Article Text

Abstract
Background We sought to characterise the frequency, health outcomes and economic consequences of diagnostic errors in the USA through analysis of closed, paid malpractice claims.
Methods We analysed diagnosis-related claims from the National Practitioner Data Bank (1986–2010). We describe error type, outcome severity and payments (in 2011 US dollars), comparing diagnostic errors to other malpractice allegation groups and inpatient to outpatient within diagnostic errors.
Results We analysed 350 706 paid claims. Diagnostic errors (n=100 249) were the leading type (28.6%) and accounted for the highest proportion of total payments (35.2%). The most frequent outcomes were death, significant permanent injury, major permanent injury and minor permanent injury. Diagnostic errors more often resulted in death than other allegation groups (40.9% vs 23.9%, p<0.001) and were the leading cause of claims-associated death and disability. More diagnostic error claims were outpatient than inpatient (68.8% vs 31.2%, p<0.001), but inpatient diagnostic errors were more likely to be lethal (48.4% vs 36.9%, p<0.001). The inflation-adjusted, 25-year sum of diagnosis-related payments was US$38.8 billion (mean per-claim payout US$386 849; median US$213 250; IQR US$74 545–484 500). Per-claim payments for permanent, serious morbidity that was ‘quadriplegic, brain damage, lifelong care’ (4.5%; mean US$808 591; median US$564 300), ‘major’ (13.3%; mean US$568 599; median US$355 350), or ‘significant’ (16.9%; mean US$419 711; median US$269 255) exceeded those where the outcome was death (40.9%; mean US$390 186; median US$251 745).
Conclusions Among malpractice claims, diagnostic errors appear to be the most common, most costly and most dangerous of medical mistakes. We found roughly equal numbers of lethal and non-lethal errors in our analysis, suggesting that the public health burden of diagnostic errors could be twice that previously estimated. Healthcare stakeholders should consider diagnostic safety a critical health policy issue.
- Diagnostic errors
- Adverse events, epidemiology and detection
- Medical error, measurement/epidemiology
Statistics from Altmetric.com
Introduction
Diagnostic error can be defined as a diagnosis that is ‘missed, wrong, or delayed, as detected by some subsequent definitive test or finding.’1 Misdiagnosis-related harm can be defined as ‘preventable harm that results from the delay or failure to treat a condition actually present (when the working diagnosis was wrong or unknown) or from treatment provided for a condition not actually present.’2 Diagnostic error and its associated harm is a major public health problem.2 Roughly 5% of modern US hospital autopsies reveal lethal diagnostic errors for which a correct diagnosis coupled with prompt and appropriate treatment could have averted death, and these odds are generally higher in other countries.3 In the USA alone, an estimated 40 000–80 000 hospital deaths, annually, result from diagnostic errors.4 Little is known about the aggregate burden of misdiagnosis-related morbidity, but according to the Harvard medical practice study, 47% of diagnostic error-related adverse events result in serious disability,5 so the burden of non-lethal misdiagnosis-related morbidity is likely quite high.
Despite their significant impact, diagnostic errors have received relatively limited public and scientific attention, even from the patient safety community.1 ,6 In 2007, in an effort to combat this trend, the US Federal Agency for Healthcare Research and Quality (AHRQ) labelled diagnostic errors as an area of special emphasis.7 AHRQ noted that diagnostic error comprises a substantial, costly portion of all medical errors, adding that diagnostic error results from a broad array of factors including both cognitive and systems issues (eg, education, training, setting-of-care, disease-specific, domain-specific).7
Malpractice claims have been used to study various error attributes, including the epidemiology of rare surgical adverse events8 and contributing factors leading to diagnostic errors.9 Although malpractice claims data are not an ideal source to determine frequency, causes, or solutions for most diagnostic errors, they do represent an important, tangible metric of medicolegal costs attributable to misdiagnosis-related harms. In smaller studies than the present one, individual insurers have previously shown that diagnostic error-related malpractice cases account for a plurality of claims and result in larger total payments than all other categories combined.10
Although previous authors have analysed US national data to assess the overall burden of malpractice claims for adverse events, detailed analyses of diagnostic error were not reported.11 Furthermore, a detailed national-level comparison of the outcomes of diagnosis-related malpractice claims with other claim categories, such as surgery or medication-related litigations, has not previously been undertaken. Understanding more about the frequency and severity of diagnosis errors relative to other error types and across different care settings (inpatient vs outpatient) will help focus error-reduction initiatives, and may have important policy implications (eg, for tort reform, managing diagnostic test overuse, or setting research priorities). Shedding additional light on the monetary consequences of misdiagnosis-related claims may be of special interest to malpractice insurers or health systems that purchase such insurance, providing them with clearer estimates of the direct financial impact of diagnostic errors and, perhaps, offering a tangible incentive to reduce them.
