Article Text

Abstract
Background Non-adherence to medications continues to be a burden worldwide, with significant negative consequences. Community pharmacist interventions seem to be effective at improving medication adherence. However, more evidence is needed regarding their impact on disease-specific outcomes. The aim was to evaluate the impact of a community pharmacist-led adherence management intervention on adherence and clinical outcomes in patients with hypertension, asthma and chronic obstructive pulmonary disease (COPD).
Methods A 6-month cluster randomised controlled trial was conducted in Spanish community pharmacies. Patients suffering from hypertension, asthma and COPD were recruited. Patients in the intervention group received a medication adherence management intervention and the control group received usual care. The intervention was based on theoretical frameworks for changing patient behaviour. Medication adherence, disease-specific outcomes (Asthma Control Questionnaire (ACQ) scores, Clinical COPD Questionnaire (CCQ) scores and blood pressure levels) and disease control were evaluated. A multilevel regression model was used to analyse the data.
Results Ninety-eight pharmacies and 1186 patients were recruited, with 1038 patients completing the study. Patients receiving the intervention had an OR of 5.12 (95% CI 3.20 to 8.20, p<0.05) of being adherent after the 6 months. At the end of the study, patients in the intervention group had lower diastolic blood pressure levels (mean difference (MD) −2.88, 95% CI −5.33 to −0.43, p=0.02), lower CCQ scores (MD −0.50, 95% CI −0.82 to −0.18, p<0.05) and lower ACQ scores (MD −0.28, 95% CI −0.56 to 0.00, p<0.05) when compared with the control group.
Conclusions A community pharmacist-led medication adherence intervention was effective at improving medication adherence and clinical outcomes in patients suffering from hypertension, asthma and COPD. Future research should explore the implementation of these interventions in routine practice.
Trial registration number ACTRN12618000410257.
- chronic disease management
- pharmacists
- compliance
- healthcare quality improvement
- health services research
Data availability statement
Data are available upon reasonable request to the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- chronic disease management
- pharmacists
- compliance
- healthcare quality improvement
- health services research
Introduction
Patients with chronic conditions rely on medications to treat and control their diseases.1 However, medication adherence (ie, the process by which patients take their medications as prescribed) is suboptimal.2 Medication adherence is composed of initiation, implementation and discontinuation.3 4 There is evidence that nearly 40% of patients with chronic conditions discontinue their medication after 1 year and 4% never initiate their treatment.5 Similarly, implementation of the dosing regimen (ie, the extent to which a patient’s actual dosing corresponds to the prescribed dosing regimen) has been shown to decline over time.6 This complex phenomenon is a preventable7 source of patient harm and poor health outcomes. It often leads to disease progression, lower quality of life, increased use of healthcare resources8 and increased morbidity and mortality.9 10 It accounts for an estimated 125 000 deaths per year in the USA,11 with annual costs per patient ranging from $949 to $44 190 (US$2015).12 This problem is especially relevant in chronic conditions such as hypertension, asthma and chronic obstructive pulmonary disease (COPD), three of the most prevalent non-communicable diseases in developed countries, whose prevalence continues to increase.13–15 Medication non-adherence rates in these conditions are high, reaching 50% for antihypertensive medications5 and between 20% and 80% for inhaled medications,16 17 with 14%–20% patients failing to fill in their first prescription.18
Medication adherence interventions have the potential to improve clinical outcomes, patient’s health-related quality of life19 20 and the efficiency of the healthcare system.21–23 Long-term multicomponent interventions involving behavioural change theories seem promising at improving adherence,24–26 probably because they target multiple determinants.27 However, previous research has reported a lack of convincing evidence regarding the efficacy of these interventions, mainly due to the wide heterogeneity in settings, participants, intervention types or adherence measures among others. Moreover, there seems to be a paucity of randomised controlled trials reporting an improvement in both adherence and clinical outcomes,28 despite ethical standards for adherence research dictating that attempts to improve adherence should be judged by their clinical benefits.28 In this regard, some evidence suggests that community pharmacist-led interventions may enhance both medication adherence29–32 and disease-specific clinical outcomes.33 34 However, these usually involve interventions that would be difficult to implement in usual care settings. The development of effective interventions that are implementable in routine practice settings still represents a challenge for quality improvement in patient care.35
Quality use of medicines is often included as a key objective in many national medicine policies, through the implementation of initiatives aiming at ensuring medicines are safely and effectively used. This usually includes mechanisms to monitor and manage medication adherence, which constitutes one of the overarching goals to improve healthcare quality and patient safety.36 In Spain, adherence management is one of the six professional services with national priority following a consensus among Spanish national professional pharmacy organisations.37 However, there is a lack of evidence on the effectiveness of a medication adherence intervention that can be further implemented into regular practice.
