Article Text

Abstract
Objective aim Identify and eliminate barriers to HIV testing in primary care and to decrease the rates of patients never being tested, and limit unnecessary repeat testing.
Setting Primary care clinics within an urban publicly funded safety net hospital and community health system in Cleveland, Ohio. Reported HIV prevalence among male Cleveland residents is 1193.5/100 000.
Design A time series analysis using statistical process control was used.
Methods Primary care encounters of patients aged 13–64 years from selected sites were reviewed throughout the initiative for HIV testing prior to the visit and associated with the visit.
Results Run charts of the proportion of men and women never tested for HIV demonstrated marked improvement and special cause variation with six sequential quarters falling outside of the trend lines. Evaluation of encounters associated with a first HIV test confirmed testing occurring within primary care rather than elsewhere in the health system.
Conclusions Implementing an electronic medical record-based reminder effectively increased HIV testing among primary care patients not previously tested, while education and practice feedback alone did not.
- Reminders
- Decision Support, Computerized
- Quality Improvement
Statistics from Altmetric.com
Background and knowledge
On 13 July 2010, the White House released the National HIV/AIDS Strategy calling for efficiencies that allow for increased testing, identification of people living with HIV, and linking them into care.1 The Centers for Disease Control and Prevention (CDC) estimate that 1.1 million people in the USA are living with HIV, nearly three-fourths of them being men (CDC, 2008).
Since 2006, the CDC has recommended HIV testing for all individuals between age 13 and 64 years at least once in their lifetime.2 Prior to 2006, testing was routinely recommended only for pregnant women, individuals at high risk, or living in areas with prevalence greater than 1%, or for patients seeking services for sexually transmitted infections.3 ,4 Traditional testing guidelines limited the number of patients due to the HIV risk assessment requirement, a known barrier to HIV testing.5 The revised recommendations received widespread support with most primary care professional organisations providing policy or consensus statements encouraging implementation.6 ,7 Support for these guidelines has facilitated revision of most state laws to allow more ‘routine’ HIV testing.8 ,9 In November 2012, the US Preventive Health Services Task Force endorsed HIV testing as a grade A recommendation ensuring that it will be a covered service under the new Affordable Care Act.10
By performing routine HIV screening, patients may be diagnosed earlier which can improve outcomes for those diagnosed, and has a public health impact through reduced transmission of the disease.11 ,12 As such, numerous initiatives to increase and support HIV testing in medical settings are underway.13 However, HIV testing has a unique set of barriers that is not seen with most other preventive screening recommendations.
HIV testing has been stigmatised and treated with exceptionalism. It is the only blood test that can be performed anonymously with some states requiring the availability of an anonymous testing as an option. HIV testing, historically, required patients to provide signed informed consent, as well as pretest and post-test counselling (current laws continue to vary by state). As a result, it was often sought out or offered as a standalone screening test and not part of routine medical care. Additionally, the rigorous requirements around testing led to misunderstandings between providers and patients. Many providers did not test for fear of breaking the rules or perceiving the patient to not be at risk. On the other hand, patients believe HIV testing to be part of routine testing whenever they had their blood drawn, if hospitalised, or having surgery.
Successful usage of public health screening recommendations require acceptance by patients and provider. Early screening and treatment for diseases, such as diabetes, heart disease, cervical, colorectal and breast cancer have been linked with improved health and longevity. Despite this association with improved health outcomes, widely accepted screening guidelines have less than optimal usage.14 ,15 Men, as well as minority populations, are noted to have lower usage of preventive health screenings; this poses a significant issue as the burden of a disease is predominantly among these same populations.16–19
Electronic medical records (EMR) offer opportunities to accelerate quality improvement (QI) through clinical decision support features20; however, factors such as current patient care workflow, end-user acceptability of reminders, provider beliefs regarding recommendation and familiarity with EMR need to be considered.21 ,22 Prior to the revised guidelines, a Veterans’ administration (VA) project using clinical decision support increased HIV testing among patients with risk factors identified by the medical record,23 however, a separate VA study using a ‘low-intensity’ clinical reminder did not increase HIV routine screening or HIV risk assessment despite a high prevalence of risk factors among patients.24 Both interventions involved provider education but occurred prior to the 2006 CDC guidelines. In 2010, we successfully increased HIV testing among patients not previously tested using an EMR-based reminder.25 The steps necessary for its success have not been described previously.
