Article Text

Abstract
Medical errors continue to occur despite multiple strategies devised for their prevention. Although many safety initiatives lead to improvement, they are often short lived and unsustainable. Our goal was to build a culture of patient safety within a structure that optimised teamwork and ongoing engagement of the healthcare team. Teamwork impacts the effectiveness of care, patient safety and clinical outcomes, and team training has been identified as a strategy for enhancing teamwork, reducing medical errors and building a culture of safety in healthcare. Therefore, we implemented Team Strategies and Tools to Enhance Performance and Patient Safety (TeamSTEPPS), an evidence-based framework which was used for team training to create transformational and/or incremental changes; facilitating transformation of organisational culture, or solving specific problems. To date, TeamSTEPPS (TS) has been implemented in 14 hospitals, two Long Term Care Facilities, and outpatient areas across the North Shore LIJ Health System. 32 150 members of the healthcare team have been trained. TeamSTEPPS was piloted at a community hospital within the framework of the health system's organisational care delivery model, the Collaborative Care Model to facilitate sustainment. AHRQ's Hospital Survey on Patient Safety Culture, (HSOPSC), was administered before and after implementation of TeamSTEPPS, comparing the perception of patient safety by the heathcare team. Pilot hospital results of HSOPSC show significant improvement from 2007 (pre-TeamSTEPPS) to 2010. System-wide results of HSOPSC show similar trends to those seen in the pilot hospital. Valuable lessons for organisational success from the pilot hospital enabled rapid spread of TeamSTEPPS across the rest of the health system.
- Patient safety
- Quality improvement
- Teamwork
- Team training
- Safety culture
Statistics from Altmetric.com
Introduction
Numerous strategies exist to address the global issue of patient safety; however, the ongoing occurrence of adverse events in healthcare calls for adaptable and sustainable strategies that address the challenge at many levels.1–3 Organisational leaders continue to create solutions, expend time and effort to implement them, yet find improvements to be unsustainable. Staff faced with competing priorities and incessant innovations often regard new strategies as another flavour of the month.
Background
Seeking to optimise the effectiveness and sustainment of safety initiatives, our health system leadership concluded that transforming to a culture of safety was the prerequisite to attain our patient safety goals. The vision was to build a sustainable culture of safety as the foundation for our organisation to guide daily practice creating a zero tolerance for errors, and empowerment to speak up and influence actions to facilitate safety.
The impact of organisational cultures is documented; it drives behaviour and influences performance outcomes.4 Our experiences also validate that ‘the challenge of patient safety is not only clinical, but also organisational’,5 and justified the solution to build a culture of safety.
Creating a culture of safety in healthcare organisations requires the participation of all members, as healthcare delivery requires multiple caregivers to work together as an effective team with the goal of achieving desired patient outcomes and preventing harm. The quality of teamwork impacts the effectiveness of care, patient safety and clinical outcomes.6 Poor teamwork is cited as a major factor in adverse events,7 however, effective teamwork requires training and development, and formal training is recommended.6 ,8 Team training has been identified as a strategy for enhancing teamwork,9 reducing medical errors and building a culture of safety in healthcare.10
The problem
Our experience mirrored the current healthcare landscape. As a health system, we invest heavily in quality improvement which includes ongoing monitoring of patient outcomes and developing process improvement as needed. Despite numerous patient safety processes, preventable adverse events continued to occur; improvements were often short term and not sustained to our expectations.
Setting
The North Shore LIJ Health System (NSLIJHS) is comprised of 15 hospitals, two skilled nursing facilities, an institute of medical research and a medical school. It is the nation's second largest, non-profit, secular healthcare system, based on the number of beds, the nation's 18th largest healthcare network, based on net patient revenue, and the largest in New York State.
Strategies for improvement
Choice of solution
We selected Team Strategies and Tools to Enhance Performance and Patient Safety, (TeamSTEPPS), an evidence-based framework developed by the Agency of Healthcare Research and Quality (AHRQ), and Department of Defense as the intervention for organisational transformation to a culture of safety. This report will describe the use of TeamSTEPPS for team training, coupled with establishment of an infrastructure for ongoing team engagement and sustainment for building a culture of safety across a multihospital health system.