We sought to analyse a large public-use national dataset of closed malpractice claims. The goals of this study were to assess the number, magnitude of payments, severity, setting and trends of US national diagnosis-related malpractice claims, and to compare them with other malpractice claim categories. We hypothesised that, among paid malpractice claims, diagnostic errors are the most frequent, most severe and most expensive. We also hypothesised that outpatient diagnostic errors are more common but less deadly than inpatient ones.
Materials and methods
Study design
This study of medical malpractice payments analysed public-use data from National Practitioner Data Bank (NPDB) during a 25-year period (1986–2010) based on the year of the alleged act or omission.12 We used medical malpractice payments for each malpractice allegation category to determine the associated cost during the 25-year study period. Other attributes for each claim (severity, setting, etc) were derived directly from the same database.
Study setting and population
The NPDB is an electronic repository of payments made on behalf of practitioners for malpractice settlements or judgments, established to implement the Health Care Quality Improvement Act of 1986. The NPDB is maintained under the authority of the US Department of Health and Human Services and first began gathering data in September 1990.13 The data file is accessible for public use, although certain details (eg, physician specialty, specific diagnosis) are maintained as confidential and unavailable for analysis.
Study protocol
The public-use data file was accessed in 2012 (898 575 total allegations dating back to acts alleged as early as 1900). We analysed misdiagnosis-related claims occurring during the 25-year period from 1986 to 2010, considering only records that had recorded payments and the year of act or omission (for trend analysis). We chose 1986 as a start date because the average time from allegation to filed claim is about 5 years, and the dataset is robust for claims filed beginning in 1990. We did not analyse data from 2011 or beyond, as there were too few diagnostic error claims recorded in the database (<100), due to the lag in claims being closed and filed. Because the time gap between allegation and payment varied widely, and secular trends in payment presumably reflect current economic conditions when payments are actually rendered, we report payment trend data by payment rather than allegation year.
Outcome measures
We describe error type, outcome severity and payments, comparing diagnostic errors to other allegation groups and inpatient to outpatient within diagnostic errors. In the online supplementary data we also describe payment sources and the geographic distribution of payments. These categories are defined in the NPDB public-use data file,12 and key classifications and definitions for our analysis are abstracted in the online supplementary methods. We grouped the nine gradations of severity as ‘minor,’ ‘disability,’ or ‘death’ for analysis. Most diagnosis-related allegations were sub-classified (error type) as ‘failure to diagnose’ (code 101), ‘delay in diagnosis’ (code 200), or ‘wrong or misdiagnosis (eg, original diagnosis is incorrect),’ but these terms are not further defined.12 Mean and total payments were calculated on an annual basis to assess for temporal trends. Where data were recorded only in a subset of years, we restricted our analysis to that date range; two important data fields were first added in 2004 (outcome severity and inpatient vs outpatient setting). Because claims filed at a later date generally reflect claims payments from an earlier time period (up to 25 years earlier), we report all analyses as 1986–2010, but note with an asterisk when data reflect a limited date range.
Statistical analysis
Descriptive statistics were used. All payment values are reported in 2011 US dollars after adjustment for inflation using Medical Care Consumer Price Index conversion factors (US Bureau of Labor Statistics).14 Data were analysed using SPSS V.17.0 (SPSS, Chicago, Illinois, USA). We calculated two-tailed χ2 p values for comparison of proportions, Student t test for comparison of means, and Mann-Whitney test for comparison of medians. We considered p<0.05 statistically significant.
Results
During the study period (1986–2010), there were 350 706 recorded allegations (all categories, including those unrelated to diagnostic error), with payment data and allegation year available. Of these, there were 100 249 diagnosis-related allegations. The mean time between the alleged act or omission and the reported payment for diagnosis-related allegations was 4.7 years (range 0–25, SD 2.4), slightly longer than that for the mean for all other allegation categories (4.2 years, range 0–26, SD 2.8). Most payments (n=93 035, 93%) were made on behalf of allopathic and osteopathic physicians. The inflation-adjusted, 25-year sum of diagnosis-related payments in 2011 USdollars was US$38.8 billion (mean per-claim payout US$386 849; median US$213 250; IQR US$74 545–484 500).
