Article Text

Abstract
Background: The German cystic fibrosis (CF) quality assurance (CFQA) project is a patient registry for CF which was founded in 1995. Relevant clinical and laboratory data, respiratory function test results, complications, and CF treatments are entered into the database once a year for each patient. Using the database, a study was undertaken to elucidate the relationship between nutrition and lung function in a large patient cohort by cross sectional and longitudinal analysis.
Methods: A cohort of 3298 patients above 2 years of age was analysed. Patients were grouped according to the presence or absence of malnutrition (wasting and/or stunting). Cross sectional and longitudinal analyses over 2 and 3 years including mixed model analyses were performed.
Results: The prevalence of abnormal weight for height (<90% predicted) increased with age from 19% in children aged <6 years to 38% in adults with CF. Patients with malnutrition had significantly lower mean values of vital capacity, arterial oxygen tension (Po2), and forced expiratory volume in 1 second (FEV1) and higher serum IgG (p<0.05). Pseudomonas aeruginosa infection was also associated with decreased pulmonary function. Malnourished adolescents aged 12–18 years experienced a serious decline in FEV1 of about 20% predicted, whereas mean FEV1 values remained stable at above 80% predicted in adolescents of normal weight. Longitudinal follow up showed that malnourished patients of all ages and those with P aeruginosa infection had significantly worse lung function than their normally nourished counterparts and a greater yearly loss of FEV1 % predicted. During 1 year of observation adolescents who experienced a >5% predicted decrease in weight for height had a concomitant mean loss of FEV1 of 16.5% predicted during that year, whereas patients who gained relative weight had a parallel increase in FEV1 of 2.1% predicted.
Conclusions: These data emphasise the close relationship between nutrition, lung function, and clinical course in CF. Normal body weight and absence of P aeruginosa infection was associated with better preservation of lung function.
- cystic fibrosis
- nutrition
- lung function
- children
Statistics from Altmetric.com
Most patients with cystic fibrosis (CF) carry mutations at the CFTR gene which are associated with malfunction of the pancreas. Since malabsorption due to pancreatic insufficiency causes intolerance of nutritional fat, patients are at risk of low energy intake in addition to increased faecal nutrient loss. In the past malnutrition was considered one of the key clinical features of CF. A low fat diet was recommended by most CF centres until the mid 1980s when acid resistant pancreatic enzymes became available. At that time researchers from Toronto had reported that an energy rich diet not restricted in fat, together with additional (conventional) enzyme supplements, resulted in a better nutritional status and longevity of their patients compared with those treated in Boston, a comparably large and experienced centre.1 Seventeen years later, with modified dietary recommendations in the US, substantially smaller differences in the growth indices of patients with CF between the US and Canada were observed.2 Thus, there was evidence that improved nutrition was associated with better long term outcome, as had already been stated in an earlier paper by Kraemer et al.3 A consensus report on nutrition in CF published in 1992 described nutritional management as an important part of the multidisciplinary approach to the disease.4 Nowadays there is no reason to accept nutritional failure or growth retardation in any patient with CF.5
Patient registries for CF permit analysis of data from large cohorts of patients over many years. Results from Canada and the US, the UK, Australia, Europe, and Denmark have shown improved nutritional status, lung function, and survival of CF patients during the last decades.2,6–12 Respiratory function tests, energy expenditure, growth status, and weight were more abnormal with increasing age. Later birth cohorts had improved outcome, and some authors described sex related differences in health. Most of these studies present cross sectional data, however, while the longitudinal course of certain patient groups over years has been addressed in only a few reports.13,14
The relationship between nutritional status and lung function has not been analysed in detail using data from patient registries. The German CF quality assurance project was founded in 1995 and data from more than 5000 patients with CF aged 1 month to 58 years have been documented up to the end of the year 2000. The aim of the present study was to describe the prevalence of malnutrition in these patients and to elucidate the relationship between nutrition and lung function by cross sectional and longitudinal analyses. We speculated that patients with normal weight would be in a better clinical condition than malnourished patients, and that the yearly decline in pulmonary function would be smaller if weight was normal.
