Article Text

Abstract
Objectives: Emergency medical service systems in Norway are based on equity and equality. A toll free number (113) and criteria based dispatch are crucial components. The establishment of an emergency medical system (EMS) manned by an air and ground emergency physician (EP) has challenged the role of the general practitioner (GP) in emergency medical care. We investigated whether there were any geographical differences in the use of 113, alerts to GPs by the emergency medical dispatch centres (EMDCs), and of the presence of GPs on scene in medical emergencies leading to a turnout of the EP manned EMS.
Methods: This was a prospective, observational cohort study of 385 000 inhabitants covered by the two EMDCs of Rogaland county, Norway, including 1035 on scene missions of the EP manned EMS during the period 1998–99.
Results: The proportion of emergency calls routed through 113 was significantly lower, the proportion of alerts to GPs significantly higher, and the proportions of GPs on scene significantly higher in rural than urban areas.
Conclusion: We found geographical differences in the involvement of GPs in pre-hospital emergency medical situations, probably caused by a specialised emergency medical service system including an EMDC and an air and ground EP manned EMS. There were geographical differences in public use of the toll free 113, and alerts to GPs by the EMDCs, which is likely to result from geographical conditions and proximity to medical resources. Future organisation of the EMS has to reflect this to prevent unplanned and unwanted autonomously emerging EMS systems.
- CBD, criteria based dispatch
- EMDC, emergency medical dispatch centre
- EMS, emergency medical service
- EP, emergency physician
- GP, general practitioner
- LDC, local dispatch centre
- emergency medical service
- general practitioner
- geographical differences
- prehospital
- toll free emergency number
Statistics from Altmetric.com
- CBD, criteria based dispatch
- EMDC, emergency medical dispatch centre
- EMS, emergency medical service
- EP, emergency physician
- GP, general practitioner
- LDC, local dispatch centre
- emergency medical service
- general practitioner
- geographical differences
- prehospital
- toll free emergency number
The Norwegian emergency medical service (EMS) system intends to provide help regardless of time and place by a uniform alert and response system. It is internationally recognised that criteria based dispatch (CBD) of ambulances, and use of a three digit number for medical emergencies, are useful tools in this effort,1,2 and have therefore been adopted and implemented in many countries.3–5
In Norway, the parliament passed a new legislation in 1990 aimed at consistency in organising the EMS systems nationwide. A dedicated toll free phone number, 113, routes calls to emergency medical dispatch centres (EMDCs), which dispatch ambulances and/or general practitioners (GPs) based on criteria in the Norwegian Index for Medical Emergencies (known as the Index).6
GPs have traditionally been part of the Norwegian EMS system, including for the most acute cases, and particularly in rural areas where the patient may be hours away from the nearest hospital. With the establishment of a nationwide EP manned air and ground EMS in 1988, and presence of the EMDCs, together with increasing competence of ambulance personnel, the role of the GP on call has been challenged. The objectives of the present study of medical emergencies leading to an acute response by the EP manned EMS were to explore any geographical differences in: the public use of the single three-digit number, 113; the EMDC alerts to GPs on call; and to what extent GPs on call were present on scene.
MATERIALS AND METHODS
Emergency medical dispatch
Rogaland county in southwestern Norway (fig 1) has a population of about 385 000. Fjords crossed by ferries divide the county into a southern part with the densely populated city of Stavanger, and a northern part with the city of Haugesund. Both cities have a hospital with an EMDC staffed by nurses and ambulance personnel. The response is based on criteria given by the Index.6

Map of Norway. Detail is the county of Rogaland.
The Norwegian Index is a further development of CBD first developed in Seattle and King county.1 The Index is a decision tool to secure an appropriate response to a medical emergency. It is based on clinical signs, symptoms, or events, not diagnosis, presented in 40 categories such as unconsciousness, fever, and chest pain, with subgroups of criteria for various responses. According to the Index, each call is classified either as: “acute”, with the highest priority; “urgent”, with a high, but lower priority; or “not urgent”, with the lowest priority. With “acute” calls, both ambulances and the GP on call should be alerted. In addition, the EP manned EMS is alerted if the EMDC operator believes there is a chance for an improved outcome based on the expertise of the EP, or on the time element for longer transports. “Not urgent” calls received through 113 are transferred to local dispatch centres (LDCs), established in most municipalities in Rogaland, and the situation is handled by GPs on call. The LDCs also have individual, local telephone numbers that the public should call if they feel, as described in all telephone directories, that “help can wait a little while”. If a call to the LDC, staffed by a nurse, is recognised as “acute”, it should be transferred to an EMDC.
The GPs are family physicians, being on call according to rotation, thereby participating in the EMS.