The distribution of all allegations and payments by malpractice allegation group is shown in table 1. The distribution by malpractice allegation group and outcome severity is shown in table 2. The attributable fraction of severe outcomes by malpractice allegation group is shown in table 3. Diagnostic errors resulted in death almost twice as often as other allegation groups (40.9% vs 23.9%, p<0.001) and accounted for the highest combined total number of deaths and major disability (roughly as many as the next two top categories combined) (tables 2 and 3).
Distribution of malpractice allegations and payments by primary allegation group (1986–2010)
Distribution of outcome severity and associated payments by malpractice allegation group (1986*–2010)
Attributable fraction of severe outcomes by malpractice allegation group (1986*–2010)
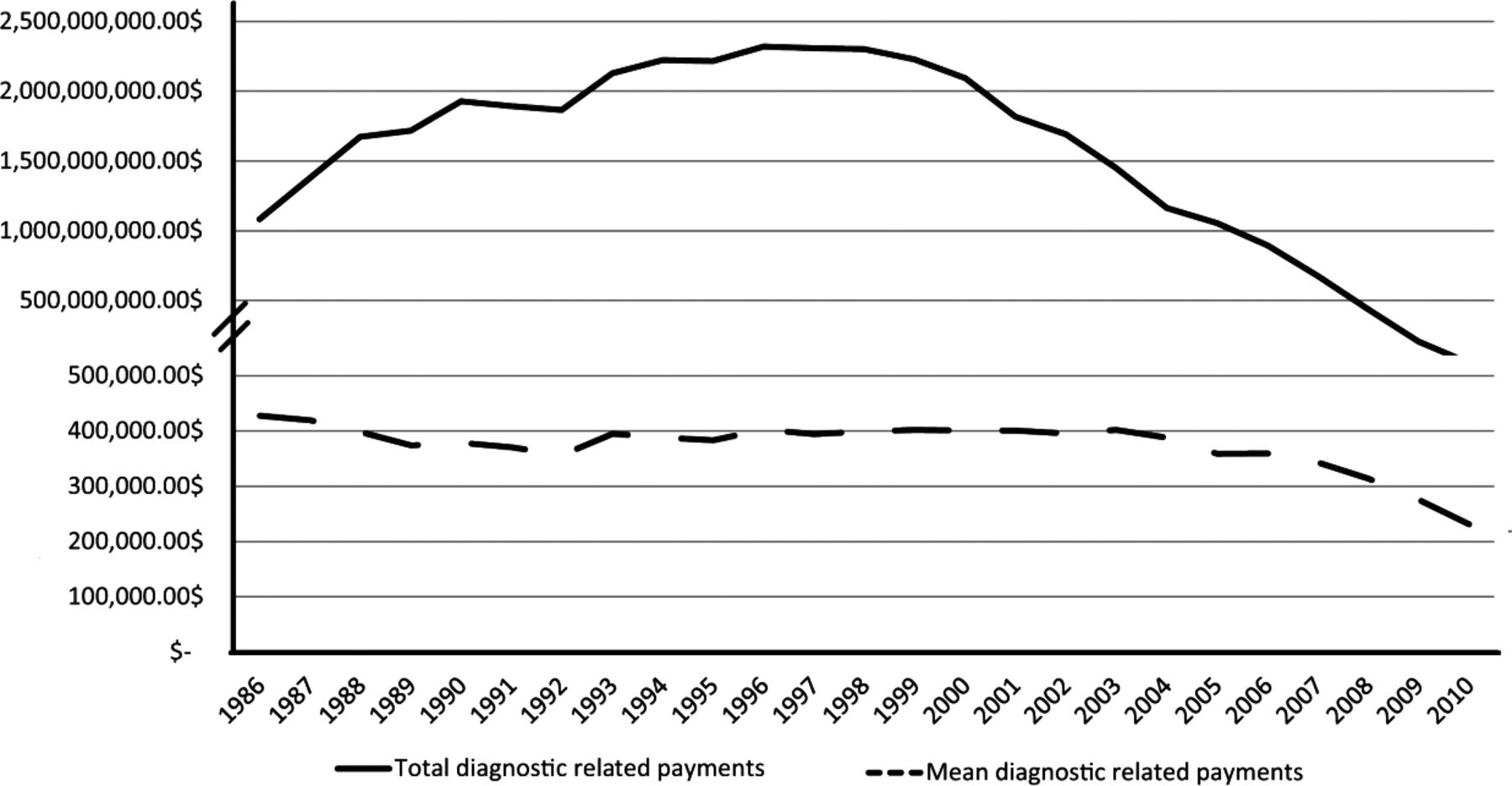