METHODS
The German CF quality assurance (CFQA) project is a patient registry which contains relevant clinical and laboratory data, respiratory function test results, and categorised CF treatment and complications.15 Data are entered into the database once a year for each patient. In 1997, clinical data from 3448 patients aged 0–58 years were available from 97 different CF outpatient clinics in Germany. For the present study the cohort of 3298 patients aged above 2 years of age was analysed.
Cross sectional analysis
The 1997 data from all patients were divided into four different age groups: 2–5.9 years, 6–11.9 years, 12–17.9 years, and 18.0 years of age or older, since severity of disease increases with age. According to a publication by Lai and coworkers,16 patients were defined as malnourished if data indicated wasting and/or stunting—that is, if (1) weight was below 90% of the predicted normal value for sex and height in children,17 if body mass index (BMI) was <19 kg/m2 in adults or if (2) weight was <80% of the median normal value for sex and age, or if (3) height was <90% of the median normal value for sex and age.17 Pulmonary function was considered abnormal if (1) forced vital capacity (FVC) was <80% predicted and (2) if forced expiratory volume in 1 second (FEV1) was below 75% of the predicted normal value.18 Mid expiratory flow at 25% of vital capacity (MEF25) was rated abnormal if values were less than 60% predicted. The lower limit of normal for oxygen tension (Po2) in oxygenised capillary blood was 10.7 kPa (80 mm Hg). Serum immunoglobulin G (IgG) values were considered increased if Z scores were ≥2.19 Reference values were used according to recommendations made by the Scientific Advisory Committee of the CFQA project who selected appropriate normal values for the population under consideration. The tabulated reference data for weight were related to a third degree polynomial equation of height. Comparisons between age groups were made for means of nutritional and lung function parameters, and the relative proportion of patients with abnormal results was determined for each age group. In addition, patients were grouped according to the presence or absence of risk factors such as Pseudomonas aeruginosa colonisation or malnutrition.
Multifactorial variance analysis was performed to investigate the association between lung function and malnutrition and the confounders P aeruginosa infection and sex. The Student's t test for independent samples was performed to compare means between groups with normal or abnormal results. χ2 and Fisher's exact tests were used to evaluate proportions of patients.
Longitudinal analysis
Patients who had complete data sets for 1995 and 1996 were eligible for the first part of the longitudinal analysis. 536 children aged 6–11.9 years and 477 adolescents aged 12–17.9 years were analysed in detail. For each patient the differences in weight for height and FEV1 between 1996 and 1995 were calculated.
Three longitudinal groups were defined according to the resulting differences: “better” if the results in 1996 were at least 5% higher than those in 1995: “no change” if the differences were between –5% and +5%; and “worse” if the results were at least 5% lower than in 1995. For each of these groups mean changes in FEV1 and weight for height between the two years were determined. When means from the three longitudinal groups were compared, one way analysis of variance with the Student-Newman-Keuls test was performed. All calculations were made using SPSS (SPSS Inc, Chicago, USA).
In a second longitudinal analysis the equality of FEV1 slopes and intercepts in different risk groups was tested for 1995, 1996, and 1997. Mixed model analysis was performed using SAS Proc Mixed version 6.12 for Windows.20 A multiple comparison adjustment for the p values and confidence limits for the differences of least squares means was performed with a Tukey test. An approximate F test was used to assess the effect of deleting a variable from the model. A level of p=0.05 was used to indicate statistical significance.
RESULTS
Cross sectional data
Clinical and lung function data were available for 3298 patients above 2.0 years of age (table 1). As expected, mean weight for height, vital capacity, FEV1, and Po2 decreased with age, and the proportion of patients with abnormal results was larger in older patients. Mean weight for height was below 90% predicted in 19.0% of children aged 2–6 years and in 31.5% of adolescents. In children below 12 years of age, Po2 had the highest frequency of abnormal results. More than 50% of adolescents had abnormal MEF25, IgG, and Po2, while FEV1 was decreased in only 38.5%. A multifactorial analysis of variance revealed that FEV1 was related to both malnutrition (p<0.001) and P aeruginosa colonisation (p<0.001) but was independent of sex (p>0.05) for all age groups.