Local problem
A basic analysis of HIV testing completed within the health system between 2002 and 2007 showed an annual increase in total tests completed but a decline in newly identified cases each year. Total tests completed were less than 5% of total outpatient encounters for each year. The majority of tests were completed among outpatient women and most often linked to prenatal care.
Intended improvement
The purpose of this project was to identify and eliminate barriers to HIV testing in primary care, to decrease the rates of patients never being tested, and to limit unnecessary repeat testing.
Specifically, the intended improvement was to increase the proportion of men and women between the ages of 13 and 64 years who know their status by being tested in the healthcare system where they receive primary care. To decrease missed opportunities for HIV testing most efficiently, we sought to define the proportion of missed opportunities as well as the characteristics of patients who have never been tested. This information would be used to explore barriers and define interventions that would increase first-time HIV testing within the health system by incorporating it into routine primary care.
Given the nature of the project, the QI team was primarily an infectious disease specialist and an education specialist who met with numerous key stakeholders in primary care and graduate medical education. Additional support and expertise was sought with institutional quality experts and members of the hospital's informatics group.
Methods
Setting
The Greater Cleveland area is one of Ohio's highest-prevalence areas with most cases residing within the city limits. The Cleveland Department of Public Health reports an HIV/AIDS rate of 770.9/100 000 among all Clevelanders, and 1193.5/100 000 among male Clevelanders.26 Cases are concentrated in areas with high rates of poverty. The MetroHealth System (MHS) is a publicly funded academic teaching hospital, and the primary provider of indigent care to the community, and is comprised of a major medical centre, a rehabilitation hospital, a long-term care/skilled nursing centre, an outpatient surgery centre, and a network of satellite community-based healthcare centres (CHC). Many of the CHCs are located in areas of high medical need. The health system is also the primary provider of Ryan White funded HIV medical care serving over 1200 unique patients living with HIV in 2011. MHS employs approximately 500 physicians (20% of whom provide primary care to adolescents and adults), 110 Nurse Practitioners, 365 graduate medical trainees (residents and fellows, 120 of whom are in Internal Medicine, Medicine/Paediatrics, or Family Medicine), and hosts 350 medical students annually.
The health system supports a fully integrated EMR system which has been in place for more than 10 years. One feature of the EMR is a health maintenance list that is used for general preventive health activity reminders (tetanus vaccination) as well as specialty practice (such as routine haemoglobin A1C monitoring for diabetic patients). Usage of this health maintenance feature has been encouraged by an institution supported QI programme.
Planning the intervention
Between June and December 2009, we identified five community health centres and two main campus clinics to be targeted, and met with key stakeholders from these sites prior to educational sessions. The health centres were chosen because of their location in neighbourhoods with a high incidence and prevalence of HIV and, therefore, had the greatest likelihood of unidentified HIV infection and are the primary healthcare option for residents of these neighbourhoods. Information systems extracted encounter data from the identified sites to establish a baseline of testing practices. Baseline data at all sites showed very high rates of patients never being tested, particularly among men. These reports were used to engage stakeholders (lead physician and nurses for each site) and gain their support for an intervention to increase testing.
Based on the initial experience with providers, there were knowledge gaps regarding who should be tested for HIV in addition to structural and legal barriers. Education included local HIV epidemiology, their group practices specific HIV testing information, an update on HIV testing laws, case studies of missed opportunities, as well as reminders on the benefits of routine testing, including early detection and early treatment and resources for HIV care. Providers voiced support, though most were concerned about lack of time to incorporate testing into routine practice, and little change was observed with education alone.
