Article Text

Abstract
Objectives The study aimed to investigate how the ‘natural experiment’ of reconfiguring the emergency healthcare system in Denmark affected in-hospital and 30-day mortality on a national level. The reconfiguration included the centralisation of hospitals and the establishment of emergency departments with specialists present around the clock.
Design Hospital-based cohort study.
Setting All public hospitals in Denmark.
Participants Patients with an unplanned contact from 1 January 2007 until 31 December 2016.
Interventions Stepped-wedge reconfiguration of the Danish emergency healthcare system.
Main outcome measures We determined the adjusted ORs for in-hospital mortality and HRs for 30-day mortality using logistic and Cox regression analysis adjusted for sex, age, Charlson Comorbidity Index, income, education, mandatory referral and the changes in the out of hours system in the Capital Region. The main outcomes were stratified by the time of arrival. We performed subgroup analyses on selected diagnoses: myocardial infarction, stroke, pneumonia, aortic aneurysm, bowel perforation, hip fracture and major trauma.
Results We included 11 367 655 unplanned hospital contacts. The adjusted OR for overall in-hospital mortality after reconfiguration of the emergency healthcare system was 0.998 (95% CI 0.968 to 1.010; p=0.285), and the adjusted OR for 30-day mortality was 1.004 (95% CI 1.000 to 1.008; p=0.045)). Subgroup analyses showed some possible benefits of the reconfiguration such as a reduction in-hospital and 30-day mortality for myocardial infarction, stroke, aortic aneurysm and major trauma.
Conclusions The Danish emergency care reconfiguration programme was not associated with an improvement in overall in-hospital mortality trends and was associated with a slight slowing of prior improvements in 30-day mortality trends.
- health services research
- emergency department
- morbidity and mortality rounds
- health policy
Data availability statement
Data may be obtained from a third party and are not publicly available. Data may be obtained from a third party and are not publicly available. According to Danish law, data cannot be shared. However, the data sources are available for other researchers pending approval from the Statistics Denmark.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
There are conflicting results on short-term mortality after reconfiguration of emergency healthcare systems.
Research on the consequences of major emergency healthcare reforms is scarce.
Additional knowledge is imperative, as major healthcare reforms are massive investments in physical and human capital and entail complex organisational changes.
WHAT THIS STUDY ADDS
The Danish emergency healthcare reconfiguration from 2007 to 2016 had no change on in-hospital mortality but slightly increased 30-day mortality.
Subgroup analyses showed a decrease in in-hospital or 30-day mortality for myocardial infarction, stroke, aortic aneurysm and major trauma, all conditions that require urgent management.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
Reconfiguration of a nationwide emergency healthcare system is a complex and massive investment.
As such, all mechanisms can never be described; however, the results of this study do not support any association between mortality and reconfiguration.
Introduction
Over the past few decades, the number of emergency hospital visits has increased in several European countries, including Denmark.1 The increasing number of emergency visits are partially due to an ageing population, with an increasing comorbidity burden, which also increases the complexity of clinical presentations.2 3 These challenges put pressure on healthcare systems and negatively influence the quality of care.4 To mitigate these challenges, healthcare system reconfiguration, where services are centralised to a small number of large facilities, has been proposed in several countries (eg, the UK, Ireland, Belgium and the Netherlands).5–8
Since 2007, the emergency healthcare system in Denmark has been reconfigured.9 This includes fewer emergency hospitals through mergers, the closing of smaller hospitals and the centralisation of specialised treatment, including emergency and acute care into one unit with the relevant medical specialists present at all times. A consequence for many patients has been longer distances and travel time to emergency departments (EDs), especially in rural areas. In addition, mandatory referral to the ED from either a general practitioner (GP) or the emergency dispatch centre was instituted nationwide. These initiatives were a part of a major reform to the healthcare system by the National Health Authority which aimed to provide equal access to uniform high-quality treatment at all times and in every part of the country.9 ThisDanish reform address issues relevant to many healthcare systems, specifically the uniform efficient delivery of high-quality emergency healthcare services. In Denmark, this includes centralising emergency care to fewer sites, a single entrance for all unplanned patients and the presence of specialist doctors 24/7.