Mean clinical data (95% confidence intervals) in 1997 by age group
Pulmonary function was decreased in 56.0% and 85.6% of P aeruginosa positive adolescents and adults, respectively, whereas only 37.4% and 66.3% of non-colonised patients had abnormal lung function (p<0.001, fig 1). An association between P aeruginosa colonisation and malnutrition was also observed. However, most patients had a weight for height above 90% predicted or a body mass index above 19 kg/m2, irrespective of bacterial status.

Frequency of (A) malnutrition and (B) impaired lung function in patients with and without Pseudomonas aeruginosa (PA) colonisation.
Patients with malnutrition had significantly lower vital capacity and FEV1 and higher serum IgG. As shown in table 2, this was independent of P aeruginosa infection. For example, in malnourished children aged 6–11.9 years who were P aeruginosa positive, mean vital capacity and FEV1 were 11.3% and 14.5% predicted lower, respectively, than in normally nourished children (table 2). A similar difference between children of normal and decreased weight was observed in the absence of P aeruginosa colonisation—for example, FEV1 was 11.8% predicted lower. In P aeruginosa positive and negative adolescents, malnutrition was associated with even larger differences in lung function, IgG, and Po2. The differences between normally nourished and malnourished adults with CF were comparable to those in adolescents, and the presence or absence of P aeruginosa had no additional effect.
Mean differences (95% confidence intervals) between malnourished and normally nourished patients by age groups and by Pseudomonas aeruginosa colonisation
Figure 2 shows cross sectional mean values of FEV1 by age and bacterial status. FEV1 values of at least 90% predicted were observed in children and adolescents with normal weight and no P aeruginosa infection. P aeruginosa positive patients with normal weight had mean FEV1 values which were 10–20% predicted lower, but they remained at above 80% predicted except at age 13. In contrast, malnutrition was associated with a severe decline in FEV1 of about 20% predicted between 12 and 18 years of age, irrespective of bacterial status. Malnourished patients colonised with P aeruginosa had the worst results at any age. For example, at ages 8 and 17 mean FEV1 was only 65% and 46% predicted, respectively. These differences between the four groups were both clinically relevant and statistically significant (p<0.001).

Cross sectional mean values of FEV1 grouped by presence or absence of malnutrition and Pseudomonas aeruginosa (PA). The decline in % predicted FEV1 at age 18 years is partly due to different reference values for adults.
Longitudinal analysis
Three patient subgroups were formed with respect to the patients' individual courses from 1995 to 1996. Malnourished adolescents who experienced a decrease of ≥5% predicted in weight for height during that year had a concomitant mean loss in FEV1 of 16.5% predicted, whereas patients who gained relative weight had a parallel increase in FEV1 of 2.1% predicted. These differences were statistically significant (p<0.001). In adolescents with normal weight in 1995, FEV1 declined by 7.6% or 0.16% of predicted if weight decreased by at least 5% or remained stable, respectively, whereas patients who improved their weight by more than 5% had a concomitant increase in FEV1 of 4.3% (p<0.001). Figure 3 shows the respective data for 6–11.9 year old children.

Mean values of individual differences in FEV1 (% predicted) between 1995 and 1996 in 536 schoolchildren aged 6–11.9 years of age. (A) Normally nourished children. (B) Children who were malnourished in 1995 (weight for height (W/H) <90% predicted). If W/H decreased by 5% or more, a concomitant decline in FEV1 of (A) 12.8% and (B) 7.5% predicted was observed.