EMR-based intervention
In July 2010, the EMR health maintenance list was modified to include ‘HIV test once’. The reminder automatically incorporated prior testing within the health system (since EMR was available—1999 to present) such that patients who had been previously tested were shown to have this activity as complete. The health maintenance list is a passive reminder in that it does not need to be reviewed or acknowledged to complete a visit and will remain active if ignored. When there are items to complete, a red ‘HM’ (health maintenance) appears in the upper right corner of the header of the patient's chart (figure 1). Providers may click on the ‘HM’ to view activities (figure 2). Providers may perform the activity (ie, order the test, vaccine, etc), as well as mark as declined, previously completed elsewhere, or done. Notes may be added detailing the reason for an override, but are not required. The activity may also be marked postponed which makes the HM go away temporarily but returns to active at future encounters. The reminder does not prevent repeat testing, though it tracks dates of testing and includes a hyperlink to the test result. HIV testing was not added to the selected quality measures for practice reports. Providers and support staff were notified of the modification at informal lunch and learn meetings.

Chart review mode. The red 'HM' will be present in the patient header if there are preventive health items due.
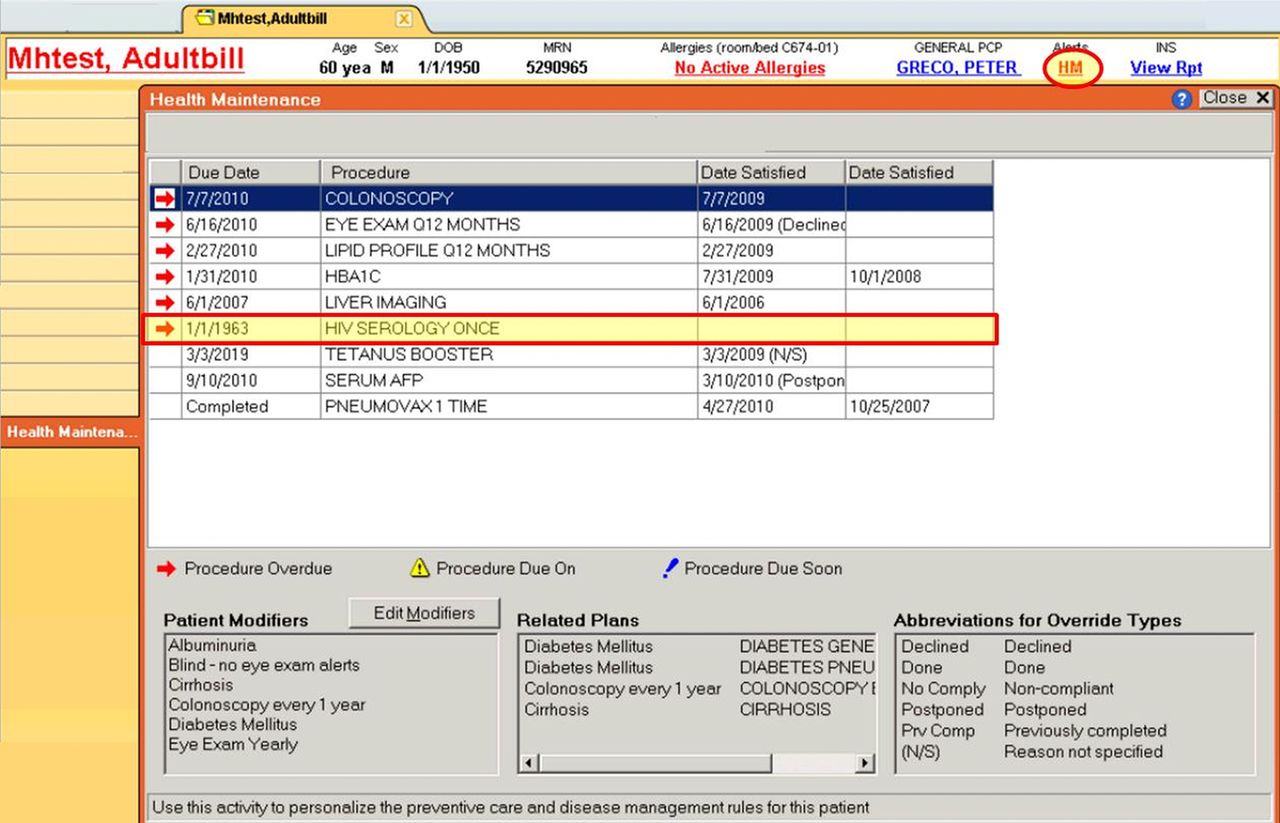
Health maintenance detail. Clicking on the HM takes the user to this screen which details why the ‘HM reminder’ is present as well as contains dates and hyperlinks to previously completed items.