Mortality is a key marker of care quality.10 Increased short-term mortality in out-of-hours admissions is an internationally recognised phenomenon that may be caused by a lack of experienced healthcare professionals and a shortage of staff.11–13 Several single-centre and multicentre studies have shown both reduced and increased short-term mortality after reconfiguration of emergency healthcare systems.8 10 14–18 However, research on the nationwide consequences of major emergency healthcare reforms is scarce.19 Additional knowledge is imperative, as major healthcare reforms are massive investments in physical and human capital and entail complex organisational changes. The quasi-experimental implementation of reconfiguration in Denmark provides a unique opportunity to evaluate the benefits, if any, of centralising emergency care. In this study, we aimed to investigate how the reconfiguration of the emergency healthcare system in Denmark has affected in-hospital and 30-day mortality at a national level. We exploited the natural variation in implementation across Denmark to rigorously test how the reconfiguration of emergency care affects mortality across selected diagnoses and times of arrival at the hospital.
Methods
Setting
The Danish healthcare system is tax-funded and provides universal coverage and services free of charge at the point of delivery for all of Denmark’s 5.8 million residents. However, some co-payment is required for prescription drugs. All residents are assigned a GP, who acts as the gatekeeper to secondary healthcare.20 Private hospitals represent <3% of all hospital activity and do not treat emergency patients.20
The 2007 healthcare reform
A major healthcare reform was introduced in Denmark in 2007.9 Five larger administrative units were created to serve as regional authorities. The regions are responsible for governing, managing and funding public hospitals and were responsible for implementing the reform. Hospitals were centralised, resulting in the closure of most small, rural hospitals; when the reform is fully implemented in 2025, the number of hospitals will have been reduced from 44 (in 2007) to 21 (in 2025).9 Centralisation was gradually implemented in a stepped-wedge configuration beginning in June 2008.
As part of the reconfiguration, all undifferentiated unplanned patients, except for a few specified populations (eg, children, psychiatric complaints, women in labour, etc) should initially be seen in EDs.21 Therefore, it was mandatory for specialists from internal medicine, orthopaedic surgery, general surgery, anaesthesiology and radiology to be available in the ED around the clock. However, by 2016, this reform had only been fully implemented in approximately half of the country’s hospitals,22 and it was not until 2017 that emergency medicine was recognised in Denmark as a primary medical specialty.
Although many countries allow patients open access to the ED, from 2011 to 2014 Denmark introduced a referral system. This required patients to either call their emergency dispatch centre for an ambulance or are referred by their GP. Therefore, all Danish EDs are now closed to non-referred patients.
All five regions provide out-of-hours primary care, with first-line telephone contact with either a specialised triage nurse (The Capital Region of Denmark) or a GP (the four remaining regions), who decides the next step for the patients.20 Before 2014, all out-of-hours patients had a home-visit or were asked to visit an out-of-hours clinic staffed by GPs. Since January 2014, the Capital Region did not offer home visits, and all patients who are thought to need urgent care are triaged to hospital and treated as ED patients. The change in the Capital Region, from a system like the other regions to the new system, has led to a substantial increase in the number of unplanned emergency hospital contacts.1
Data sources and study cohort
The study cohort was based on data from national databases maintained by the Danish government. We included all unplanned non-psychiatric hospital contacts by adult patients (aged ≥18 years) with a public hospital in Denmark from 1 January 2007 to 31 December 2016 with 30-day follow-up. All planned inpatient admissions, planned outpatient visits, patients in labour (International Classification of Diseases 10th Revision: O00-O99), visits to psychiatric hospitals and patients registered as dead before their hospital contact were excluded.
All residents in Denmark have a unique personal identification number that allows cross-linkage of all registers. Data were extracted from the Danish National Patient Registry (DNPR).23 The study population selected from DNPR was merged with income data (Income Statistics Register), education-level data (The Danish Education Register), country of origin, marital status, age and vital status (The Danish Civil Registration System).24–26
No visits were counted twice in the study cohort. Patients could have several unplanned visits and admissions during the study period, and they were all included in the study cohort. Transfer between departments or from the ED visit to admission was coded as separate visits/admissions in the DNPR. When an unplanned ED visit was converted to an unplanned inpatient admission, or the patient was transferred between departments within 3 hours, the visits/admissions were considered to represent the same hospital contact. Sensitivity analysis of the 3-hour rule has demonstrated that this assumption is valid.1
Outcomes
The primary outcome was in-hospital mortality, and the secondary outcome was 30-day mortality from the date of admission of the index contact (both in-hospital and out-of-hospital mortality). Patients were followed until death or the end of the study period, whichever came first. In-hospital mortality was defined as death that occurred during the hospital stay. Some patients had multiple unplanned hospital contacts during the study period, including admissions that overlapped the 30-day follow-up time; death was only assigned to the last unplanned hospital contact for these patients.