Rationale for choosing TeamSTEPPS for team training and engagement
TeamSTEPPS addresses leading causes of medical errors, and improves quality, safety and efficiency in healthcare. It is specifically designed as a resource for healthcare providers to improve patient safety through effective communication and teamwork skills.11 Its implementation is based on Kotter's Principles of Change.12 The framework is supported by over 20 years of research, and was field tested in tertiary and community, as well as civilian and army hospitals increasing its applicability across varied settings.13
This versatility fits the vision and need of our health system, as it can be adapted according to the needs of the organisation; to create transformational change (culture change) or incremental change (continuous improvement/problem solving).
All members of the healthcare team with direct or indirect involvement in care of patients need to be trained in teamwork.8 TeamSTEPPS curriculum,6 targets clinical and non-clinical members of the healthcare team leading to effective partnerships across the organisation. The profound simplicity of TeamSTEPPS increases its applicability.
TeamSTEPPS is comprised of five core principles; Team Structure, Leadership, Situation Monitoring, Mutual Support and Communication.14 Within these principles a variety of skills, competencies and checklists are clearly articulated and developed to translate the concepts into practice. The core principles lead to changes in knowledge, skills and attitude of the team members, demonstrated by a shared mental model, mutual trust and team orientation. Further, the availability of a training delivery system with a multimedia toolkit and a standardised curriculum with implementation guidelines provided free or at nominal costs by AHRQ, enhanced our choice.
TeamSTEPPS provides the organisational processes to optimise clinical interventions. For instance, an infrastructure is provided to support staff involvement and involving staff early in the change process (rather than imposing the change on them) is essential for success.15 Proactive error prevention warrants the redesign of the current system to foster organisational processes like teamwork, communication, accountability, shared decision making and problem solving to augment clinical strategies for high-quality care delivery.16
Implementation