Evaluation of the intervention
To evaluate the effect of the intervention on screening, we used control chart methodology to look for significant trends and decreased variation. We reviewed encounters for testing on current visit as well as one's testing history. A missed opportunity was defined as an encounter in which a patient was not tested for HIV and had not been tested previously within the health system. First-time testers were defined as patients who had no prior record of HIV testing in the system and were tested in association with a primary care visit. Repeat testers were defined as patients who had a prior record of HIV testing in the system and were tested in association with a primary care visit. Over-rides were not reviewed nor incorporated in this analysis. Encounters were aggregated by quarter, by clinic location and provider type, as well as by patient age, gender and race to determine trends in testing. Patients previously diagnosed with HIV were excluded from the analysis, as were encounters occurring after the diagnosis for patients newly diagnosed with HIV. Chart reviews were performed on all positives to confirm the patient was newly diagnosed in that encounter.
Primary care outpatient encounters for patients aged 13–64 years from hospital-based primary care clinics and the five targeted health centres between January 2008 and December 2011 were included. Primary care encounters included provider visits (medical doctor (MD)), doctor of osteopathic medicine (DO), APN) in Internal Medicine, Medicine/Paediatrics, and Family Medicine.
Analysis
Between January 2008 and December 2011, a total of 419 522 (289 436 women and 130 086 men) outpatient encounters qualified for analysis. The characteristics of patients included in the study are shown in table 1. Data from 2008 was used to establish a baseline rate of subjects being tested for HIV. We used p charts to trend rates of patient encounters that were never tested for HIV, first-time testers, and repeat testers. P charts control for variations in volumes as was seen among the selected sites. Of note, the intervention correlated with the economic downturn and as a safety net provider, the system experienced an increase in volumes. We aggregated the results by gender, age, practice type and practice site and updated them quarterly. Ongoing analysis of encounter-level data continues to be used to evaluate the effect of the intervention. All analyses were conducted in SPSS V.17.0.
Results
Following the addition of HIV testing to the health maintenance reminder list in the EMR, there was a significant decrease in subjects who were ‘never tested’. The trend line extending outside of the upper control limit (UCL) and lower control limit (LCL) for greater than six periods in both men and women provide evidence for special-cause variation and suggest the impact is related to a change in process rather than chance variation (figures 3 and 4). Simultaneously, there was an increase in encounters in which a first-time test occurred, verifying the change was occurring as a result of increased testing in primary care rather than elsewhere in the system (figure 5). The trend line in figure 5 remains within the UCL and LCL demonstrating stability within the new process.