A 113 call is automatically routed to the EMDC nearest to the emergency. Calls for assistance by the EP manned EMS are routed to the EMDC in Stavanger. EMDC, LDC, ambulances, GPs on call, and the EP staffed ambulance communicate and co-operate through a closed radio system.
The emergency physician manned EMS
The EP manned EMS, carrying a board certified anaesthesiologist from Rogaland Central and University Hospital, Stavanger, carries out approximately 400 air and 600 ground missions per year. The average time interval from alert to start of the mission is 2 minutes.
Data in this study
We chose to study the calls attended to by the EP manned EMS, as these were likely to be the most severe cases, for which the type and timing of response were most likely to affect outcome. During an 18 month period, 1 March 1998 to 31 August 1999, we included all on scene EP manned EMS missions classified as acute primary missions, in the Stavanger and Haugesund EMDC areas. The EP gave a tentative diagnosis and severity score, using the NACA Severity of Injury or Illness Index7 (table 1). For further analyses, patients were dichotomised into two groups; NACA score 0–4 and 5–7 (patients with injuries/diseases with acute threat to life or worse) and the diagnoses into six groups; cardiac arrest, cardiac diseases, respiratory failure, trauma, deliberate self intoxication, and miscellaneous diseases, based on full hospital reports in addition to the reports from the flight physicians and dispatch centres.
The eight level Severity of Injury or Illness Index (NACA scale) for grading injuries or diseases
The patients were classified into four age groups; ⩽15 years, 16–54 years, 55–69 years, and ⩾70 years.
The population figures of the municipalities were retrieved from Statistics Norway.8 The 282 000 people covered by the EMDC in Stavanger were split into four geographical groups depending on the distance from the centres of the municipalities to the hospital in Stavanger, the base of the EP manned EMS. The 103 000 people covered by the EMDC in Haugesund, including about 10 000 from the neighbouring county Hordaland, constituted a separate geographical group. The routing of emergency calls to EMDCs or LDCs, the alerting of GPs on call by EMDCs, and the presence of GPs on scene, were analysed according to geographical, age, and diagnostic groups.
Data were collected and entered into a database constructed with FileMakerPro (version 4.1; FileMaker Inc., CA, USA) and analysed by SPSS (version 10.0; SPSS Inc., IL, USA). The Norwegian Social Data Services and the regional committee for medical research ethics approved the study.
Statistics
The risk ratios for a medical emergency situation, being alerted through 113 or through the phone of the LDC, for the GP on call being contacted by the EMDC or not, and whether an alerted GP was on scene or not, were tested in Cox regression models adjusted for geographical group, sex, age, NACA score, and diagnostic groups. In addition, analysing for factors associated with the GP being on scene or not, was stratified for whether the GP was contacted or not. Any differences between NACA subgroups were tested by χ2 tests. Less than 1% probability of error was considered significant.
RESULTS
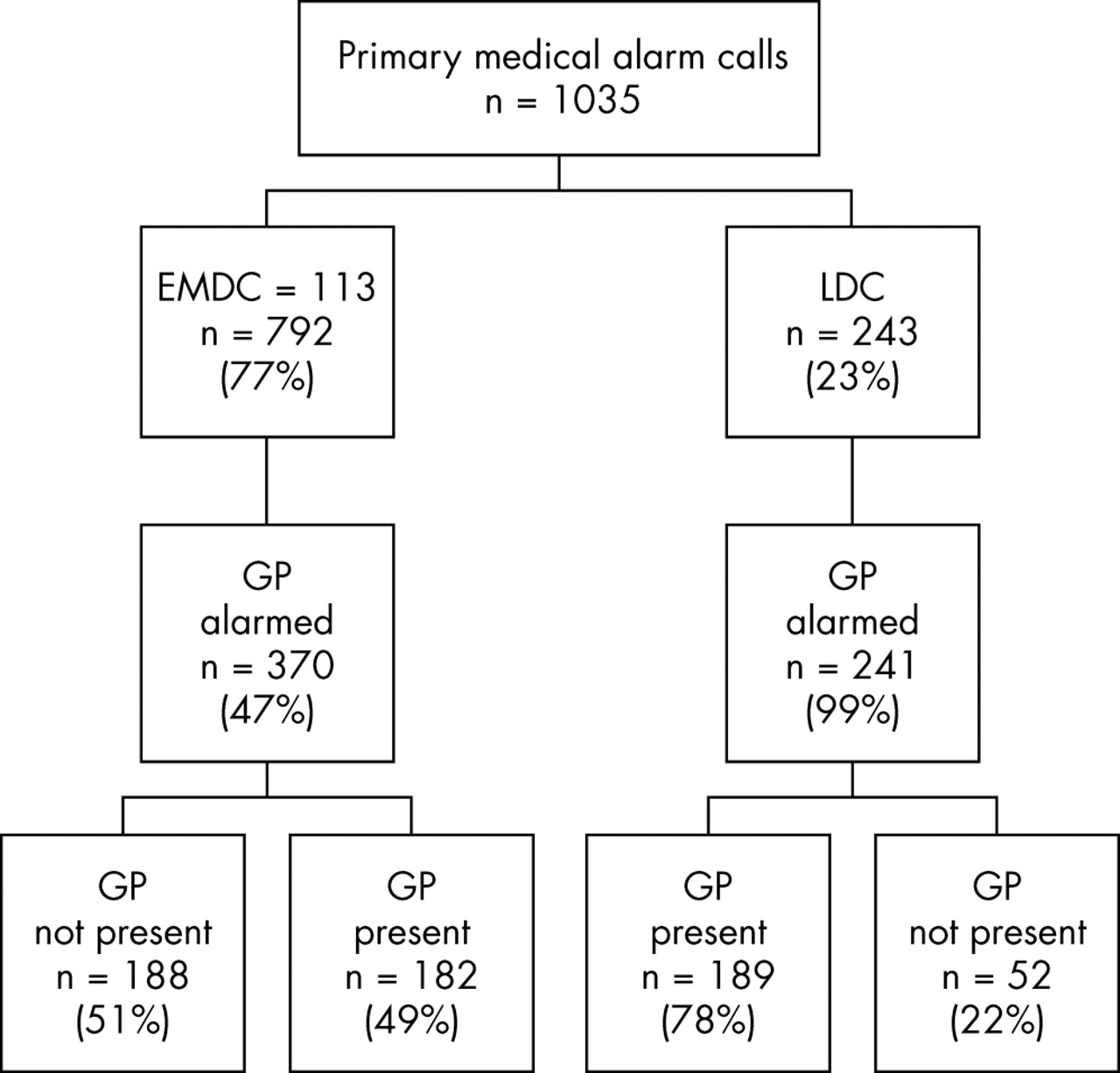