Study design
We used an interrupted time-series analysis in which contacts before the reconfiguration of the emergency healthcare system were compared with contacts that occurred after reconfiguration.27 Each hospital had a unique time period divided into two periods, before and after the reconfiguration, creating a natural stepped-wedge configuration. The unique period for each hospital was based on information obtained during telephone interviews with department leaders and public reports. We stratified the unplanned contacts into 23 hospitals with EDs in Denmark at the end of the study period.1 Three hospitals did not change during the study period; therefore, their timeline only consisted of one period, and these three hospitals acted as control hospitals throughout the study. Online supplemental figures 1 and 2 show the raw unadjusted in-hospital and 30-day mortality rates for the 23 hospitals. The main results are reported on a national level.
Supplemental material
Both an unadjusted and a fully adjusted model were performed accounting for hospitals as clusters; the hospital status after the reconfiguration was used because of hospital mergers during the study period. The fully adjusted model accounted for seasonality, changes in visit patterns due to changes in the out-of-hours system in the Capital Region of Denmark and implementation of mandatory referral to the EDs. The model was also adjusted for sex, age, Charlson Comorbidity Index (CCI; low, 0; medium, 1–2 and high, >2),28 ethnicity (Danish or non-Danish), education (low, medium or high education corresponding to the International Standard Classification of Education 1997 categories: 0–1, 2–3, 4–6) and income level (low, medium or high).
We used monthly time points for mortality and analysed a median of 53 time points (range 17–120) before reconfiguration and 67 time points (range 0–103) after reconfiguration (online supplemental figures 1 and 2). The impact model included a continuous-time variable (pretrend) throughout the study period and a continuous-time variable (slope change) from the reconfiguration date and onwards. The effect of reconfiguring the emergency healthcare system was estimated as the slope change between the two periods. The pretrend represents how the trend would have continued if the emergency healthcare system had not been reconfigured.
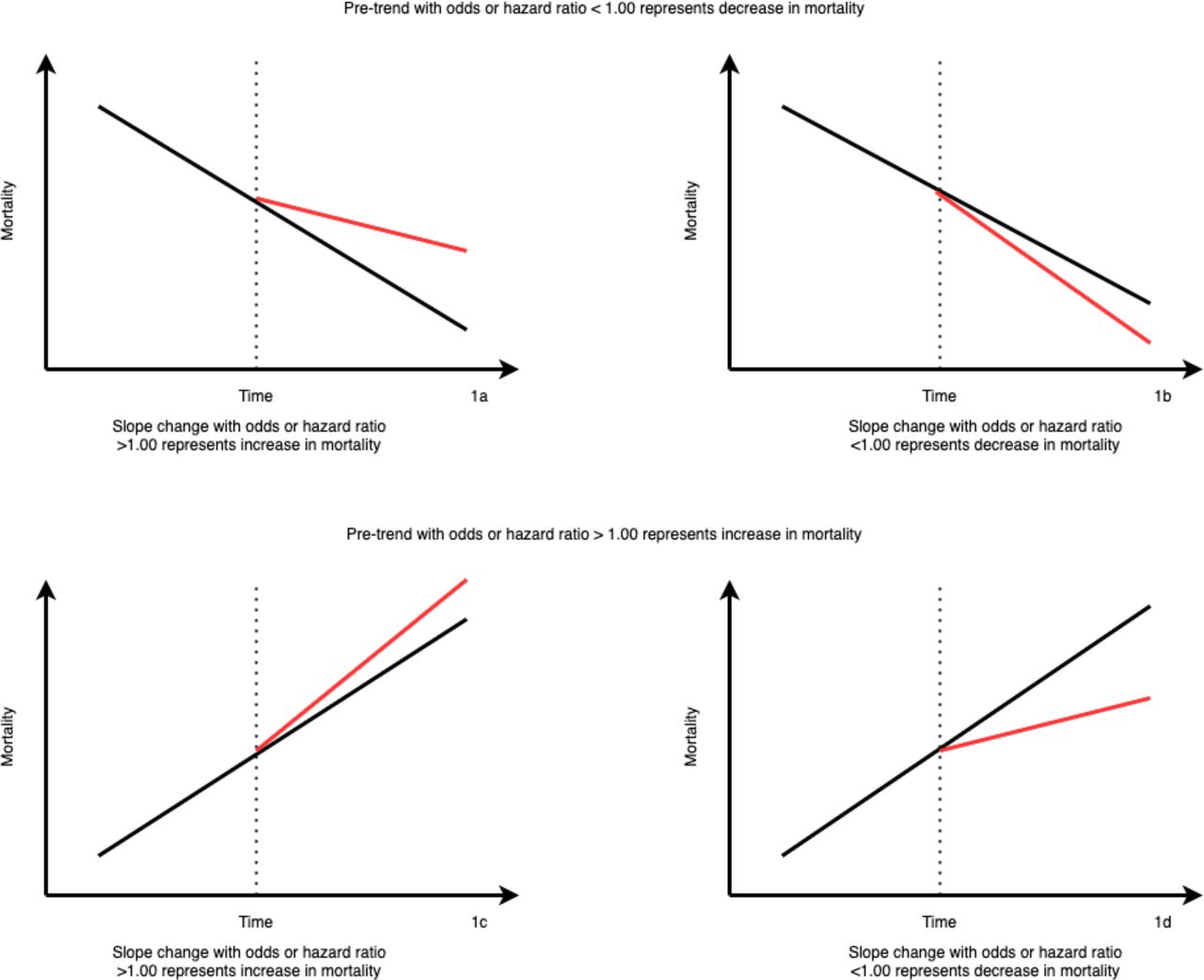
A pretrend with an OR or HR <1.00 represented a downward trend (decreasing mortality) (figure 1A,B), whereas a pretrend with an OR or HR >1.00 represented an upward trend (increasing mortality) (figure 1). A slope change with an OR or HR <1.00 represented a decrease in mortality, regardless of the direction of the pretrend. A slope change with an OR or HR >1.00 represented an increase in mortality, regardless of the direction of the pretrend. Therefore, a downward pretrend with an OR or HR for slope change >1.00 can still have an overall decrease in mortality (figure 1).

{kind=link}
Different possible outcomes in interrupted time series. The dotted line represents the time of reconfiguration. The black line represents how the mortality trend was before the reconfiguration and would have continued if there was no reconfiguration of the emergency healthcare system. The red line represents the new trend after the reconfiguration of the emergency healthcare system. Slope change is the difference between the black and red lines.
