problem minimisation and—most importantly—incident disclosure would enable them to articulate questions and insights such as the ones described above. Framed as a dialogue and anchored to the principle of ‘being open’,23 incident disclosure may create room for patients' and relatives' questions about and insight into the risks, problems, failures and errors accompanying and explaining the unexpected outcome. Such dialogue needs to be carefully choreographed to ensure both patients and clinicians can share their questions and experiences, and learn from adversity. As open dialogue, incident disclosure may benefit patient involvement in treatment decision-making, as well as patient input into clinical practice improvement.24 To allow patients (and relatives) to help clinicians obviate service safety risks for future patients, significant governmental, professional and public support is needed to ensure being open about incidents with those who are harmed becomes part and parcel of how healthcare services tackle incident management.25
Finally, the study had three limitations. First, few people came forward to be interviewed despite thousands of patients being estimated to experience serious incidents every year.26 27 Despite aiming for considerably more interviews, the study was concluded when it reached 100 interviews due to time and funding constraints. Saturation on the overarching themes outlined above was evident, but the richness of the existing interviews suggested that additional data might have affected the number and specification of ancillary themes. Second, the study's interviewee recruitment process was complicated and limited by the health services' ethics committees' requirement that the health service be granted the right to independently select the patients and incidents to include in the study. Third, these interviews are in essence patients and family members self-reporting what went wrong and how it was disclosed. We were not able to check these accounts against those offered by the practitioners involved (doing so was designed into the study, but vetoed by all participating health services).
Conclusion
This article has presented evidence derived from the largest interview study conducted to date investigating 119 patients' and family members' insights into and questions about risks, incidents and incident disclosure. The article further outlined barriers to patients and family members being heard, in addition to practical and ethical reasons for taking into account what patients and family members have to offer as part of the incident management process.
As central component of this process, incident disclosure presents a range of opportunities. Healthcare organisations and managers may mobilise disclosure as a way to role-modelling ethical and professional ways of dealing with patients and families, even in adverse circumstances. Services may also use disclosure as the means of involving patients in strengthening clinical safety at levels that go beyond their personal care and that extend to rendering the service safer (eg, through ‘co-design’). Practitioners may, through being open about incidents, recognise the importance of the untutored questions and experience-based views that patients and families have about what led to the incident. These questions and views may be able to shed light on what made the incident inevitable, avoidable or perhaps even unacceptable. Finally, disclosure presents an opportunity for patients and families to ensure others do not fall victim to the same type of incident, and this concern should invest incident investigation and professional learning with special motivation and gravity.28
At these various levels, openness may ensure that safety and quality prevail over fear, recrimination and bureaucratisation. Openness may countervail behaviours whose “entanglement and enmeshing of day-to-day life into legal liability with the risk of potential litigation will lead to overcautious, excessively sensitive, cramped and inhibited social relationships” (p 105).29
In advocating open dialogue with patients and family members, we neither downplay the constraints that are attached to privileged information nor diminish the risks of engaging in disclosure. However, our study suggests that ‘being open’ is what patients and families prefer and expect. In this regard, the expression ‘being open’ is better attuned than the awkward term ‘disclosure’ to characterise the desired quality of postincident communication between clinicians and those harmed. Indeed, being open characterises all of the most critical tasks emerging from this study. Clinicians need to make patients and their relatives aware that their concerns about harm and safety risks are listened to and acted on. Services need to be open to patients or families wanting to discuss improvements, and perhaps partake in activities where such improvements are monitored and evaluated. Openness in care should guide these tasks, as it is what patients and relatives regard as ethical and professional.
Acknowledgments
We thank all the patients and family members who contributed to this study. We also thank all the people at the health services and ethics committees who saw merit in this work and allowed us access to patients who were harmed by a healthcare incident. We further thank the Australia-wide investigator team whose assistance with data collection and data interpretation have been invaluable.
References
Footnotes
Funding This work was supported by the Australian Commission on Safety and Quality in Health Care, and we thank them for their financial and practical support and moral encouragement during the two and a half years of the project.
Competing interests None.
Ethics approval UTS HREC, approval code: 2008/300.
Provenance and peer review Not commissioned; externally peer reviewed.