The objective of this study was to evaluate the effectiveness of a community pharmacist-led medication adherence management intervention for adult patients being treated with hypertension, asthma or COPD medications on medication adherence and clinical outcomes compared with usual care.
Methods
This study has been reported following the Consolidated Standards of Reporting Trials guidelines for cluster trials.38
Study design
A cluster randomised controlled trial was undertaken in community pharmacies across six Spanish provinces (A Coruña, Albacete, Ciudad Real, Guadalajara, Soria and Tenerife), representing about 12% of the provinces and 7% of community pharmacies in Spain.39 Pharmacies were the unit of randomisation to minimise cross-contamination between study groups. A study protocol has been registered and approved by the Spanish Medication Agency (Agencia Española de Medicamentos, 4DZRC79213). No incentives were provided to pharmacists or patients.
Pharmacy recruitment
An invitation letter to enrol in the study was sent to all the pharmacies in each province by the local pharmacy professional body. The inclusion criteria for pharmacies were: availability of a counselling area; availability of at least one pharmacist to provide the intervention; and the attendance of all pharmacists to an initial training session before the beginning of the study. Inclusion criteria were verified by the local pharmacy professional bodies and by members of the research team. Due to the nature of the intervention, cluster randomisation was used to minimise cross-contamination between study groups. Eligible pharmacies were the unit of randomisation. They were assigned by an independent researcher after they agreed to participate in the study to either an intervention group (IG) or control group (CG) using a computer-generated list of random numbers with ratio 1:1.
Sample size calculation/sampling
Sample size calculations were based on the difference of expected proportions between adherent patients in CG and IG at the end of the study. An absolute difference of 20% in the prevalence of adherent patients between both groups was considered of clinical relevance.40 41 A two-tailed comparison test was applied, considering an 80% power, alpha=0.05 and assuming a 50% prevalence of non-adherent patients at baseline.
The sample size was increased to take into account the design effect (DEFF), calculated as: DEFF=1+[nc−1]*ICC (intraclass correlation coefficient) (where nc=7, average size of the cluster estimated for 102 clusters; ICC=0.05), resulting in 1025 patients. This number was increased to account for a potential 20% loss to follow-up. Therefore, 1230 patients and 102 pharmacies were estimated to be required. Each pharmacy was required to recruit 12 patients: 4 suffering from hypertension, 4 from asthma and 4 from COPD.
Patient recruitment
Patients were recruited consecutively in the participant community pharmacies for 2 months. Filling a prescription (for new or/and existing prescribed medications) was the prompt for the pharmacist to initiate a conversation about the study with potential eligible patients. Patients’ inclusion criteria were: 18 years or older; signature of the informed consent; ability to complete EuroQol-5D,42 Morisky-Green-Levine Medication Adherence Questionnaire (MGL MAQ),43 44 Asthma Control Questionnaire (ACQ)45 or Clinical COPD Questionnaire (CCQ)46; and to have a prescribed medication for hypertension (ie, medications included in the Anatomical Therapeutic Chemical (ATC) classification system groups C02, C03, C07, C08 or C09), asthma or COPD (ATC group R03). Medication groups were defined as per the ATC classification system developed by the WHO.47 Hypertension, asthma and COPD were the target conditions due to their high prevalence and non-adherence rates.13–15 If patients suffered from more than one of those diseases, data were only collected for one condition. This was selected by the pharmacist on the basis of the number of patients to be recruited per disease. Patients were excluded if they: were collecting someone else’s medication; were pregnant or lactating; could not attend the pharmacy on a regular basis; had previously participated in any adherence education programme or study; had communication limitations or any other impairment the recruiting pharmacist considered as precluding them from participating in the study. During recruitment, the pharmacist explained the general characteristics of the study (ie, study involving monthly visits to the pharmacy, in which patients had to respond to the pharmacist’s questions about their medications and health), assessed the patient’s willingness to participate and their eligibility criteria. Patients were blinded to the study design, group and hypotheses. Patients willing to participate received an information sheet and their signed informed consent was obtained. Subsequently, the pharmacist and the patient agreed on a date for the initial and subsequent visits.