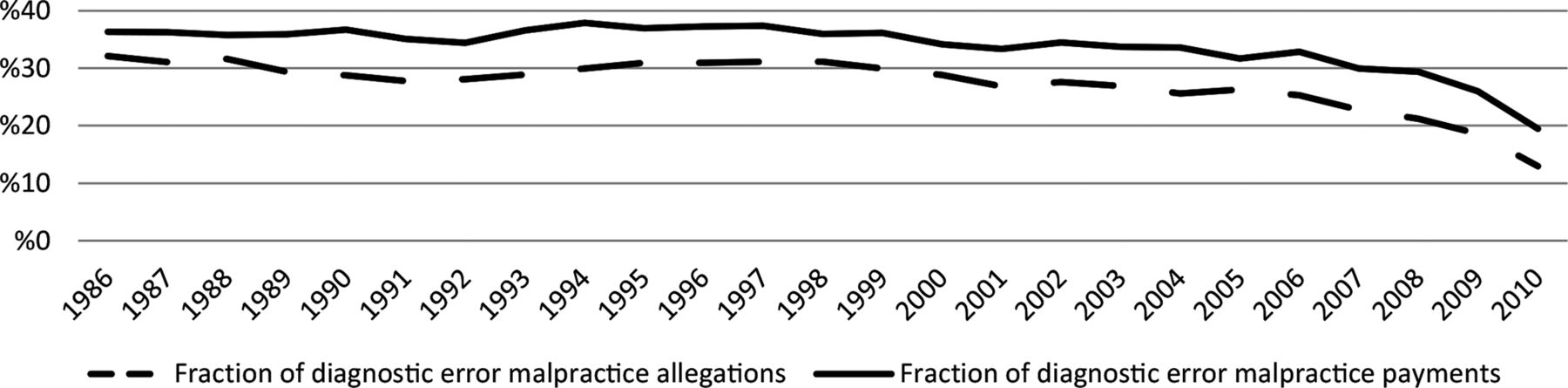
Temporal trends in the fraction of allegations and payments are shown in figure 1 and trends in mean and total payments in figure 2. The proportion of allegations and payments attributable to diagnostic error, as well as the mean payment for diagnostic error-related claims, remained fairly constant through 2005; the total diagnosis-related payments peaked in the late 1990s, and fell from 2000 to 2005 in association with a general rise and fall in total payments during that period (1986—US$2.9 billion; 1998—US$6.4 billion; 2005—US$3.3 billion). The trends were similar for outpatient and inpatient diagnostic errors (data not shown), with outpatient diagnostic error claims outnumbering inpatient claims by twofold to threefold.
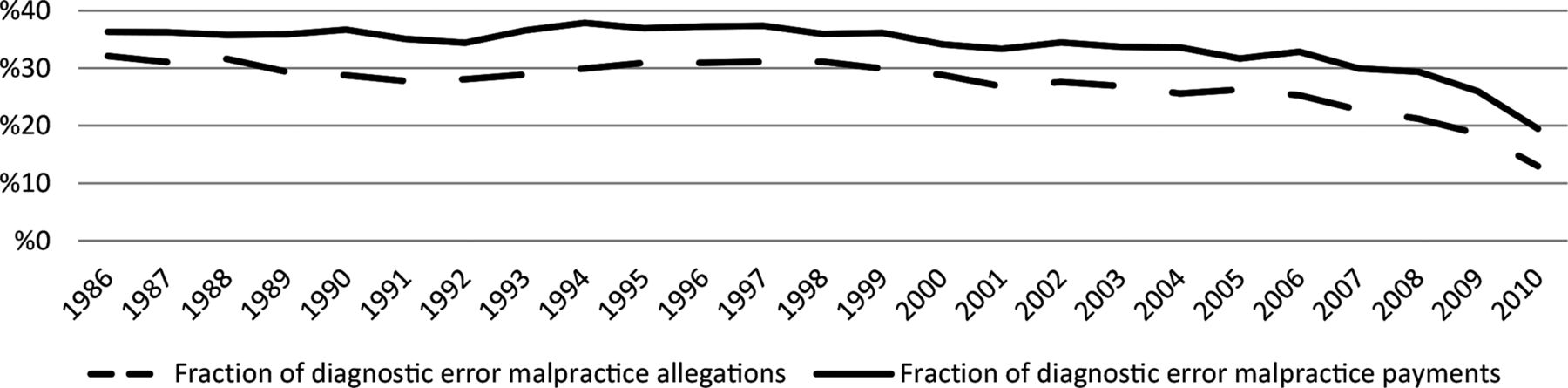
Fraction of malpractice allegations and payments attributable to diagnostic errors (1986–2010).