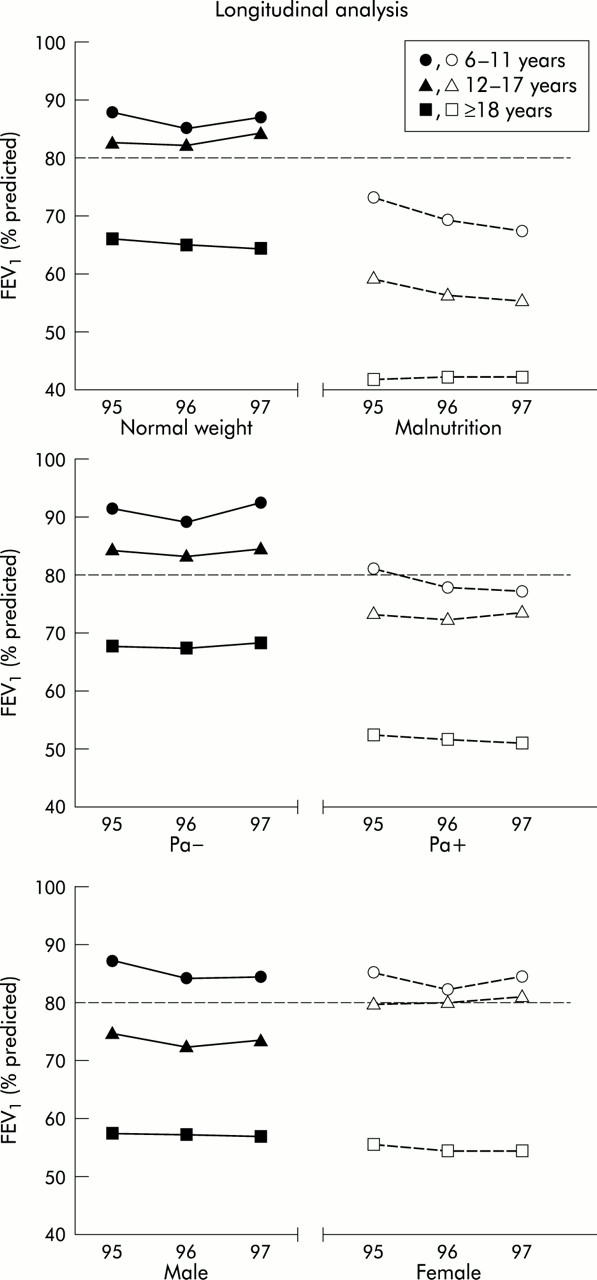
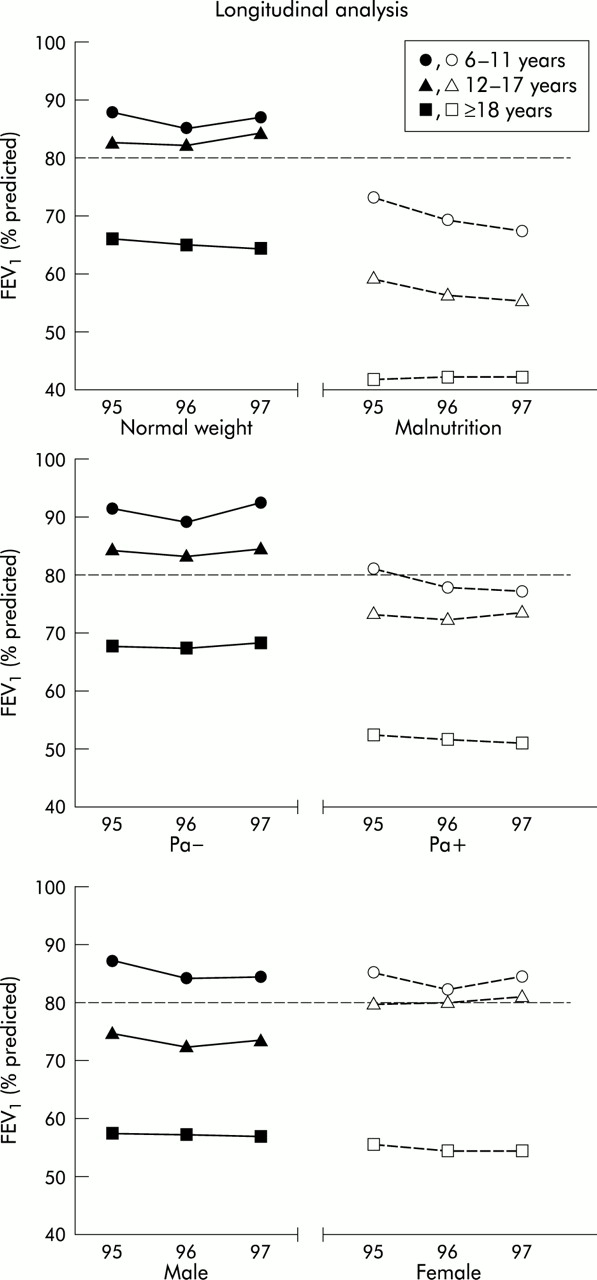
In a further step a mixed model analysis was performed to identify differences between sexes and between risk groups (patients with or without malnutrition or P aeruginosa infection, respectively) with respect to the decline in FEV1 within a year. Malnourished patients of all age groups had significantly worse lung function than their normally nourished counterparts (table 3). At the initial visit in 1995, FEV1 was 11.7–23.9% predicted lower if weight for height was decreased . During the 2 year follow up period, adolescents with malnutrition experienced a decline in FEV1 whereas lung function remained stable in adolescents with normal body weight (p<0.01, fig 4). The FEV1 slopes of patients colonised with P aeruginosa were significantly worse in children and adolescents with a 1.14–2.79% predicted faster decline in lung function (p<0.001). The only association with sex was found in adolescents, with females showing a slower progression of lung disease than males—that is, a 1.58% predicted difference in FEV1 within a year (table 3).