The health system became early adopters of TeamSTEPPS; implementation began in the pilot hospital in September 2007 and was completed in 2008. In 2008, senior leadership decided to implement TeamSTEPPS system-wide and allocated resources. A corporate-level team with expertise in research and Evidence-Based Practice (EBP), education and process improvement was formed to lead the TeamSTEPPS implementation.
Communicating the vision
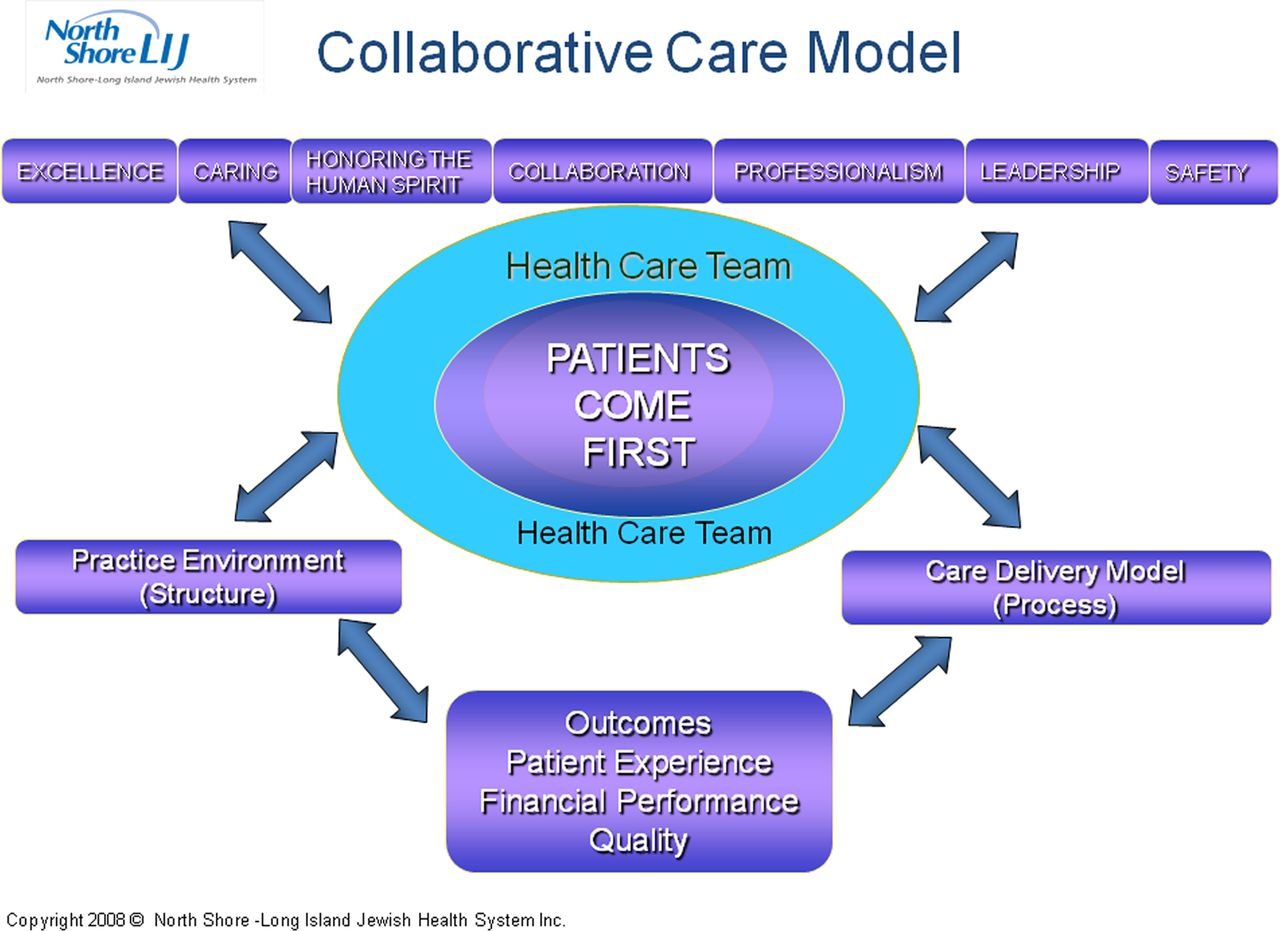
Aligning team-training objectives and safety aims with the organisational goals is recommended for creating successful training programmes.17 Our goal was to communicate the relevance of TeamSTEPPS to the organisational vision and mission, thus building a foundation for sustainment at every phase of implementation. By discussing the organisational care model (figure 1) at the beginning of every TeamSTEPPS class, and highlighting the TeamSTEPPS framework as a supporting process within that model in pursuit of our core value of safety, we communicated the relevance and permanence of the change.
{kind=link}
The organisational care model.
Within our organisational model, the Collaborative Care Model, safety is one of the core values. Donabedian's model of Structure+Process=Outcomes, supports the model's applicability and utility.18 In this model, structure refers to our practice environment, encompassing both the tangible physical environment and the intangible—the culture. Process refers to our care delivery framework, within which we embed various processes, as needed. TeamSTEPPS was introduced as a process to operationalise the core value of safety. Highlighting the model served to emphasise our philosophy and core values, even though our structures, processes or methods may change.
Creating an infrastructure for implementation and ongoing team engagement
TeamSTEPPS curriculum provides an infrastructure for implementation that includes leadership at the executive level as well as interdisciplinary front-line staff identified within the infrastructure as the Change Team.
The Change Team is described as a multidisciplinary team of leaders and staff with the expertise, credibility and motivation necessary to drive a successful TeamSTEPPS implementation.14 We customised the council-based infrastructure of our organisational care model, Collaborative Care Councils, to function as change teams at the unit/department level. These interdisciplinary teams of frontline staff are not disbanded and, thus, support the message of permanence, enabling ongoing team engagement and anchoring of initiatives. Further, the councils provide a forum for front-line teams to provide input and make decisions, increasing their accountability and empowerment.