Patients attended six face-to-face monthly visits, undertaken in the pharmacy’s counselling area. Patients allocated to the IG received a protocolised medication adherence management intervention (figure 1) whereas patients in the CG received usual care (defined as the supply of medicines and medication-taking advice). In each visit, patients’ data were collected and clinical variables recorded.

Adherence management intervention overview.
Intervention group
Patients in the IG received the medication adherence management intervention. It involved the provision of a complex intervention,48 based on behaviour change frameworks, aiming at identifying and addressing barriers for medication adherence through tailored strategies. The intervention included:
Pharmacist interview to assess adherence to medications for asthma, COPD or hypertension using the MGL MAQ.43 44
Classification of patients as non-adherent (non-intentional, intentional or combined) or adherent.
Identification of barriers for medication adherence. Barriers could be practical, defined as gaps in knowledge or skills; or perceptual, namely those associated with the patient’s health beliefs and perceptions about the condition and their medications.
Intervention proposal using strategies tailored to the type of non-adherence and identified barriers (online supplemental appendix 1).
Application of the transtheoretical model of behavioural change49 by which the pharmacist elicited the patient’s readiness to change while discussing the proposed strategies.50
Follow-up through monthly scheduled visits to review patient progress and provide feedback or new strategies to improve or maintain adherence.
Application of motivational interviewing principles and skills26 51 during the patient–pharmacist interaction.
Supplemental material
Pharmacist training
Group and individualised training sessions were provided by the research team and by practice change facilitators (PCFs, external pharmacists who solved any problems or queries during the study through monthly visits and ensured compliance with the study protocol). Pharmacists in the IG received an initial training which covered the following topics: study protocol, management of the targeted conditions, frameworks for changing patient behaviour and educational skills to provide the intervention, over a 2-day session. Pharmacists in the CG were only trained in data collection and study procedures.
Study outcomes
Medication adherence (appropriate implementation of the dosing regimen) was the primary outcome, assessed by the MGL MAQ43 44 and reported as the percentage of adherent patients. Secondary outcomes included asthma control, COPD clinical health status and hypertension control. Asthma control was assessed using the ACQ-5.45 Results were reported as mean ACQ scores (scale 0–6, with lower scores indicating a better clinical control) and as the percentage of controlled patients (ACQ ≤0.75). A difference of ≥0.5 in mean scores was considered clinically significant.52 COPD clinical health status was assessed using the CCQ.46 Results were reported as mean CCQ scores (scale 0–6, with lower scores indicating a better clinical control) and as the percentage of patients with low clinical impact of the disease (scores <1.0).53 A difference ≥0.4 between mean scores was considered clinically significant.54 In COPD, ‘disease control’ is not achieved, as normalisation of pulmonary function is not possible and patients may continue with exacerbations or limitations during daily life activities regardless of receiving treatment.55 Hypertension control was assessed through systolic blood pressure (SBP) and diastolic blood pressure (DBP) levels using a Visomat (Roche) (two measures, 3 min interval). Proportion of controlled patients (values <140 mm Hg/90 mm Hg)56 and mean blood pressure (BP) levels were reported. All outcomes were measured in all study visits.
EuroQol data were collected in order to assess the cost-utility of the service. Results will be reported elsewhere.
Blinding
Patients were blinded to the intervention but given the nature of the intervention pharmacists were not. Only pharmacists in the IG were trained in the skills and knowledge required to deliver the intervention.
Data collection and quality
Study data were collected in an electronic data collection form, accessible by individual pharmacists through a personal username and password. Pharmacists directly recorded patient demographic data and observer-reported outcomes not involving judgement (ie, BP levels). Patient-reported outcomes (ie, medication adherence, ACQ scores and CCQ scores) were directly collected from patients. They completed the questionnaires in the electronic data collection form, requesting assistance from the pharmacist if needed.