Longitudinal results: mixed model regression estimates for forced expiratory volume in 1 second (FEV1) in 1995 (intercept) and for the mean decline in FEV1 per year (slope)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Mixed model analysis for the course of FEV1 between 1995 and 1997 in the three age groups by risk factors (malnutrition and P aeruginosa (Pa) colonisation) and sex.
DISCUSSION
The negative impact of underweight on the long term outcome of patients with CF has long been recognised.3 The results of the present longitudinal analysis from a large cohort of patients confirm that nutrition and lung function are co-dependent variables in CF. Patients with normal weight had a significantly smaller decrease in lung function over a 2 year period than those with malnutrition, and this was shown in all age groups. A fall in weight for height of 5% predicted or more within 1 year was associated with a parallel decrease in FEV1, whereas patients with improved nutrition showed constant or even improved FEV1.
Cross sectional analysis revealed that the prevalence of malnutrition was 19% in children aged 2–6 years and increased considerably with age up to 38% in adults. Other disease related parameters, particularly Po2 and MEF25, were abnormal in even larger proportions of patients, and showed a similar deterioration with age. Of the 858 adolescents aged 12–18 years, more than one third had abnormal MEF25 (59%), serum IgG (53%), Po2 (50%), FEV1 (42%), and VC (39%). The figures for FEV1 are comparable to data from other patient registries. For example, the US registry found that FEV1 was less than 70% predicted in 68% of adult patients.21 There are no data from other patient registries with respect to IgG, Po2, or MEF25 grouped by age.
In the present study, adolescent girls had better FEV1 results and a smaller yearly decline in FEV1 than boys. Younger children and adults showed no sex related differences by mixed model analysis. Data from the literature concerning the influence of sex on the course of CF are controversial. Zemel et al reported better weight (% predicted) in boys and higher Z scores for length and age in girls.13 In contrast, the growth of boys with CF was impaired on the basis of height, fat free mass, and fat mass when observed longitudinally.14 In the study by Corey et al, male patients had milder disease than females, as reflected by a smaller decline in FEV1, decreased mortality, and higher survival.22 No significant differences between males and females have been found in other studies.11,23–25
Chronic infection with P aeruginosa had a negative impact on pulmonary function, Po2, and IgG. Significantly worse mean FEV1 values were found in malnourished children, adolescents and adults, and the yearly decline in FEV1 was larger in P aeruginosa positive patients. On the other hand, a large proportion of infected patients had normal weight and lung function. A recent report revealed a faster decline in FEV1/FVC and an increased rate of worsening of chest radiographs after colonisation with P aeruginosa.26 Previous studies found that infection with mucoid P aeruginosa was associated with an accelerated rate of decline in pulmonary function.27,28 The CFQA project does not distinguish between mucoid or non-mucoid strains. From the data in the German registry, P aeruginosa infection must be regarded as a significant confounder for pulmonary function impairment in patients with CF.
When patients were stratified according to spirometric results, schoolchildren and adolescents with normal FEV1 had a 4% and 10% predicted better mean weight for height, respectively, than children with impaired respiratory function. Zemel et al analysed patients with FEV1 above or below 90% predicted and described significantly better data for weight and height in the group with normal lung function.13 The North American Epidemiologic Study of Cystic Fibrosis (ESCF) reported that mean weight for age was at the 45th percentile in patients with an FEV1 of ≥100% predicted, whereas the mean weight for age percentile was only 20 if FEV1 was significantly impaired (below 40% of normal).25 Thus, a cross sectional perspective leaves no doubt that children with normal lung function have significantly better weight.
