Article Text

Abstract
The management literature reveals that many successful organisations have strategic plans that include a bold ‘stretch-goal’ to stimulate progress over a ten-to-thirty-year period. A stretch goal is clear, compelling and easily understood. It serves as a unifying focal point for organisational efforts. The ambitiousness of such goals has been emphasised with the phrase Big Hairy Audacious Goal (‘BHAG’). President Kennedy's proclamation in 1961 that ‘this Nation should commit itself to achieving the goal, before this decade is out, of landing a man on the moon and returning him safely to earth’ provides a famous example. This goal energised the US National Aeronautics and Space Administration, and it captured the attention of the American public and resulted in one of the largest accomplishments of any organisation. The goal set by Sony, a small, cash-strapped electronics company in the 1950s, to change the poor image of Japanese products around the world represents a classic BHAG. Few examples of quality goals that conform to the BHAG definition exist in the healthcare literature. However, the concept may provide a useful framework for organisations seeking to transform the quality of care they deliver. This review examines the merits and cautions of setting overarching quality goals to catalyse quality improvement efforts, and assists healthcare organisations with determining whether to adopt these goals.
- Leadership
- Healthcare quality improvement
- Quality improvement methodologies
- Management
- Patient safety
Statistics from Altmetric.com
Introduction
In the last decade, a series of Institute of Medicine reports,1 ,2 major studies on quality of care by respected analysts,3 and a greater appreciation of data on practise variations4–10 have led to the widely-accepted conclusion that the quality of healthcare falls short of expectations. This conclusion comes at a time of unprecedented growth in diagnostic and therapeutic options that have transformed previously fatal conditions into chronic health conditions or outright cures. There is also important underappreciated evidence that improved routine care, such as the treatment of cardiovascular disease, cancer and arthritis, has resulted in declining mortality rates.11
There are many reasons for the dichotomy between major advancements in diagnostics and therapeutics, and the perception of suboptimal quality of care, including changing expectations, specialisation leading to loss of the human touch, and factors outside the purview of our delivery system such as patients’ lifestyles. Alternatively, it may be that healthcare professionals are failing to capture important aspects of quality in extant measures.
Rather than continuing to challenge current conclusions about quality, we may be better off trying to mobilise healthcare organisations around quality improvement. Many industries such as retail, aerospace and pharmaceuticals have used long-term overarching quality goals to galvanise organisational efforts around improving quality. These goals have received little attention in the healthcare industry. The aims of this report are to present the merits and cautions of overarching quality goals to achieve quality improvement, and to address the question of whether healthcare organisations should adopt these goals.
Methodology
We conducted a comprehensive literature review using multiple search strategies. We searched the PubMed database for medical literature and the Abstracted Business Information (ABI) Inform database for management literature, using the search terms ‘goal setting’, ‘overarching goal’ and ‘quality improvement’. We identified additional literature through references from the initial data set and suggestions from subject matter experts. Articles were included if they described or evaluated overarching goals as a tool for quality improvement.
Overarching goals in other industries
Management literature reveals that many organisations that enjoy enduring success have a core ideology that remains fixed while their strategies and practises continuously adapt to a changing environment.12–15 A well conceived organisational vision consists of two major components: a core ideology, which defines the enduring organisational character and transcends technological breakthroughs, management fads and individual leaders; and an envisioned future, which serves as an impetus for change.12
An envisioned future consists of two parts: a ten-to-thirty-year Big Hairy Audacious Goal (‘BHAG’, or overarching goal) and a vivid description of what the organisation will be like when it achieves this goal. The phrase BHAG was coined by Collins and Porras in 199413 and much of the following description of overarching goals in non-healthcare industries is based on their work.
An overarching goal is a bold ‘stretch-goal’ that stimulates progress. It is highly focused, clear, compelling and easily understandable, serves as a unifying focal point of effort, and acts as a catalyst for team spirit. It has a clear finish line, so the organisation knows when it has achieved the goal. One of the most famous overarching goals was President Kennedy's proclamation in 1961 that ‘this Nation should commit itself to achieving the goal, before this decade is out, of landing a man on the moon and returning him safely to earth’.16 This goal was a call to the nation rather than a goal set by a specific organisation, so it energised the National Aeronautics and Space Administration (NASA), and also captured the attention of the American public and resulted in one of the most impressive accomplishments by any organisation.14
As the goal becomes the focal point and takes on a life of its own, the leader becomes less important. After President Kennedy's death in 1963, the moon mission did not become less inspiring. The goal itself became the motivating mechanism and its ability to stimulate progress remained.