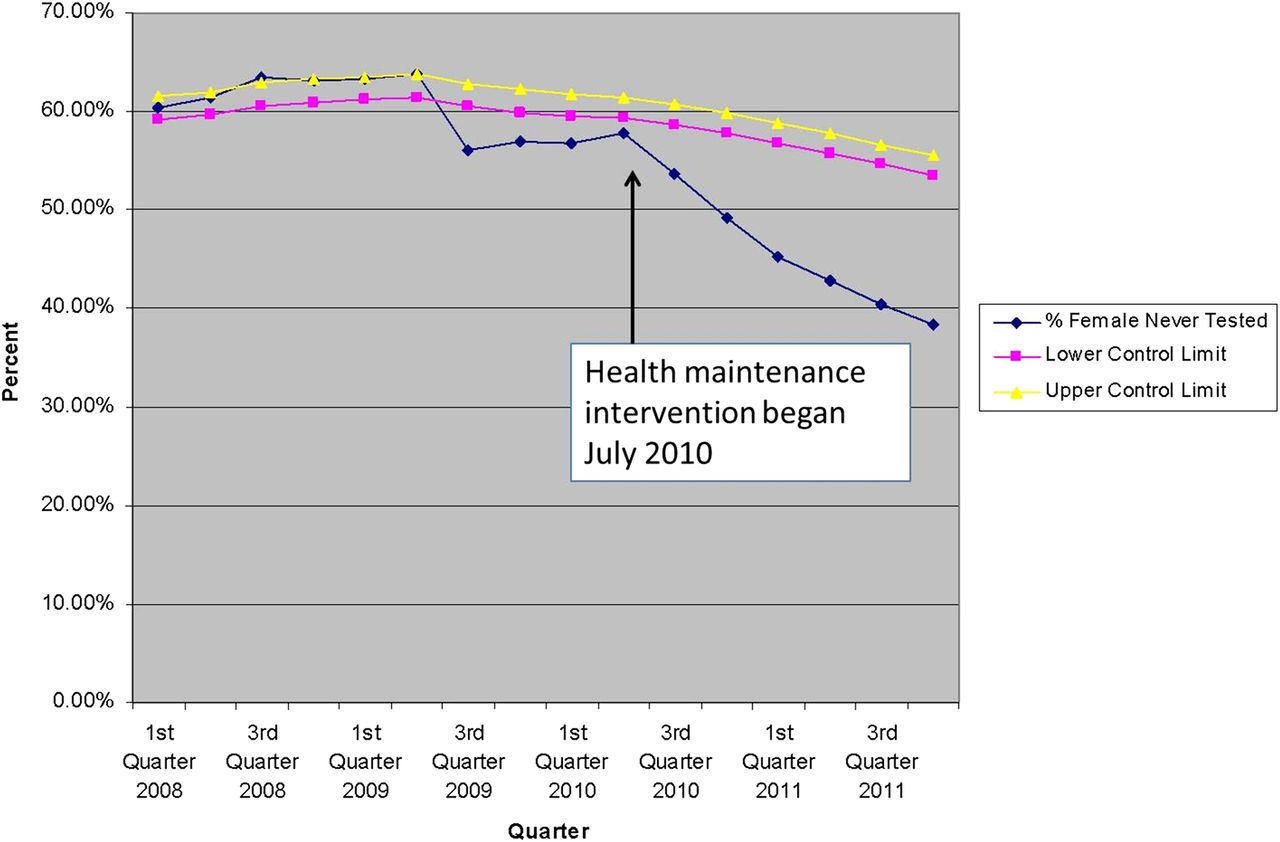
Percentage of females never tested.

Percentage of males never tested.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Percentage of first time test - all patients.
Additionally, there was no change in testing rates among patients previously tested after the reminder was implemented (data not shown). Improvement occurred in both men and women and among all practice sites and practice types except for one that tends to provide urgent care and hospital follow-up. (see online appendix table A1) When reviewing by age and gender, significant improvement occurred among all men over 18 years of age and among women 25 years and older.
Importantly, increased testing increased the identification of previously undiagnosed HIV with 33 new diagnoses in 2010–2011 versus 22 in 2008–2009. In all year groups, men were more likely to test positive than women (0.6–0.8% vs 0.1%).
Discussion
The purpose of this project was to identify and eliminate barriers to HIV testing in primary care, decrease the rates of patients never being tested, and limit unnecessary repeat testing.