The detailed longitudinal follow up in the present study together with a mixed model analysis adds important information to previously published data. Corey et al22 discussed the advantages of a mixed model analysis—for example, that repeated observations are properly accounted for in significance testing. They described a decline of only 0.7% FEV1 per year in patients with normal pancreatic function compared with a decrease of 3.1% in patients with pancreatic insufficiency. Since patients with pancreatic insufficiency generally have a lower body weight, this is indirect evidence of the influence of nutrition on the longitudinal development of lung function. Wasting has also been shown to be an independent predictor of mortality in a recent paper published in Thorax.29 In the study by Zemel et al which included a four year longitudinal analysis, Z scores for weight for age and height for age were positively associated with FEV1 % predicted.13 We have shown a 1.6% predicted smaller decline in FEV1 in well nourished children and adolescents and a 12% difference in mean FEV1 values between groups with or without malnutrition. When individual patients were categorised by change of weight and lung function within 1 year, those with a decrease in weight for height of ≥5% had a parallel decrease in FEV1 and vice versa, whereas patients with constant or even improved weight experienced no or only an insignificant decrease in FEV1. We cannot tell what the reasons for the changes in weight were since the CFQA project reports treatment by categories only. Clinical trials confirm, however, a parallel improvement in nutritional status and lung disease: intravenous antibiotics for respiratory exacerbations have a positive effect on both lung function and weight,30–32 and inhaled antibiotics not only improve pulmonary function but also the nutritional status of patients.33,34 On the other hand, long term gastrostomy feedings induce favourable outcomes of nutrition as well as of pulmonary function.35
Possible reasons for the influence of malnutrition on chronic lung disease have been discussed in a comprehensive review.36 In chronic obstructive pulmonary disease (COPD) emaciation has long been known to be accompanied by emphysema, and patients with COPD and severe airflow obstruction have lower body weight. Both oxygen consumption of respiratory muscles and resting energy expenditure were increased in patients with COPD. The flattened diaphragm present in emphysema diminishes the efficiency of respiratory muscles, and a myopathic process in malnutrition has also been suggested.37 In animal studies biochemical abnormalities were associated with malnutrition—for example, increased collagen breakdown, impaired lung repair, and decreased surfactant activity. Relatively little information is available on possible pathophysiological processes in CF. In particular, a cause/effect relationship remains to be proven.5 In the malnourished mouse model of respiratory infections in CF, nutritional deficiency contributed to compromised innate lung defences, bacterial colonisation, and excessive inflammation in the CF respiratory tract.38 A recent review summarised clinical studies on the relationship between lung function and nutritional status.39 Correlations were found between FEV1 and lean body mass, the body compartment which includes skeletal muscle, suggesting an influence of muscle wasting on pulmonary function. The detrimental effect of malnutrition on immune function in general40 must also be considered as a relevant mechanism in CF. Treatment with intravenous antibiotics was associated with a concomitant decline in inflammatory parameters (C reactive protein, tumour necrosis factor-α), energy expenditure, and an increase in body weight.32,41
In summary, the results of this study suggest that normal body weight is associated with better lung function in CF. A significantly smaller decline in FEV1 can be expected in all age groups if patients are well nourished, and this is independent of a concomitant colonisation with P aeruginosa.
Acknowledgments
The authors thank the Scientific Advisory Board of the German CFQA project (Chairman: Professor Dr Martin Stern) for permission to analyse data from the registry, and acknowledge the large amount of work by staff from the 97 CF centres who reported patient data to the project (available on website www.thoraxjnl.com).