PCFs monitored the quality of data entry and had their own access to the electronic data collection form to ensure data were being collected according to the protocol instructions.57 Patient data were protected and exported as dissociated for the statistical analysis. Only deidentified data from patients, pharmacists and pharmacies were available to the study researchers.
Statistical analysis
Data were analysed using the software package SPSS statistics (V.25.0, SPSS) and SAS/STAT V.9.4 (SAS Institute). Baseline patient-level information was summarised by treatment arm. A multilevel regression model with three levels (pharmacies, patients, visits) was conducted. It included a random intercept to account for the clustering by pharmacy and a correlation structure for the visits within patients, that accounted for changes in correlation of measurements over time (Toeplitz). A logistic regression model was used with this structure to estimate the ORs for the binary outcomes, and a similar linear mixed model was used for continuous outcomes. A likelihood ratio p value (for the overall effect of the variable across visits) and a Wald p value for the test of treatment at each time point were estimated. Estimated rates with lower and upper levels were calculated. All patients with data collected from at least two time points during the study were included in the analysis. Estimated population margins were used to estimate the percentage of patients for binary outcomes and the average value for continuous outcomes by treatment and time period. Linear and generalised linear mixed models for the study outcomes were used, allowing for the assumption of ‘missing-at-random’ (ie, missing contingent on values included in the regression model) without requiring imputation for the missing outcomes (online supplemental appendix 2).
Results
A total of 98 pharmacies and 138 pharmacists were recruited. Four pharmacies and four pharmacists dropped out from the study before starting patient recruitment and two pharmacies and three pharmacists dropped out during the study (n=4 IG, n=2 CG). Patient recruitment was undertaken by pharmacists between October and November 2017, with 1186 patients enrolled (asthma: 385, COPD: 299, hypertension: 502) and 1038 patients (asthma: 333, COPD: 249, hypertension: 456) completing the study (87.5%). Two hundred and eighteen patients were ineligible due to exclusion criteria (figure 2). Baseline patient characteristics are described in table 1.
Baseline characteristics of study patients