The pilot
One of the community hospitals volunteered to be the pilot site for TeamSTEPPS. This acute care facility has 239 beds and 1300 employees. The corporate team partnered with the executive leadership of the pilot hospital to plan for TeamSTEPPS implementation using the programme's three-phase design: (1) assessment; (2) planning, training and implementation and (3) sustainment.14
PhaseI: assessment—setting the stage
The goal of Phase 1 was to determine the organisation's readiness to implement TeamSTEPPS and was exemplified by the leadership's commitment to change and willingness to allocate necessary resources.14 An overview of TeamSTEPPS was provided to the hospitals’ executive leadership, followed by in-depth discussion and planning.
Hospital leadership chose to adopt TeamSTEPPS for creation of transformational as well as incremental change. The AHRQ tool, Hospital Survey on Patient Safety Culture, (HSOPSC), was utilised to carry out an assessment of the staff perception of the culture of safety in the organisation, and served as a baseline for future measurement of transformational change post-TeamSTEPPS implementation.19 Incremental changes were to be assessed by the unit-based teams using selected preinterventional and postinterventional measures depicting the change.
Phase II: planning, training, and implementation
Phase II involved creating an action plan, conducting staff training and testing and implementation of TeamSTEPPS. The action plan addressed the goals and method of TeamSTEPPS implementation, the desired outcomes and means of measuring the outcomes.
Training
Plans were made to educate the entire hospital in TeamSTEPPS skills. The standardised curriculum included the following: (1) a 2.5-day Master Trainer course for preparing those who would train TeamSTEPPS coaches and trainers; (2) a 4 hour TeamSTEPPS Fundamentals course for staff providing direct patient care and (3) a TeamSTEPPS Essentials course to all non-clinical staff. We adopted a unique approach to Master Training, and required all formal leaders to be trained in preparation for functioning as TeamSTEPPS coaches. This aligned both with our desire to rapidly implement and to embed the skills by preparing leadership to coach and support staff. Staff were released in cohorts according to the sequence of implementation. Classes used facilitation versus a pure didactic approach; facilitation involves coordinating interactions which leads to changes in mindset.20 This meant setting the stage for open, respectful and honest dialogue. Questions and concerns were addressed, discussions proved useful in lending clarity and allaying anxiety. Physician Master Trainers were used to train voluntary physician groups, and attending physicians. Physician participation was essential to lend credibility and maintain engagement of the multidisciplinary teams.
The sequence for TeamSTEPPS implementation identified in Phase 1 was used to plan the training. The goal was to train staff in cohorts representing their work teams, with a short time lag between training and adoption of TeamSTEPPS core skills in practice. To accomplish this, a large number of classes were offered in a short time span. We offered courses twice a day, and during weekend and evening hours to accommodate staff schedules.
Responses from leadership and staff were positive. Although there was consensus that TeamSTEPPS was a great programme, questions remained on how the concepts would translate to practice and whether it would be successful. There was concurrence on wanting this new reality of a transformed culture; however, the prevailing attitude was one of believing in TeamSTEPPS utility only when the desired changes in environment were observed; emotions ranged from excitement to scepticism.
Testing adoption: unit-based pilot
TeamSTEPPS implementation was done in a pilot unit prior to spreading it in the entire organisation. The unit's council was asked to develop recommendations for translating the TeamSTEPPS tools and strategies (table 1) into practice, and a timeline was created as a guide for facilitating a rapid, systematic and structured transition.
TeamSTEPPS tools and strategies defined
The first set of tools, Briefs, Huddles and Debriefs, was selected for their relative ease of implementation, as well as likelihood of enhancing team cohesion. The unit council planned for implementing the selected tools by determining the necessary logistics of timing, leadership, date of initiation, communication plan and process monitoring. The decisions made during the council meeting were communicated to all the unit staff. The council divided the responsibility for the information exchange and agreed to function as situational leaders to facilitate implementation. During this phase, the council met every other week to expedite the process; they utilised a flipchart display in the staff lounge to communicate about the progress of implementation and outcomes.
Some TeamSTEPPS Tools, for instance, Handoff, needed more preparation time to customise, and were alternated with those that did not require the same amount of preparation. Although the use of some Tools was situation-dependent, they were added to the implementation timeline to foster learning. Conflict resolution competencies, such as DESC (refer to table 1), were reviewed during Briefs and Debriefs to reinforce and explore if opportunities to utilise the competencies were availed. During this phase, the leadership made rounds on the unit and were available to support the new processes.