To be transformative, Collins suggests that an overarching goal should not be a sure bet—it should have no more than 50–70% probability of success, but the organisation must believe that it can reach the goal with extraordinary effort.12 ,13 For example, Sony, a small, cash-strapped venture in the 1950s, set a goal to change the poor quality image of Japanese products around the world. Similarly, in the 1930s, Merck set an overarching quality goal to transform itself from a chemical manufacturer into one of the pre-eminent global pharmaceutical companies.13
Often, overarching quality goals seem even more audacious to people outside of the organisation. However, organisations display a remarkable ability to achieve even their most audacious goals: NASA did send astronauts to the moon, Sony did change the poor quality image of Japanese products, and Merck did transform itself into a pre-eminent global pharmaceutical company. However, due to the high inherent probability of failure, many organisations fail to achieve their BHAGs. For example, the United Nations set the Millennium Development Goal to achieve universal completion of primary education for all children in its member states by 2015.17 Although this goal has not yet been achieved, many smaller but important successes have been achieve along the way—countries such as Burundi, the Democratic Republic of the Congo, Ethiopia, Ghana, Kenya, Malawi, Mozambique, Tanzania and Uganda have abolished school fees, which has led to a surge in enrolment.17 In cases like this, even though an organisation may not be successful in reaching a BHAG, the successes achieved along the way can make its efforts worthwhile. In formulating BHAGs, it is important for organisations to consider whether improvements would be realised even if the BHAG is not achieved.
Although an organisation can have any number of goals, visionary organisations pursue only those that reinforce their core ideology. For example, it may not be consistent with a hospital's core ideology to change its case mix in order to improve quality and safety. Furthermore, while some organisations choose common enemy goals to defeat a specific competitor, such as Nike's goal in the 1960s to ‘Crush Adidas’, others choose target goals that are independent of competitors. Some level of competition may lead to improved quality across an industry, and many European countries have introduced an element of competition into healthcare in an attempt to realise this improved quality.18 ,19 However, it is critically important to consider whether organisational culture and management practises would allow the organisation to thrive in a competitive environment.19 In situations where competition may detract from the ultimate goal of improved patient safety, an alternative target goal would be for healthcare organisations to ultimately compete with illness, not with each other.
The importance of a vivid description
A vivid description of the overarching quality goal is a vibrant, engaging and specific description of what it will be like to achieve the goal. This description is essential for making the ten-to-thirty-year goal tangible, and it must convey passion, emotion and conviction.12 Some executives make more progress by starting with the vivid description and subsequently defining the overarching quality goal. At the opening of Merck's first research facility in 1933, George Merck presented the vivid description, ‘We believe that research … will bring to industry and commerce new life; …Science will be advanced, knowledge increased, and human life win ever a greater freedom from suffering and disease.’12
Overarching quality goals in healthcare
Collins and Porras do not explicitly discuss the application of overarching goals to healthcare.12 ,13 In fact, the literature on goal-setting in healthcare is sparse and divided among goals that do not conform to the traditional BHAG definition, failed BHAGs and BHAGs that are in progress. Overarching quality goals in healthcare often do not conform to the traditional BHAG definition for several reasons. First, healthcare organisations are much less likely to be at risk of going out of business than companies in other industries, due to unique funding models as well as a consistent, high demand for healthcare services. However, BHAGs may be helpful in galvanising efforts around quality improvement in an industry where there may be less extrinsic pressures for quality improvement among front-line employees. Second, performance and quality in healthcare may be more difficult to quantify and measure than in other industries as it involves measuring the health of a population in addition to more easily defined metrics such as sales and profits.
Third, most large hospital improvement efforts have a short time horizon, on the order of 2–5 years. For example, in 2002, Ascension Health, the largest not-for-profit health system in the US, had the goal to provide ‘healthcare that is safe,’ defined as excellent clinical care with no preventable injuries or deaths by July 2008.20 Also, Cincinnati Children's Hospital set aims to reduce serious safety events by 25% from baseline in 2007, and to reach an overall reduction in serious safety events of 80% from baseline in 2008.21 Finally, in 2008, the European Commission declared a broad cross-institution goal of electronic health record interoperability across European Union borders by 2015.22 Although these goals do not meet the definition of a BHAG due to their short time horizons, they are focused, clear and compelling, and definitely not a sure bet.