Flow chart of study participants. *Two hundred and eighteen patients were ineligible due to exclusion criteria: collecting someone else’s medication (83), were pregnant or lactating (10), could not attend to the pharmacy on a regular basis (75), had previously participated in any adherence education programme or study (19), had communication limitations or any other impairment the recruiting pharmacist considered as precluding them from participating in the study (31). **The difference of eight recruited pharmacies is due to pharmacies that had previously participated in the 2-month pilot study and wanted to continue but could not be allocated to the control group. Therefore, they were allocated to the intervention group.
Medication adherence
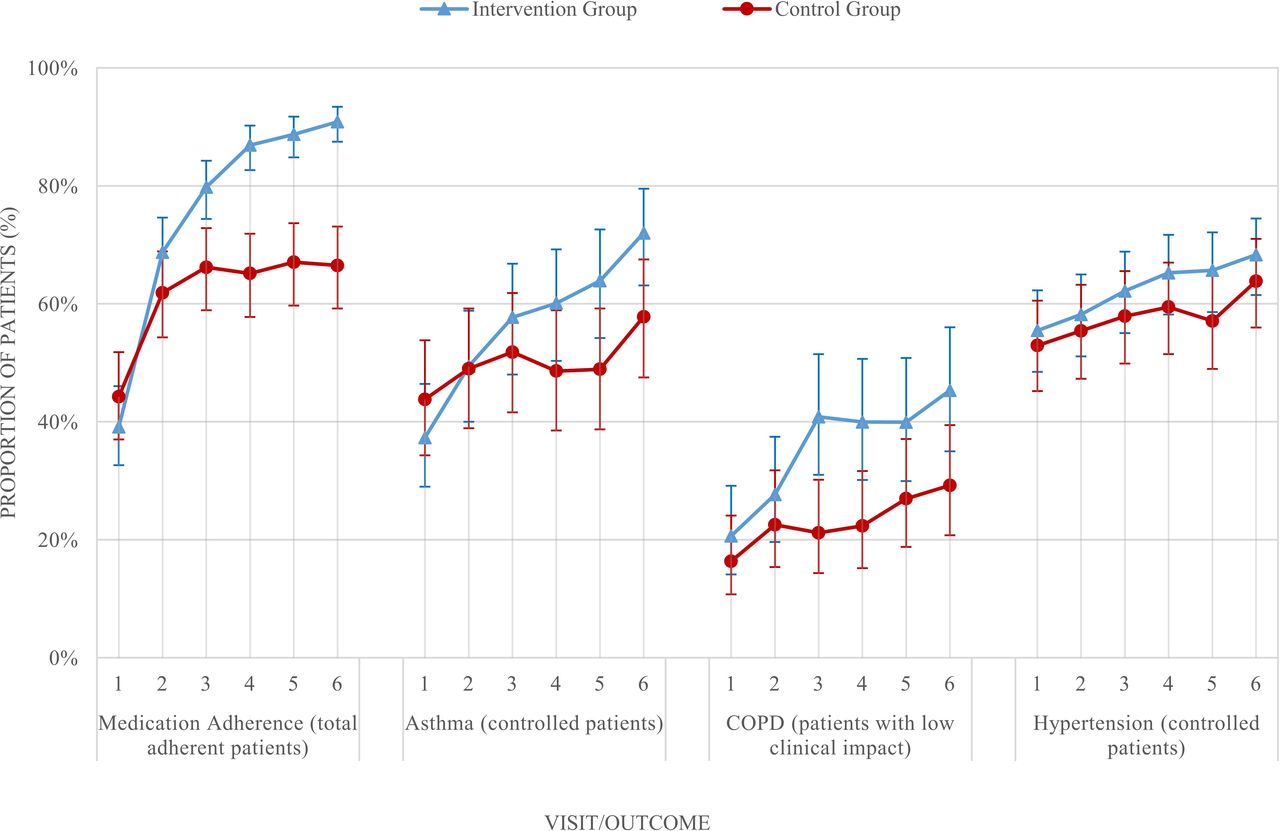
At baseline, the percentages of adherent patients were 39.1% (IG) and 44.3% (CG). For individual follow-up periods, significant differences between study groups were observed from visit 3 (p<0.05) to visit 6 (OR 5.12, 95% CI 3.20 to 8.20, p<0.05) (online supplemental appendix 3, figure 3). Overall, the absolute increase in the percentage of adherent patients during the study was higher in the IG (51.8%) than in the CG (22.2%) (p<0.05). Disease-specific results are reported in the online supplemental appendix 4.
Clinical control
Hypertension
Mean baseline BP levels were similar in both study groups. Mean difference (MD) DBP between IG and CG became statistically significant after visit 5 (p<0.05). At the end of the study, there was a significant reduction in mean DBP in the IG when compared to the CG (MD −2.88, 95% CI −5.33 to −0.43, p=0.02). Changes on SBP were not statistically significant (MD −1.10, 95% CI −4.49 to 2.29, p=0.53) (online supplemental appendix 3). Mean baseline percentages of controlled patients were similar in both groups (IG=55.5%, CG=52.9%). These percentages increased in both groups, with no difference between groups at the end of the study (OR 1.22, 95% CI 0.78 to 1.91, p=0.38) (online supplemental appendix 3, figure 3).
Asthma
Mean baseline ACQ scores were similar in the IG and CG (p=0.98). A gradual decrease was observed in both groups until reaching significant differences in visit 5, favouring the IG (p<0.05). Mean scores decreased 0.53 (IG) and 0.26 points (CG) between baseline and visit 6. Only the diminution in the IG was clinically significant. At visit 6, mean ACQ scores were significantly lower in the IG (MD −0.28, 95% CI −0.56 to 0.00, p<0.05), indicating a better asthma control (online supplemental appendix 3). Percentages of controlled patients at baseline were similar (IG: 37.3%; CG: 43.8%). Statistically significant differences were evident after visit 5. Percentages of controlled patients at the end of the study were significantly higher in the IG (72.0%) when compared with the CG (57.8%) (OR 1.88, 95% CI 1.05 to 3.36, p=0.03) (online supplemental appendix 3) (figure 3).
{kind=link}
{kind=link}
{kind=link}
Categorical outcomes per study group and study visit. COPD, chronic obstructive pulmonary disease.