Simultaneously, the council addressed improvement opportunities on the unit, starting with things that they could directly impact, such as decreasing central-line infections, ventilator-acquired pneumonia and improving throughput. It was validating to observe empowerment develop with the team's ability to rapidly brainstorm solutions. As the Pilot Unit was transitioning, word spread to other units which immediately adopted some of the ideas. While every unit had its unique set of challenges, subsequent transitions were easier, and we attribute this to favourable communication through the proverbial grapevine. TeamSTEPPS implementation for the entire organisation was completed in 15 months.
Phase 3—sustainment
Sustainment was planned from the preparation stage. The importance and relevance of TeamSTEPPS was communicated to everyone at the start of training by communicating its connection to the organisational vision and mission via the Collaborative Care Model. The message was that TeamSTEPPS was now the way we would conduct business.
Executive leadership at the pilot hospital played a crucial role in sustainment, choosing to continue as a team beyond implementation, and have evolved in their role and functions; the team continues to provide oversight and facilitate TeamSTEPPS, empowering and engaging staff through the council structure and contributing to sustainment of TeamSTEPPS. One year after implementation, all the pilot hospital units/departments were asked to disseminate their process changes and outcomes achieved through utilising TeamSTEPPS competencies at a site-wide poster session, which was open to the entire health system. The enthusiasm was contagious, and there was tremendous pride in displaying their achievements. This camaraderie and sharing enabled further team cohesion and learning. The tremendous response convinced leadership to continue with these annual sessions. TeamSTEPPS competencies are reviewed annually and are part of the organisational orientation for new team members.
Spread: system-wide TeamSTEPPS implementation
The dramatic impact of TeamSTEPPS on the culture of the pilot hospital provided impetus to the health systems’ executive leadership decision to implement TeamSTEPPS system-wide. A timeline for rapid, systematic and structured implementation was developed, (table 2).
Key steps: implementation
Templates were developed for standardising implementation at the organisation and unit levels. Standardising the process enabled us to create a shared mental model about TeamSTEPPS rollout, and evaluate its progress. From 2009 to 2010, implementation was completed in 13 hospitals and two long-term care centres and outpatient areas. To date, 32 150 employees were trained. TeamSTEPPS is included in the annual mandatory training and orientation. Redosing is planned, and an online team site is available to share best practice. TeamSTEPPS tools and strategies serve as organisational process to support clinical process improvement.
Evaluation and results
Training was evaluated using Kirkpatrick's Model (21). ‘Level I: Reaction’ was assessed by participants’ completion of course evaluation at the end the training session; 92–96% rated the course as ‘excellent’, and 1–8% rated it as ‘good’. ‘Level II: Learning’ was evaluated using TS Learning Benchmarks at the end of the training, verbally and as a group, enabling the instructors to give immediate feedback, lending further clarity.
‘Level III: Behavior’ was assessed by appraising adoption of TeamSTEPPS competencies at the unit/department level using direct observation and anecdotes. Team competencies, such as Briefs, Debriefs, Huddles and Handoffs are embedded in daily routines at all our hospitals; others competencies are used in procedures, or as needed.
‘Level IV: Results’, the effects of team training was evaluated by assessing accomplishment of our goals of transformational change (building a culture of safety) and incremental change (continuous improvement) using Hospital Survey On Patient Safety Culture (HSOPSC) and targeted variables.
Transformational change
In the pilot hospital, the HSOPSC survey was conducted in 2007 (baseline), 2009 and 2010 (table 3). The 2009 results showed significant changes22 in the dimensions of Feedback and Communication, Overall Perception of Safety, and Staffing. Although the Dimension of Staffing showed the highest improvement, the actual number of staff had not been changed. This is a testament to teamwork effectiveness, although staffing had not increased, increased team collaboration contributed to the perception of staffing improvement. Most of the other dimensions either increased or remained unchanged. However, in 2010, all dimensions show significant improvement with three dimensions, (Organisational Learning, Supervisor/Manager Expectations, and Teamwork within Units), becoming organisational strengths (>75%).