{kind=link}
{kind=link}
Mean and total malpractice payments for diagnostic error claims 1986–2010 by year in which payment was rendered.
The most frequent types of diagnostic error identified were failure to diagnose (54.2%, n=54 327), delay in diagnosis (19.9%, n=19 982), and wrong diagnosis (9.9%, n=9 929). The remaining 16.0% (n=16 011) included 10.0% (n=10 047) coded as ‘Allegation—Not Otherwise Classified’; all other categories accounted for <1% each. The most frequent outcomes were death (40.9%), significant permanent injury (16.9%), major permanent injury (13.3%), and minor permanent injury (10.0%). Outcomes were death or ‘disability’ (permanent injury that was ‘significant’, ‘major’, or ‘worse’) in 75.6% and ‘minor injury’ (emotional only, insignificant, temporary or ‘minor’ permanent) in 24.4% (table 2; see online supplementary methods for full definitions).
Diagnostic error-associated claims are stratified by severity of adverse patient outcome in table 4 and comparisons made between inpatient and outpatient settings in table 5. Total payments for non-lethal injuries accounted for 59% of total payments. Per-claim payments for permanent morbidity that was ‘major’ (mean US$568 598; median US$355 350) or ‘significant’ (mean US$419 711; median US$269 255) exceeded those where the outcome was death (mean US$390 185; median US$251 745). The top per-claim payments (mean US$808 591; median US$564 300) were for the outcome ‘quadriplegic, brain damage, lifelong care’ (4.5% of cases, 9.3% of total payouts). There were twice as many outpatient diagnosis-related claims as inpatient ones, and the total sum of payments was double, with similar mean payments (table 5). Inpatient diagnostic errors were more often associated with death than outpatient ones (table 5).
Distribution of diagnosis-related malpractice allegations and payments by severity of patient outcome (1986*–2010)
Comparison of diagnosis-related malpractice allegations in the inpatient vs outpatient setting (1986*–2010)
Discussion
Our results support the study hypothesis and add to the growing body of literature on the importance, frequency, distribution and consequences of diagnostic error and diagnosis-related malpractice claims. They clarify using nationally representative data that, over time, diagnostic errors have consistently accounted for the largest fraction of claims, the most severe outcomes, and the highest total payments. Outpatient diagnostic errors were more common than inpatient diagnostic errors, but inpatient errors were more likely to result in death.
Among 11 primary malpractice allegation categories, diagnosis-related claims were the leading category (28.6%) and accounted for the highest proportion of total payments (35.2%). The majority of alleged diagnostic errors resulting in paid claims were missed, rather than delayed or wrong. Diagnostic errors resulted in death or disability almost twice as often as other error categories and accounted for the plurality of these severe outcomes. Permanent morbidity (44.2%) was more common than mortality (40.9%), and the highest per-claim payments were made for devastating neurologic outcomes. The 25-year sum of diagnosis-related payments was US$38.8 billion (100 249 claims), translating to US$1.6 billion per year in annual US healthcare-related expenditures for ∼4000 claims per year. The peak in total claims and payments in the late 1990s accords with results from prior reports.15 The slight decline in attributable fraction of diagnostic error claims and payments (figure 1) and sharp decline in total payments seen from 2005 to 2010 (figure 2) was unexpected, and may simply reflect delays in recording claims payments in the NPDB database (for years with payment information recorded, there was a mean of nearly 5 years from the initial ‘act’ to ‘payment’ and the average time was longer for diagnosis-related allegations than for non-diagnosis-related claims).