Chronic obstructive pulmonary disease
Mean baseline CCQ scores were 1.79 (IG) and 2.10 (CG) (p<0.05). Mean scores decreased in both groups across study visits, with significant differences being evident after visit 3 (p<0.05) (MD at visit 6 −0.50, 95% CI −0.82 to 0.18, p<0.05) (online supplemental appendix 3). A reduction of 0.39 (CG) and 0.58 (IG) points in the mean scores was observed at the end of the 6-month period, with the latter being clinically significant. At baseline, percentages of patients with low clinical impact of the disease (ie, low level of symptoms) were 20.6% (IG) and 16.3% (CG) at baseline (figure 3). These percentages increased across study visits in both groups, with significant differences favouring the IG after visit 3 (p<0.05). At the end of the study, the percentage of patients with low clinical impact of COPD was significantly larger in the IG (OR 2.01, 95% CI 1.07 to 3.75, p<0.05) (online supplemental appendix 3).
Discussion
A community pharmacist-led medication adherence management intervention resulted in improvements in medication adherence and clinical outcomes. Significant increases in the percentage of patients adhering to their dosing regimen and improvements in COPD outcomes were evident after 3 months of follow-up. In the case of asthma outcomes and DBP significant improvements were observed after 5 months.
The observed baseline percentage of adherent patients, close to 50%, aligned with the figures previously reported by the WHO.58 Interestingly, there was a gradual increase in these percentages, reaching statistically significant differences between study groups at visit 3. The percentage of adherent patients in the CG was found to remain constant during the following visits, always below 70%. In the IG, this percentage progressively increased during all study visits. At the end of the study, 90% of patients were adherent to their medications, doubling the baseline percentage in the IG and being nearly 25% more than in the CG. Previous studies assessing the effectiveness of pharmacists’ interventions using a similar follow-up period have found between 10% and 40% increase in the percentage of adherent patients.17 59 60 One study targeted patients using new prescribed medications and found a 10% increase in the percentage of adherent patients after 10 weeks of follow-up, but decreased after 26 weeks.61 This study consisted of one initial consultation and one follow-up consultation 5 weeks later.61 Our study resulted in a larger increase (51.8%), probably due to the core components of the brief complex intervention, continuous follow-up and fidelity monitoring of the intervention provision.
These results highlight the importance of continuous follow-up in medication adherence management. Evidence supports that interventions provided on a regular basis are more likely to increase adherence than a single intervention, signalling adherence management interventions are to be maintained as long as the treatment is needed.28 Similarly, interventions delivered across multiple visits are more effective than those delivered during a single visit.62 Our results align with these findings, suggesting adherence interventions should be delivered for at least 3 months to be effective.
There is evidence in the literature indicating that pharmacist-led interventions improve medication adherence in patients with asthma, COPD and hypertension.32 63 However, limited information exists regarding the description of effective interventions, making it difficult to replicate these in real practice. There has been a call to generate more evidence on the impact of these interventions on disease-specific clinical outcomes.28 Due to the negative impact medication non-adherence has on the patient’s outcomes, adherence management has been considered a key element in the development of quality improvement initiatives.35 Moreover, monitoring patient outcomes and medication management skills are essential when delivering interventions aiming at improving quality and safe medicines use.64
Core components of the intervention were based on evidence-based behaviour change frameworks to tailor specific patient needs and elicit medication adherence improvement. Including cognitive-based behaviour techniques resulted in adherence improvements.65 A recent meta-analysis stated the importance of cognitive and behavioural components to effectively change adherence behaviour.25 However, there is no evidence supporting that a single theory should be used.66 We considered a range of strategies tailored to each patient’s individual needs, including educational components or reminders, as they have shown to be effective in chronic conditions,67 68 such as hypertension.69 Our findings align with previous studies, which have shown increases in medication adherence and decreases in BP levels.41 60 70 71 Although our intervention resulted in a larger increase in the proportion of controlled patients in the IG (12.8%) when compared with the CG, differences between study groups were not statistically significant at the end of the study. This could be due to the low mean baseline BP levels of included patients and to uncontrolled hypertension not being a patient inclusion criterion. Additionally, BP changes may also take longer to manifest, as differences in DBP levels started to be significant after 5 months of follow-up. Consistent with other studies that reported reductions of 3–11 mm Hg (DBP) and 7–30 mm Hg (SBP),41 60 71–74 our study reported a reduction of 3.3 mm Hg in SBP and 2.5 mm Hg in DBP levels. Non-adherence has been associated with a high DBP, thereby an improvement of medication adherence can positively impact in DBP and hypertension control.75–77
Pharmacists’ interventions in patients with respiratory conditions such as counselling and education have also found to be effective at improving clinical outcomes.33 Our proposed intervention resulted in a larger increase in the percentage of controlled patients (34.7%), when compared with previous studies that reported 13%–30%.17 78 The reduction of 0.53 points in mean ACQ scores was clinically significant52 and similar to previous studies.17 78 Similarly, an improvement on the average score and percentage of patients with low clinical impact of COPD was observed. Unlike previous studies,40 79 our intervention resulted in clinically54 and statistically significant differences in mean CCQ scores from visit 3 until the end of the study, indicating the intervention was effective at improving clinical outcomes in patients with COPD.