In total, 1035 missions (fig 2) were included, 394 (38%) by helicopter and 641 (62%) by car. The median response time (from alert to arrival at the scene) was 8 minutes by rapid response car (range 1 to 55, interquartile range 7 to 12), and 20 minutes by helicopter (range 4 to 58, interquartile range 15 to 28).

{kind=link}
{kind=link}
Total number of events by the alert mode (via the toll free 113 or through the local dispatch centre (LDC) to the emergency medical dispatch centre (EMDC)), by whether GPs were alerted or not by EMDC, and by whether an alerted GP appeared on scene.
The median age was 52 years (range 0–98, inter-quartile range 27–73), and 65% were men, with no age differences between the sexes. Some 130 missions (13%) involved patients under the age of 16. An NACA score of five or higher, patients with injuries/diseases with acute threat to life or worse, was given in 485 missions (47%).
Public alerts through the toll free 113 number
The use of 113 varied with the distance from Stavanger, the base of the EP manned ambulance. In the geographical groups with more than 15 minutes’ driving time by ground ambulance, the adjusted proportion of calls through 113 were significantly lower than the proportion in Stavanger (table 2). The use of 113 did not differ with severity of illness/trauma as defined by the two NACA subgroups.
Adjusted risk ratio* for the EMS system being alerted of medical emergencies via the dedicated toll free number (113), for GPs being alerted by the dispatch centre, and for alerted GPs (n = 611) being present on scene, according to estimated transportation time to Rogaland Central and University Hospital
Alerting of GPs by the two emergency medical dispatch centres
The frequency of alerting the GP by the EMCDs in “acute” cases increased with increasing distance from Stavanger and was 3–4 times the proportion in Stavanger when adjusted for age, sex, diagnosis, and NACA severity score (table 2).
General practitioners presence on scene
If alerted, a GP was present in 27% of the missions in the city of Stavanger, and the adjusted proportions in the other areas were 2–4 times higher (table 2). The presence of GPs on scene was highest on missions with the highest NACA score (NACA 5–7) in two of the geographical groups; areas with 5–14, and more than 45 minutes’ ambulance driving time from Stavanger (p<0.01 and p = 0.01 respectively).
DISCUSSION
Public alerts routed to the toll free 113
There was significant variation in the public use of the three digit number, 113, in medical emergencies leading to the turnout of an EP manned EMS. In urban Stavanger, hosting the base of the EP manned EMS, 96% of public calls came through 113, compared with only 50% in more remote areas (table 2).
When the emergency medical system was reorganised in Norway, great effort was made to make the new toll free 113 known. Television, radio, and newspapers were used in the information campaign, and emergency information and illustrations of basic life support had an eye catching place in all telephone directories. As only 50% of the emergency calls evaluated to be in need of, and leading to a turnout of the EP manned EMS came through 113 in rural areas, it could be asked if the effort and money spent on this campaign did pay off. In a recent US study9 of a community intervention where one goal was to increase the use of emergency medical services for patients suffering from myocardial infarction, less than 40% of these patients were brought to hospital with ambulances despite a massive information campaign.