Fourth, quality goals in healthcare are often set such that there is a considerable degree of certainty that the desired outcome will be achieved. For example, in 2007, Sentara Health Care in Norfolk Virginia (VA) set the strategic aim to eliminate preventable harm, defined as a 20% reduction in serious safety events by 2010, building on a previous 65% reduction from 2003 to 2007. As they had previously successfully reduced safety events, an additional 20% reduction had a high level of certainty.21
Finally, some quality goals in healthcare do not conform to the BHAG definition because they do not have clear finish lines. For example, in December 2004, the Institute for Healthcare Improvement (IHI) set the goal to ‘reduce morbidity and mortality in America … [by] extending or saving as many as 100 000 lives … in 18 months… and in every year thereafter’ through deploying rapid response teams; delivering reliable, evidence-based care for acute myocardial infarction; preventing adverse drug events; preventing central line infections; preventing surgical site infections; and preventing ventilator-associated pneumonia.23 While many successes have been seen in each of these areas, we do not know whether the IHI has been successful in reaching this goal as it is extremely difficult to determine the number of lives saved by the associated interventions across the country.24 Although the criteria for success were difficult to measure for this initiative, it did unify many organisations across the USA around a common goal and lasting reductions have been made to preventable patient harm through these efforts.25 ,26
While many quality goals in healthcare do not conform to the traditional BHAG definition, BHAGS do exist in the healthcare literature. In cases where these BHAGs have failed, the improvements gained have often made the journeys well worth the effort. For example, in 1971, President Nixon set a BHAG by declaring a war on cancer. He proclaimed, ‘The time has come in America when the same kind of concentrated effort that split the atom and took man to the moon should be turned toward conquering [cancer].’ Like President Kennedy's moon mission, the war on cancer was a call to the nation, not to a specific organisation with close control over execution of its goals. It rallied multiple organisations around a common goal. In 2003, the Director of the National Cancer Institute added a timeline to the war on cancer by issuing the challenge ‘to eliminate the suffering and death from cancer… by 2015’. Although cancer has not been eradicated more than 30 years after President Nixon's original goal, the number of non-skin cancer survivors has increased from three million in 1971 to 11.7 million in 2007.27
We have yet to determine whether some BHAGs in healthcare will be successful as they are still in progress. For example, an emerging effort at Dartmouth Institute for Health Policy and Clinical Practise has a stated goal of ‘achieving the healthiest population possible in our two states (New Hampshire and Vermont)’.28 This is reflected in the mission statement of Dartmouth-Hitchcock Medical Center, to ‘achieve the healthiest population possible, leading the transformation of healthcare in our region and setting the standard for our nation.’ Like the moon mission, this goal is a call to a region rather than a specific organisation, and fosters cooperation and collaboration around a common goal rather than competition. The effort is just beginning and specific targets and timelines are being formulated.
Finally, many important quality improvement initiatives have been successful in healthcare without the use of overarching quality goals. For example, the US Veterans Health Administration transformed its image from a ‘dangerous, dirty and scandal-ridden’ healthcare organisation in the early 1990s to one of the highest quality, most cost-effective systems in the USA today.29 ,30 Without a specific BHAG, they made a transition from a culture of quality assurance to one of quality improvement, employing various initiatives such as a national surgical quality improvement programme, a national customer feedback centre, and training and financial support for individual VA facilities to adopt quality improvement initiatives.31
How do you meet the goal?
Although many organisations set big goals, research shows that only 38% of them reported being ‘completely’ or ‘mostly’ successful.15 Barriers to the successful implementation of overarching quality goals have been documented in the literature,32–34 including goals that are not clearly defined, a lack of resources to support improvement initiatives and a failure of management to provide ongoing support.
Organisational transformation is required to achieve BHAGs. Successful organisational transformations that have overcome the barriers described above have three key elements in common:35
-
Narrative review op-down direction setting
Top-down direction setting should be used to develop overarching quality goals. A goal must be articulated and a sense of urgency must also be communicated to ensure the cooperation and motivation of many individuals.20 ,36 After two very public chemotherapy overdoses in 1995, the Dana-Farber Cancer Institute successfully transformed its organisation into one with an overarching goal of quality and safety by engaging leadership to communicate a sense of urgency, be held accountable and set performance expectations. Although a formal BHAG was not used in this initiative, Dana-Farber cited the engagement of leadership as its most critical success factor.37
Another key success factor is the formation of a powerful guiding coalition with enough power to lead the change effort.36 This group need not include all of the company's most senior executives, but it should be powerful nonetheless—in terms of titles, information and expertise, reputations and relationships. Because the guiding coalition includes members who are not part of senior management, it should operate outside of the normal organisational hierarchy in order to develop a shared assessment of the organisation's problems and opportunities.