This specific project focused on HIV testing in primary care, so we included a measurement of first-time testing associated with a primary care visit to confirm a change in primary care provider behaviour rather than elsewhere in the healthcare system. The intervention successfully increased testing among patients previously never tested without increasing repeat testing. We noted previously that 80% of patients who tested positive for HIV during 2008–2009 had not been tested before in the system27 which supported the focus on first-time testing of patients. By minimising repeat testing among patients without acknowledged risk, there is a lower cost of the intervention and a likely greater yield of new cases per test performed.
Additional time was an important barrier to address for providers. The intervention successfully addressed this concern in two ways. First, the HM reminder reduced providers’ time in determining who needed to be tested. More importantly, because the HM reminder is already used by providers of primary care, no additional keystrokes or steps were needed to view the reminder or incorporate it into their patient workflow. Additionally, no providers voiced concerns about additional time needed for testing after the intervention.
At the start of the intervention, Ohio testing law still required additional informed consent as well as pretest and post-test counselling for all patients. When testing laws were being revised, we capitalised on our relationships with stakeholders at many levels in the system to advocate for and rapidly implement institutional policy changes to be consistent with revised Ohio testing law. Adoption of the revised laws also decreased providers’ time concerns.
The initiative achieves the National HIV/AIDS Strategy (NHAS) goal to reduce new infections by increasing the number of persons who know their status as well as increasing those testing positive being successfully linked to care.1 Based on prior practice, we believe that many of the newly diagnosed patients would not have been tested and diagnosed without the initiative, thus, the initiative was also successful at identifying and initiating care at an earlier stage when treatment is more beneficial.28
Our project is novel in its incorporation of an EMR-based strategy and its focus on ambulatory primary care. The ongoing identification of new patients who may benefit from treatment justifies its benefit. We focused on the primary care setting as many providers locally felt that it was the most appropriate place for patients to be routinely tested, and the HM list presented a unique intervention opportunity. By incorporating HIV testing into primary care, we helped demystify HIV testing for patients and providers.
While the intervention increased testing, many patients remain untested after their visit in primary care. Reasons for not testing were not assessed and it will be important to do so in the future to continue to improve rates of testing. Another limitation is inability to automatically incorporate external testing data as well as the lack of pre-1999 data. Routine testing for pregnant women has been recommended since 1995.29 Higher rates of ever testing may be seen, especially among older women, if historical data were available.
Conclusion
We demonstrated that an EMR-based reminder effectively increased provider-initiated HIV testing among ambulatory primary care patients. This low-cost intervention demonstrates one of the advantages and improved health outcomes that can be seen with meaningful use of an EMR. We believe that the intervention would be easily reproduced in a similar setting and should be effective for other preventive health screening activities. Key elements that facilitated success included an established and comprehensive EMR system and incorporating testing in an existing workflow with modification rather than creating an additional step. The cost to replicate the project is nominal: limited to programming, provider education time and evaluation.
Acknowledgments
Portions of this work have been presented at the 2010 Infectious Disease Society of American (IDSA) Annual Meeting in Vancouver, British Columbia; at the 2010 National Summit on HIV Diagnosis, Prevention and Access to Care in National Harbor, Maryland; at the 2011 National HIV Prevention Conference in Atlanta, Georgia, and the 2011 American Public Health Association meeting in Washington, DC.
References
Footnotes
-
Contributors AKA, AC and MDT all contributed to the conception and design, or analysis and interpretation of data drafting the article or revising it critically for important intellectual content and final approval of the version to be published.
-
Funding This project was funded in part by the AIDS Funding Collaborative, Cleveland, Ohio.
-
Competing interests None.
-
Ethics approval The study was performed under MetroHealth IRB review, study protocols: MHS IRB: 07-00590 and 10-0366. Interventions were targeted to healthcare providers, outcome evaluation was performed retrospectively.
-
Provenance and peer review Not commissioned; internally peer reviewed.