The differences we found in use of the toll free 113 probably mirror differences in patterns of communication and interaction between patients and the EMS system in urban and rural areas. Our study was not designed to reveal any delay in response, or any influence on patient outcome due to the differences in routing of the emergency calls.
The emergency medical dispatch centres
According to the Index,6 both GPs and ambulances should be alerted in “acute” cases. This was mostly complied with in rural areas, whereas in Stavanger, GPs were alerted in only 23% of cases (table 2). It seems unlikely that the failure to alert a GP in Stavanger would affect the outcome or reduce the use of resources, as all the patients were within 5 minutes’ transport time of the EP manned EMS. The routine of alerting the GP in the vicinity of the base can be questioned, as having an EP rapidly on scene is shown to save life years.10 For the more remote areas the situation is different, and the GP, if called, is frequently the first physician on the scene.
The observed differences in alerting pattern might therefore be logical, but there is no official political nor professional endorsement of such practice, and as stated above, it does not follow the criteria based dispatch as defined in Rogaland. There seems to be an established practice outside the formal decisions or priority discussions, and without any reflections on differences in quality of care. It appears that the routines have been modified by daily life experiences, but one should note the risk of overconsumption of the specialised EMS.9
GPs on scene
We found a higher frequency of GPs on scene with increasing distance from the base of the EP manned EMS, similar to findings by Hotvedt et al in northern Norway.11 In Stavanger, approximately one quarter of the alerted GPs were present when the EP arrived. In this area, the EP can arrive rapidly, a fact that might influence the decision making of the GP. GPs in rural areas may be more vulnerable to criticism than their city colleagues if they do not show up at medical emergencies, and they may know the patients and their relatives better, and therefore feel a stronger obligation to participate. They may also feel more useful in situations where the EP manned EMS needs time to get to the scene, and where weather conditions may limit the use of this service. The observed variation of GPs present on scene may be a subject for more studies, including the skills and equipment of GPs as parts of the EMS system.
General discussion
There are studies supporting the role of GPs in medical emergency service. In Brussels, GP dispatchers, with a standby GP who can make house calls for non-vital complaints or be of supplementary assistance to the ambulances, reduced the use of ambulances, the frequency of hospitalisation, and also tended to decrease the use of mobile intensive care units.12 This is a function similar to the Norwegian LDCs and GP housecall system, but with the addition of a GP in the dispatch centre. There was no indication in the Belgian study that this compromised the medical assistance to vital emergencies. At the same time, Christensen et al found an anaesthesiologist manned ground ambulance reduced the number of hospitalisations in a Danish urban EMS system.13 It can be speculated that there is an overall health benefit by reducing hospitalisation of patients, and rendering the special medical resources available for those needing them most, whether in rural or urban areas. Somers et al14–17 also support the role of GPs in pre-hospital emergency medicine, but address the need of improving skills needed to deal with emergencies and disasters.
To reveal the direct impact of the EP manned EMS, only calls that lead to activation of this service, approximately 14% of all “acute” calls, were included in this study. Both the EP manned system and the Index are well established in the area, and it seems unlikely that many life threatening emergencies failed to be included.
CONCLUSION
We found significant geographical differences in the emergency medical service in the county of Rogaland. In emergencies leading to a turnout of the EP manned EMS, the toll free 113 phone number for medical emergencies was less used in rural areas, where up to 50% of the calls were initially made to the LDC. General practitioners are more regularly alerted by the EMDCs, and more regularly present on scene in medical emergencies with increasing distance from the base of the EP manned EMS. Obviously, the specialised EMS influences the involvement of GPs in pre-hospital emergencies.
The intention of the reorganising of the emergency medical service in Norway was a service based on equity and equality, independent of the location of the emergency scene, and GPs were thought to be the backbone of the EMS system. This seems to be the fact for rural areas of Rogaland, but in urban areas, the GPs play a more modest role. There seem to be logical reasons for a different organisation and function of the EMS service based on geographical conditions, and access to medical resources. Future organisation of the EMS has to reflect this, preventing unplanned and unwanted autonomously emerging EMS systems. It is of vital importance that GPs in rural areas have the competence and skills needed for handling medical emergencies.
Acknowledgments
The authors want to acknowledge the superior computer software support from B Conneryd, Gotland, Sweden. We deeply appreciate the financial support from The Norwegian College of General Practitioners, and from Rogaland Medical Association.
REFERENCES
Footnotes
-
Competing interests: none declared
Linked Articles
- Prehospital care