To the best of our knowledge, this is the first study proposing a medication adherence management intervention in community pharmacies in Spain using complex interventions based on theories and frameworks of behaviour change and reporting clinical outcomes; targeting one of the priority Spanish pharmacy services37 and one of the key goals of healthcare.35 The novelty of this study is the proposal of a structured patient-tailored pharmacist intervention based on evidence-based frameworks25 and assessment of clinical variables in a community pharmacy setting. Although there is some evidence supporting the use of these frameworks in patients suffering from hypertension, it is limited for patients with asthma or COPD.
Practice implications
Findings of this study provide evidence on the effectiveness of a patient-targeted intervention and support the future implementation of a medication adherence management service in regular practice.
Limitations
Objective adherence measures such as dispensing data could not be used. There was a lack of interoperability between pharmacies hindering the access to dispensing records. Therefore, only implementation adherence through a self-reported method was assessed, which may have been affected by desirability bias. Nonetheless, in the absence of a gold standard,80 patient self-reported questionnaires have a close correlation with electronic monitoring devices.81 Due to the nature of the intervention, pharmacist blinding was impossible. This is common in studies evaluating educational interventions. The intervention’s design required the collection of data as part of the patient’s evaluation and the provision of the intervention. Therefore, it was impossible to include a blinded data collector. Blinding personnel and intervention providers is often not achievable for studies assessing educational interventions. Potential risk of bias derived from lack of blinding for pharmacists was minimised, as the main study outcomes were either participant-reported outcomes (ie, patients who were blinded to the study group) or observer-reported outcomes not involving judgement.
Positive effects were also observed in the CG for medication adherence, asthma and COPD control during the first 2 months of study. Patients often modify their behaviour when feeling observed (ie, Hawthorne effect). Moreover, data collection could have made patients more conscious of their behaviours and have impacted their health. Finally, control pharmacists may have provided more information than they would provide during usual care, even if they were instructed not to change their regular practice.
Conclusion
A structured patient-targeted intervention based on behavioural change frameworks and the assessment of clinical variables proved to be effective at improving medication adherence and disease-specific clinical outcomes in patients with hypertension, asthma and COPD. Overall, intergroup differences were significant after 3 months of follow-up, highlighting the importance of continuous monitoring in the management of medication adherence. This study proposes an approach to address patient safety and quality of care through adherence management. Integrating prescribing and pharmacy data would increase the potential of the intervention by measuring all dimensions of medication adherence. Future research should explore the implementation of these interventions in routine practice.
Data availability statement
Data are available upon reasonable request to the corresponding author.
Ethics statements
Patient consent for publication
Ethics approval
This trial follows the Ethical Principles for Medical Research Involving Human Subjects and Good Clinical Practice and International Council for Harmonisation. It was approved by the Ethics Committee of Research of Granada (CEI-Granada) (registration number: 0021-N-17).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors VGC, SIB, MÁG and FMM were involved in the conception of the work. ATR, VGC, TP, RVD, BPE and MIVM were involved in the codesign of the work and oversight of data collection. KR led the statistical design and assisted with data analysis and interpretation. ATR and VGC led the drafting of the manuscript. All authors have read and approved the final manuscript.
Funding This project was funded and supported by Laboratorios Cinfa.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.