Pilot hospital results for ‘Hospital Survey on Patient Safety Culture’: difference in pre-TeamSTEPPS versus post-TeamSTEPPS implementation
The system-wide results show the same trend seen in the results of the pilot hospital pre-TeamSTEPPS and post-TeamSTEPPS validating Kotter's observation,23 ‘real transformation takes time’. Comparison of system-wide results of HSOPSC from 2009 (prior to TeamSTEPPS implementation) to 2011, showed significant improvement in the dimensions of ‘Feedback and Communication about Error’ ‘Frequency of Events Reported’, ‘Hospital Handoff and Transitions’, ‘Staffing’ and ‘Teamwork across the Units’. Considered as an area of strength with scores >75% were ‘Organisational Learning’ and ‘Teamwork within Units’.
Incremental change
Incremental changes were assessed by comparing preintervention and postintervention measures of variables depicting the change. Examples include reduction of nosocomial infections, falls, improvement in process measures and decrease in adverse outcomes, birth trauma and return to the operating room in perinatal services.24
We believe that TeamSTEPPS served to optimise other initiatives and impacted the organisations’ deep commitment to quality; NSLIJHS was honoured as the recipient of the National Quality Forum 2010 National Quality Healthcare Award.
To date, 300 Collaborative Care Councils are established across the 14 hospitals, ambulatory care and emergency medical services of the health system. The councils keep the teams engaged, and the team engagement improves our care delivery.
Discussion
Based on our findings in the areas of transformational and incremental changes, team training works. This finding is consistent with previous reports of team training impact, including improving team effectiveness and team training outcomes,7 ,25 and patient and organisational outcomes.26 The meta-analysis conducted by Salas et al supports team training as an appropriate intervention for influencing team processes and performance.27 Our findings are similar to recent reports of the impact of team training using TeamSTEPPS/modified TeamSTEPPS.10 ,28 ,29 However, methodological constraints still prevents us from directly correlating team training to clinical outcomes.30
Limitations
The scope of our implementation and train-the-trainer model required a large number of trainers. Although the curriculum is standardised, we could not monitor every training session for delivery of content or unique attributes of the trainers that could positively or negatively impact the training.
Although our TeamSTEPPS implementation was planned and organised to be rapid, we could not control the onslaught of ongoing changes or other initiatives impacting patient safety. This adds to the difficulty in attributing TS as directly impacting several outcomes. In addition, logistical constraints of implementation made it difficult to assign control units which could have strengthened our preintervention and postintervention comparisons.
Lessons learned
The implementation of TeamSTEPPS for team training and engagement has taught us many valuable lessons, (table 4).
Lessons learned table
Accountability
It is essential to establish a partnership between the team facilitating TeamSTEPPS implementation and the organisation. The organisation should select a responsible point person with clear delineation of roles and responsibility. We have subsequently used two point persons at the organisational level; one focusing on implementation of TeamSTEPPS and the other facilitating the Collaborative Care Councils.
Leadership
The role of the Executive Leadership Team is crucial in the implementation and sustainment of TeamSTEPPS. The executive team at the pilot hospital has evolved to create processes to facilitate the Collaborative Care Councils and TeamSTEPPS; they established processes to drive and monitor the changes, align activities with the mission and vision of the organisation, as well as check-back loops to exchange information. We consider this as best practice for ongoing engagement of the leadership and frontline for sustaining TeamSTEPPS and Collaborative Care Councils.
All the hospital leadership must attend Master Training sessions to enable informed decisions and participation. It is very important that they understand the TeamSTEPPS strategies in order to be a champion, role model and coach for the rest of the hospital. Additionally, leadership rounding focused on TeamSTEPPS heightens accountability and ownership.
Leadership support and involvement at all levels of the institution is critical for success. It is essential for the nurse manager and physician leader of patient care units to be champions and role models for the success of TeamSTEPPS. We also noted the importance of engaging informal leaders who often emerged through development of the council structure.