-
Bottom-up performance improvement
Broad-based, bottom-up performance improvement can be used to encourage people to take a fresh approach to solving problems. This requires clear communication using a range of media. A good transformation story disseminated widely can bridge the gap between top management and the rest of the organisation. The transformation story should address the case for change, the challenges and opportunities ahead, and the impact that the change will achieve. Good stories also confront the emotional angle and the need to embrace a different mentality at work. Leaders at Dana-Farber were able to communicate a transformation story about the iatrogenic death of Betsy Lehman. They focused on the expectation of a preoccupation with the possibility of error, constant vigilance to safe practise, avoiding the ‘arrogance of excellence’, and transparency and honesty when confronted with errors and harm.37
On-going communication should include symbolic anecdotes and success stories. For example, a hospital that set the goal of ‘uniting its staff around the needs of patients’ highlighted the way an obstetric team had combined management data and doctors’ experiences to identify the cause of high mortality rates among part of an immigrant population that the hospital served. Illustrations such as this serve as examples of collaborative behaviours and analytical approaches to problems that the hospital expected from everyone else. Other successful motivators include contests, such as a contest for the best idea to improve patient safety.
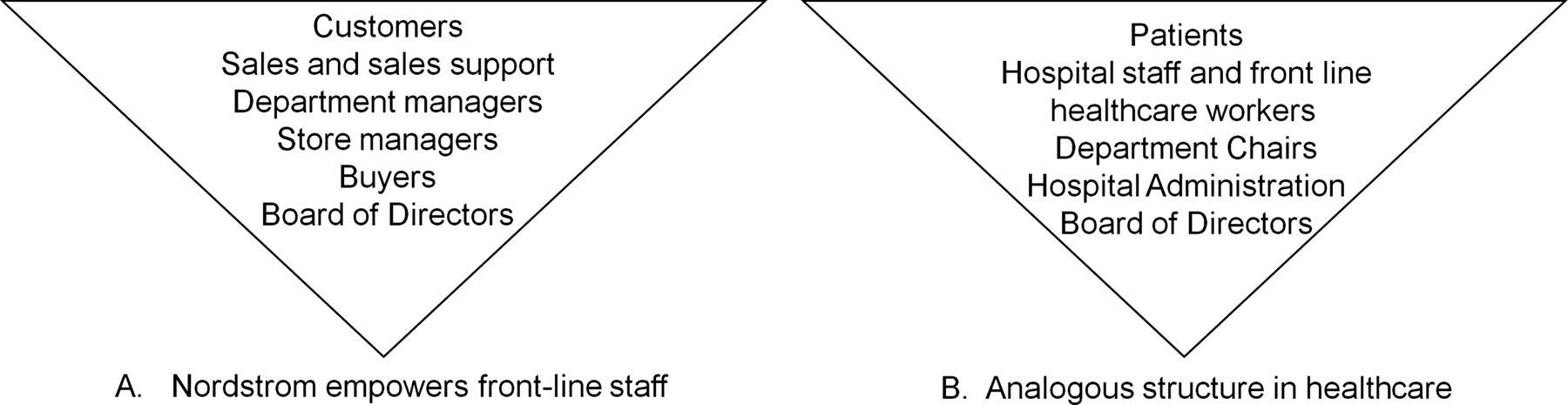
To effectively achieve bottom-up performance improvement, the importance of front-line healthcare workers and other hospital staff must be emphasised and communicated. For example, the retailer Nordstrom described its company structure as an upside down pyramid, empowering and emphasising the importance of front-line sales staff.13 Figure 1 shows an analogous organisational structure that can be applied to hospitals, empowering front-line staff.

{kind=link}
Nordstrom uses a bottom-up organisation that empowers front-line staff (A). An analogous organisational structure in healthcare is shown in (B).
To illustrate the importance of front-line staff, Dana-Farber described patients and their families as victims, and also clinical staff who experience shame and blame due to medical errors.37 This nurtured a supportive working environment, where front-line staff were comfortable reporting errors and near-misses, and clear and objective decision rules were used to determine accountability subsequent to an adverse event.37
-
Cross-functional core process redesign
Cross-functional core process redesign links people, activities and information in new ways, producing dramatic improvements in cost, quality and timeliness. Our healthcare centre used a cross-functional approach when it created teams to develop its care paths for coronary artery bypass graft surgery in the mid-1990s. These teams included cardiologists, cardiac surgeons, anaesthesiologists, residents, operating room personnel, physical therapists, dieticians, social workers and other non-medical staff.