REFERENCES
Supplementary materials
Acknowledgements
The authors thank the Scientific Advisory Board of the German CFQA project (Chairman: Professor Dr Martin Stern) for the permission to analyse data from the registry, and acknowledge the large amount of work by staff from the 97 CF centres who reported patient data to the project:
Aachen, Kinderarztpraxis; Aue, Klinikum Aue, Kinderklinik; Augsburg, Kinderkrankenhaus Josefinum; Bad Saarow, Humaine Klinikum Bad Saarow, Klinik f�r Kinderheilkunde; Berlin, Krankenhaus Lichtenberg, Kinderklinik Lindenhof; Berlin, Krankenhaus Zehlendorf, Lungenklinik Heckeshorn, Kinderambulanz; Berlin, Kreiskrankenhaus Nauen, Betriebsst�tte Staaken; Berlin, Krankenhaus Buch von Berlin-Pankow, "C W Hufeland"; Bochum, Ruhr-Universit�t Bochum, Klinik f�r Kinder- und Jugendmedizin; Bodenheim, Praxis f�r P�diatrie und Allergologie; Bonn, Universit�t Bonn, Zentrum f�r Kinderheilkunde; Borkum, Reha-Klinik Borkum Riff; Brandenburg, St�dt. Klinikum Brandenburg GmbH, Kinderklinik; Bremen, Zentralkrankenhaus St.-J�rgen-Stra�e, Prof. Hess - Kinderklinik; Bremen, Krankenhaus "Links der Weser", Kinderklinik; Chemnitz, Kinderarztpraxis; Coswig, Fachkrankenhaus Coswig, Zentrum f�r Pneumologie u. Thoraxchirurgie; Cottbus, Carl-Thiem-Klinikum Cottbus, Klinik f�r Kinder- und Jugendmedizin; Datteln, Vestische Kinderklinik Datteln; Dresden, Carl-Gustav-Carus-Klinikum, TU Dresden; D�sseldorf, Kinderklinik, Schlo�mannshaus; Erfurt, Klinikum Erfurt GmbH, Klinik f�r Kinderheilkunde, Poliklinik; Erlangen, Fr.-Alexander-Universit�t Erlangen-N�rnberg, Klinik f. Kinder u. Jugendliche; Essen, Ruhrlandklinik Essen, Zentrum f�r Pneumologie u. Thoraxchirurgie; Essen, Universit�tsklinikum Essen, Klinik f�r Kinder- u. Jugendmedizin; Esslingen, St�dtische Kliniken Esslingen/Neckar, Klinik f�r Kinder u. Jugendliche; Frankfurt, Klinikum der J. W. v. Goethe-Universit�t, Schwerpunkt Pneumologie; Frankfurt, Klinikum der J. W. v. Goethe-Universit�t, Klinik f�r Kinderheilkunde; Frankfurt/Oder, Klinikum Frankfurt/Oder, Klinik f�r Kinder- u. Jugendmedizin; Frechen, Kinderarztpraxis; Freiburg, Universit�ts-Kinderklinik der Albert-Ludwigs-Universit�t Freiburg; Gie�en, Universit�ts-Kinderklinik, Bereich Pneumologie u. Allergologie; G�ttingen, Georg-August-Universit�t, Kinder-/Poliklinik; Greifenstein, Pneumologische Klinik, Waldhof-Elgershausen; Greifswald, Ernst-Moritz-Arndt-Universit�t, Klinik f. Kinder- u. Jugendmedizin; Hagen, Allgemeines Krankenhaus, Kinderklinik; Halle (Saale), Martin-Luther-Universit�t, Klinikum Kr�llwitz, Klinik f�r Kinderheilkunde; Hamburg, Gemeinschaftspraxis, CF-Zentrum Altona; Hamburg, Praxis; Hamburg, Universit�ts-Kinderklinik, Eppendorf; Hannover, Medizinische Hochschule Hannover, Abt. Pneumologie; Hannover, Kinderklinik der MHH, Abt. P�d. Pneumologie; Heidelberg, Klinikum der Universit�t, Kinderklinik, Abt. Pneumologie; Heidelberg/Rohrbach, Thoraxklinik der LVA Baden, Abt. Innere Medizin - Pneumologie; Heilbronn, Kinderklinik Heilbronn; Homburg/Saar, Universit�tsklinik f�r Kinder- u. Jugendmedizin, P�d. Gastroenterologie; Jena, Klinikum der Friedr.