Most diagnostic errors do not lead to harm,16 ,17 and resulting harms are permanent and serious in only 25% of adverse events.5 Thus, it is clear that our results primarily reflect the subset of diagnostic errors that cause more serious medical consequences. This is expected given that malpractice claims require some injury, and is consistent with our findings that more serious outcomes outnumber less serious ones 3:1 among diagnosis-related claims. Thus, paid claims are likely a more accurate surrogate for serious misdiagnosis-related harms than a surrogate measure of all harms. Nevertheless, autopsy-derived18 estimates of mortality due to diagnostic errors (∼40–80 000 deaths per year in US hospitals4 suggest that these claims data substantially understate even serious misdiagnosis-related harms (∼500 deaths per year). This roughly 100-fold disparity could exist because diagnostic errors were not recognised and reported,1 ,6 claims were never filed,19 legitimate claims were not paid,20 or NPDB data are incomplete.21 Data from the Harvard Malpractice Study indicate only 1.5% of negligent injuries result in claims,19 suggesting that most of the gap is probably attributable to the recognition, reporting and decision-to-file-a-claim stages. The consistency of this disparity (ie, ratio of errors to claims) across different studies and methods also lends credibility to the accuracy of autopsy-based national estimates of deaths due to diagnostic errors.
Aggregate estimates of total non-lethal morbidity from diagnostic errors have remained elusive.2 Our study suggests that, among malpractice claims, permanent disability is at least as common as death as a consequence of diagnostic error. Although the distribution of outcomes in malpractice cases may not be representative of adverse events from all diagnostic errors, these results do suggest that measuring mortality alone as an outcome of diagnostic errors is probably insufficient, since disability could easily be as common as death. If the hospital-based autopsy-derived mortality estimate4 is accurate, and permanent disability is, in fact, as common as death, the number of patients suffering misdiagnosis-related, potentially preventable, significant permanent morbidity or mortality annually in US hospitals alone would be 80 000–160 000. Extrapolating to the world population, this could represent 2–4 million patients globally, suffering death or disability from diagnostic error.
Perhaps not surprisingly, the highest payments were for severe, permanent neurologic morbidity. This result accords with health-related quality-of-life ratings which are consistently lowest for diseases and health states associated with adverse neurologic outcomes including stroke,22 a major cause of morbidity and mortality worldwide.23 With 1.2 million cerebrovascular events annually in the USA, and a missed diagnosis rate estimated at about 9%,24 there are probably over 100 000 missed strokes in the USA alone. It is unknown from these NPDB data how many of those with diagnostic errors resulting in disability were the result of stroke or other neurologic conditions, but the most disabling health conditions are neurologic ones.25 Taken together, these findings suggest special attention should be paid to the issue of neurologic diagnostic errors—errors are frequent, individual patients are at high risk of severe misdiagnosis-related harm, and the resulting population-based disability burden is likely high.
The majority of diagnostic errors were coded as missed (ie, ‘failure to diagnose’), and this type was 2.7-fold more common than delayed, and 5.5-fold more common than wrong diagnoses. These results merit consideration, since they differ from previously published results. In a detailed study of 100 diagnostic errors, the three types of diagnostic error were more evenly distributed (wrong 38, missed 34, delayed 28).26 Brief definitions of the three terms were published in that study, but are not well standardised, so differences might simply reflect different terminology or coding practices. If not, however, one must wonder whether missed diagnoses are more likely to result in a claim or payment. Future studies with more detailed access to case information should explore this possibility.
The large number, severity and costs of misdiagnosis-related malpractice claims underscore the need to develop effective policies regarding medical diagnosis and diagnostic error. Physician diagnostic errors, diagnostic testing behaviour, and medical malpractice claims interact in complex fashion to influence the costs and quality of care,20 especially in countries like the USA where the medicolegal tort system is active.27 There are natural tradeoffs between quality and cost inherent in the diagnostic process—more testing generally improves detection but increases costs and risks adverse consequences of testing itself and false positive results. Excessive, inappropriate diagnostic testing (‘diagnostic test overuse’28) results, in part, from fear of missing medically important diagnoses that could result in medical malpractice litigation (so-called ‘defensive medicine’).29 Some recent estimates have placed the annual US costs of defensive medicine in the hundreds of billions,30–32 but more conservative estimates suggest it is probably closer to US$45–60 billion. The costs of healthcare are increased by diagnostic errors directly through preventable adverse outcomes of the true condition, any inappropriate treatments or testing for the incorrectly diagnosed one, and malpractice claims paid. They are increased indirectly in response to malpractice claims paid by adjustments to medical liability premiums, changes in physician diagnostic test ordering behaviour (defensive medicine), and any downstream consequences (eg, costs associated with loss of the physician workforce or services as a result of intolerably high malpractice liability insurance premiums33). Theoretical arguments to the contrary, notwithstanding, empirically, the malpractice system in the USA appears to increase costs while decreasing quality and safety,20 and threatening access.34
Initiatives to reduce diagnostic error (safety) and diagnostic test overuse (efficiency) must consider this complex interplay between errors, testing and malpractice litigation. For example, efforts to reduce stroke misdiagnosis in patients with acute dizziness or vertigo seek a practice shift from commonly applied (but less accurate) neuroimaging tests to infrequently applied (yet more accurate) bedside eye movement assessment.35 ,36 Such efforts risk failure through legal challenges without tort reform policies that indemnify physicians for following well-established scientific evidence even if it is not ‘standard of care’ to do so. Similarly, initiatives focused on more effective stewardship of finite healthcare resources driven by medical societies37 or payers38 risk push-back from patients, providers, or health systems if the effect on diagnostic errors and associated malpractice claims are not considered.