Although many organisations have cross-functional initiatives, cross-functional core process redesign takes them much further with its intense performance orientation, its focus on only a few key processes and its support for the resulting changes.35 This approach shifts the focus of work and decision-making from hierarchical channels to new horizontal flows across functions, locations and organisational boundaries, and can achieve dramatic improvements (25–75% or more) in cost, quality and time.35
Pitfalls in adopting overarching goals
Although overarching goals have been successful in other industries, critics cite some serious pitfalls32–34 that should be considered when implementing such goals in healthcare. First, given the a priori probability of success of no more than 50–70%, many efforts are bound to fail. In those cases, the key is whether the damage and disappointment of ‘failure’ is justified by the lessons of the journey. If the organisation is confident that the attempt and process will always be justified regardless of the outcome, than this risk is minimised. For example, there have been many successes in the war on cancer, even though we have not met President Nixon's goal of eradicating the disease. But if failure to achieve the goal is likely to lead to an abandonment of the infrastructure and improvements that were created to reach it, then the damage can be lasting. In the end, a key question is whether the leadership will be glad they made the effort even if they fail.
Second, a goal that is too specific can cause employees to neglect important dimensions of performance that are not specified by the goal-setting system.32 The trade-offs between urgent, imminent daily challenges and the importance of making progress on the overarching goal cannot be avoided. Third, specific and challenging goals may motivate unethical behaviour and distort risk preferences by promoting the adoption of riskier strategies to attain the goals.32 ,34 Examples of unethical behaviour resulting from goals include failure to report errors or problems with achieving the goal. When the stakes are high, such as in healthcare where errors may result in increased morbidity and mortality, this is high-risk behaviour. This problem may be particularly prevalent when the time horizon is relatively short. In the last few years, the financial services sector has provided a plethora of examples where focus on quarterly profits and meeting earning targets came at the expense of organisational health.
Fourth, aggressive goal-setting may promote a culture of competition rather than cooperation.32 In healthcare it is widely accepted that improved efficiency and outcomes require enhanced teamwork within and between organisations. Setting adversarial overarching goals such as ‘to have dominant market share’ rather than focusing on internal transformation or target goals such as ‘relieving suffering’ may detract from that teamwork and ultimately make the overarching goal unachievable. Finally, there is the concern that while increasing extrinsic motivation, overarching goals can cause a reduction in intrinsic motivation.32 Healthcare providers who are otherwise motivated to do their best for individual patients may make different choices if they are being motivated by an inappropriate overarching goal. If the goal is to capture market share and retain care within an organisation but the individual patient would likely fare better with a referral to a cross-town rival, front-line providers could be torn among loyalties.
Should healthcare organisations adopt overarching quality and safety goals?
Based on the experience of other industries with overarching quality goals, and the lack of widespread success with many existing quality improvement methods in healthcare,1–10 overarching quality and safety goals are a potential strategy to improve the quality of healthcare. There are currently no well developed examples of successful overarching goals in healthcare that conform to the Collins and Porras’ BHAG definition. Although this paucity of overarching quality and safety goals may reflect a difficulty in coming up with the ‘right’ goal or a scepticism of the literature from other industries on the topic, it is more likely to reflect concerns with difficulties in precisely measuring potential goals such as the relief of suffering across a population, the challenges of a rapidly evolving industry (where a 10 year time horizon is considered incredibly long), an appreciation of the pitfalls of setting such goals, concern for competing goals such as maintaining operating margins in challenging economic times, and a fear of failure.
As the public expectations for high quality and efficient healthcare escalate, it is likely that more organisations will be considering overarching quality and safety goals. Although there are minimal data to evaluate this approach in healthcare, the benefits and drawbacks of creating overarching goals have been well described in other industries. When making the decision on whether to adopt an overarching quality and safety goal in healthcare, the Board of Trustees must consider the nature of the goal, the organisational culture and risk-tolerance, the success of existing quality improvement methods, and whether the goal may promote improvements faster and more effectively than other methods under consideration. Future research should focus on methodologies for selecting successful overarching goals.
In conclusion, while the literature on BHAGs in healthcare is sparse, the management literature outlines several examples of successful and failed BHAGs. Healthcare organisations that are deciding whether to adopt a BHAG or other overarching quality goal should consider the common pitfalls of overarching goals in addition to the nature of the goal and whether it is compatible with their organisational culture and risk-tolerance.
Acknowledgments
We gratefully acknowledge the members of the Board of the Massachusetts General Hospital Physicians Organisation for their comments and lively discussion on overarching quality goals in healthcare.
References
Footnotes
-
Contributors All listed authors contributed to the conception and design, or analysis and interpretation of data; drafting the article or revising it critically for important intellectual content; and final approval of the version to be published. KCN is the guarantor, contributed to the study design, performed the literature review, data and synthesis, wrote the paper and coordinated revisions. TGF, DFT and GSM contributed to study design, data analysis and synthesis, and reviewing and editing the manuscript.
-
Funding None.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.