Training
Trainers should be selected carefully with consideration for their teaching and group management skills; along with the TeamSTEPPS content, trainers have to be adept at facilitating honest interactions, maintaining focus and leading the group. We have often paired trainers with content and educational process expertise to get the desired skill sets.
The plan for training should be based on the sequence of TeamSTEPPS implementation in the organisation with minimal time lag between training and implementation. Departments, disciplines and services that interact daily should be cohorted for training. This allows for the seamless integration of the TeamSTEPPS strategies in daily practice.
Team training
An interdisciplinary approach to training is essential to the acceptance and commitment of the staff. This means having an interdisciplinary team of trainers as well as attendees. Interdisciplinary attendance, including physicians, at training classes provides varied perspectives to the learning and discussion, and demonstrates organisational commitment to participants in a tangible manner. Without fail, in the few classes held that did not have interdisciplinary attendance, this was mentioned and perceived as a negative by staff.
Teams attending training together have the opportunity to engage in team building and start the TS implementation dialogue in an empowering environment.
Dosing
It is important to note that refresher training (dosing) will have to be done at intervals to maintain knowledge and practice of strategies. A study done at the health system showed a significant decrease in retention of knowledge and attitudes between three months and six months post-TeamSTEPPS training validating the need for redosing.
Implementation
The process of implementation should be standardised for all units. It must be rapid, systematic and structured. Integration of strategies should begin when 60% of the unit or department staff has completed training.
Physician participation
One of the critical factors for a successful implementation is physician involvement. Physicians need to be part of the entire process—planning, training and rollout. If the physicians do not believe that teamwork is essential for reducing errors and improving patient outcomes, it will be extremely difficult to implement team training. Physicians must be engaged as champions who believe in the importance and value of the training.31 Our experience demonstrated that physicians responded best to training conducted by other physicians. It is important that physicians are seen as leaders in TeamSTEPPS training and rollout.
Integration
It is important for TeamSTEPPS not to be seen as just another initiative that will be gone in a year or two. This can be accomplished by embedding TeamSTEPPS strategies into all the organisation's processes; quality, orientation of new staff, annual competencies, human resources and policies. Standardisation of the Collaborative Care Council agenda throughout our organisation and development of hospital-wide Central Councils created a forum for sharing best practices, accountability, sustainment and oversight for continued integration of TeamSTEPPS into practice.
In conclusion, cultural transformation is a complex process with multiple factors (table 5) influencing its success. Therefore, it is essential to adopt solutions, such as TeamSTEPPS, that are applicable to all the members of the organisation. Adopting solutions that can be easily integrated into clinical routines or workflow increases compliance and engages front-line staff ensuring sustainability. Integrating TeamSTEPPS with our Collaborative Care Councils provides the infrastructure and processes to enhance team performance with effective mechanisms for communication, problem solving and engagement of large, interdisciplinary teams impacting patient safety. The Collaborative Care Model and TeamSTEPPS are now our way of life.
Summary: implementation challenges and strategies for success
Acknowledgments
The authors wish to acknowledge the following senior leadership of North Shore LIJ Health System listed for their guidance and support: Michael Dowling, President and Chief Executive Officer. Mark J Solazzo, Executive Vice President and Chief Operating Officer. Maureen T White, RN, MBA, NEA-BC, Senior Vice President, Chief Nurse Executive. Lawrence G Smith, MD, MACP, Executive Vice President and Physician-in-Chief, Dean Hofstra-NSLIJ School of Medicine.
References
Footnotes
-
Contributors Both authors meet conditions 1, 2 and 3 according to ICMJE guidelines. Please see below for specific contributions. LT: coordinated the design of organisational model (Collaborative Care Model); designed TeamSTEPPS implementation for pilot hospital and system-wide; facilitated baseline and ongoing AHRQ Patient Safety Survey and acquisition of data, analysis interpretation; drafted and revised manuscript, final approver for publication; approved the final version to be published. CG: facilitated implementation of Collaborative Care Councils (infrastructure to support the organisational model system-wide); facilitated implementation of TeamSTEPPS system-wide, including facilitating incremental changes using TS; drafted and revised manuscript, approved version to be published; approved the final version to be published.
-
Funding None.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.