Limitations
Our study could not directly assess the rate of diagnostic errors, number of adverse events, burden of harm, or preventability of harms. The correlation between paid malpractice claims and medical errors is known to be imperfect—some claims paid may be unassociated with true error, and the vast majority of true errors never result in a claim; prior studies, however, indicate that most claims paid are not frivolous20 and, despite their weaknesses, malpractice data can be taken as a crude indicator of the prevalence and seriousness of adverse medical events.11 The NPDB data regarding adverse actions against practitioners may be incomplete.21 NPDB potentially underestimates the number of malpractice payments on behalf of physicians because of the corporate shield practice, and this fraction was estimated by one study to be almost 20%.39 The frequency of petitions submitted to courts asking to dismiss malpractice claims before settlement of court proceedings is not known and, therefore, under-reporting of diagnosis-related errors is a likely possibility.40 Methods for determining diagnostic error and subtype were not described in the NPDB manual and patients may have been misclassified. Data were not available to us in the public-use version of NPDB to discern the types of clinical problems or clinical specialties most frequently involved. Despite these limitations of the NPDB, it remains the most complete source of malpractice payment data available in the USA.
Conclusion
Our results confirm that, among malpractice claims, diagnostic errors are the most frequent, most severe and most costly of all medical mistakes. We found roughly equal numbers of lethal and non-lethal errors in our analysis, suggesting that the public health impact of diagnostic errors could be substantially greater than previously estimated based on autopsy data that consider only lethal errors. Around the globe, millions of patients may suffer misdiagnosis-related harms each year. In the USA, diagnostic errors appear to be an important driving factor in the negatively synergistic cost and quality relationships among large claims payouts, rising malpractice premiums, and defensive medicine. Stakeholders, including patients, insurers, hospital systems and federal agencies should have a vested interest in making diagnostic error reduction a patient safety and health policy priority.
Because of the key role of diagnosis-related malpractice claims paid, and the unsustainably high costs of defensive medicine, health policy and tort liability reform initiatives intended to reduce malpractice claims and defensive medicine (while maintaining or improving healthcare quality and safety) should probably consider specific policies related to diagnostic error. Error-reduction initiatives should emphasise strategies that minimise misdiagnosis-related harms, rather than errors, per se. Strategies designed to reduce the costs of diagnosis by streamlining diagnostic testing protocols should consider both the direct and indirect costs of diagnostic errors in determining cost effectiveness. Future research should define the clinical contexts in which harms from diagnostic errors are greatest, assessing whether neurologic diagnostic errors account for a disproportionate share of misdiagnosis-related harms.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
- Data supplement 2 - Online appendix
Footnotes
-
Contributors DEN-T and ASST had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. AST: conceived manuscript concept; designed analytic plan; drafted manuscript; reviewed and critically edited the manuscript; approved the final version. HWL: assisted in design of analytic plan; reviewed and critically edited the manuscript; approved the final version. SCM: assisted in design of analytic plan; reviewed and critically edited the manuscript; approved the final version. AS: assisted in design of analytic plan; reviewed and critically edited the manuscript; approved the final version. MM: assisted in design of analytic plan; reviewed and critically edited the manuscript; approved the final version. PJP: assisted in design of analytic plan; reviewed and critically edited the manuscript; approved the final version. DEN-T: conceived manuscript concept; designed analytic plan; drafted manuscript; reviewed and critically edited the manuscript; approved the final version.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.