-Schiller-Universit�t, Klinik f. Kinder- u. Jugendmedizin; Karlsruhe, St�dtisches Klinikum Karlsruhe, Kinderklinik; Karlsruhe, Kinderarztpraxis; Karlsruhe, Kinderarztpraxis; Karlsruhe, Kinderarztpraxis; Kassel, Kinderkrankenhaus, Park Sch�nfeld; Kiel, Klinik der Christian-Albrechts-Universit�t, Klinik f�r allgemeine P�diatrie; Kirchzarten, Kinderarztpraxis; K�ln, Kinderkrankenhaus K�ln Riehl, Neonatol. U. p�diatr. Intensivstation E2; K�ln, Universit�ts-Kinderklinik K�ln, P�d. Pneumologie u. Allergologie; Krefeld, St�dt. Krankenanstalten, Kinderklinik; Leipzig, Universit�tskinderklinik Leipzig, Abt. f�r ambulante und soziale P�diatrie; L�beck, Medizinische Universit�t L�beck, Klinik f�r P�diatrie; Ludwigshafen a. RH, St. Marien- und St. Annastiftskrankenhaus, Kinderklinik; Magdeburg, Otto v. Guericke-Universit�t, Abt. Pulmonologie u. Intensivmedizin; Magdeburg, Otto v. Guericke-Universit�t, Med. Fakult�t, Zentrum f�r Kinderheilkunde; Mechernich, Kreiskrankenhaus Mechernich, Klinik f�r Kinder- und Jugendmedizin; M�nchen, Poliklinik-Kinderpoliklinik, Klinikum Innenstadt der LMU; M�nchen, Dr. von Haunersches Kinderspital der Universit�t M�nchen; M�nchen, Kinderklinik der TU, M�nchen-Schwabing; M�nchen, Medizinische Klinik, Klinikum Innenstadt der LMU; M�nster, Clemenshospital GmbH, Klinik f�r Kinder- und Jugendmedizin; Neubrandenburg, Klinikum Neubrandenburg, Kinderklinik; Neuruppin, Ruppiner Krankenhaus, Kinderklinik; Neuwied, St.-Elisabeth Krankenhaus, Kinderabteilung; Offenburg, Kreiskrankenhaus Offenburg, Kinderklinik; Oldenburg, Kinderklinik Oldenburg; Osnabr�ck, Marienhospital Osnabr�ck, Klinik f. Kinderheilkunde u. Jugendmedizin; Osnabr�ck, Kinderhospital Osnabr�ck; Pforzheim, St�dtisches Klinikum Pforzheim, Kinderklinik; Plauen, Vogtland-Klinikum Plauen, Kinderklinik; Potsdam, Klinikum Ernst v. Bergmann, Kinderklinik; Ravensburg, Kinderkrankenhaus, St. Nikolaus; Regensburg, Klinik St. Hedwig, Kinderkardiologie - Neonatologie; Rostock, Universit�t Rostock, Med. Fakult�t, Kinder- und Jugendklinik; Saalfeld, Th�ringen-Klinik, Kinderabteilung, Georgius Agricola; Saarbr�cken, Pneumologische Praxis; Schwarzenberg, Facharztpraxis Kinderheilkunde; Schwerin, Klinikum Schwerin, Kinderklinik; Siegen, DRK-Kinderklinik Siegen, P�diatrie; St. Augustin, Johanniter-Kinderklinik, f�r den Rhein-Sieg-Kreis; Stuttgart, Olgahospital - Kinderklinik, P�diatrisches Zentrum; Suhl, Pneumologische Praxis; Trier, Mutterhaus der Borrom�erinnen, P�diatrische Abteilung; T�bingen, Universit�ts-Kinderklinik, Poliklinik; Ulm, Universit�tskinderklinik, P�d. Gastroenterologie, Pulmologie, Allergologie; Vechta, St�dt. Marienhospital, Kinderabteilung; Wangen, Fachklinik Wangen GmbH, Medizinische Klinik f. Atemwegserkrankungen; Wilhelmshaven, Reinhard-Nieter-Krankenhaus, Kinderklinik; W�rzburg, Poliklinik der Universit�ts-Kinderklinik; Zwickau, St�dtisches Klinikum "Heinrich Braun", Klinik f. Kinder- u. Jugendmedizin