Subgroup analyses
We performed subgroup analyses in which the population was restricted to unplanned contacts with selected diagnoses (primary and secondary discharge diagnoses), including myocardial infarction, stroke, pneumonia, aortic aneurysm, bowel perforation, hip fracture and major trauma (see online supplemental table 1). Myocardial infarction, stroke, aortic aneurysm, bowel perforation and major trauma were chosen as specific diagnoses that require time-critical intervention. Hip fracture and pneumonia were less time-sensitive but frequent diagnoses. We expected that some of the diagnoses would benefit from the reconfiguration of the emergency healthcare system (myocardial infarction, stroke, aortic aneurysm, bowel perforation and major trauma), whereas others would be expected to stay stable (pneumonia and hip fracture). These diagnoses are presented with the same outcomes and stratifications as the primary analyses.
When possible, the subgroup analyses were adjusted for the same variables as the main cohort. As some subgroup analyses had too few cases for the adjusted variables, the variables were removed one by one until analysis was possible. The predefined order for removing variables was ethnicity, education level, income level, CCI, age and sex.
Stratification
The analyses were stratified according to time of day for index contacts (categorised into three periods: daytime (07:00–14:59 hours), evening (15:00–22:59 hours) and night (23:00–06:59 hours)). Contacts were also defined as ‘weekend’ if between Friday 15:00 hours and Monday 06:59 hours, or ‘weekday’ if between Monday 07:00 hours and Friday 14:59 hours. These categories were chosen to investigate whether patients always received a uniform and high-quality care based on the standard shifts in Danish healthcare. Before reconfiguration, specialists were on call from home during the evening and night.
Statistical analysis
Baseline characteristics for unplanned contacts are presented as the means and SDs or medians and IQR for continuous variables and as frequency and percentage for categorical variables. The Wilcoxon rank-sum test was used to compare continuous variables, and Pearson’s χ2 test was used to compare categorical variables. In-hospital mortality was analysed by logistic regression and 30-day mortality as parametric time-to-event analyses with Weibull distribution. Patients with more than one contact within 30 days only accounted for risk time until the next contact in the time-to-event analyses. Data management and analyses were carried out in Stata V.15 (StataCorp, College Station, Texas, USA). A significance level of 5% was applied.
Patient and public involvement
This research was performed without patient involvement. Patients were not invited to comment on the study design and were not consulted to develop patient-relevant outcomes or interpret the results. Patients were not invited to contribute to the writing or editing of this document for readability or accuracy.
Results
Our study included 11 367 655 emergency patient contacts, 4 704 362 before and 6 663 293 after the reconfiguration of the emergency healthcare system. The median age of patients, proportion of females, median income and proportion with a high education increased slightly, whereas the proportion with Danish ethnicity, married contacts and contacts with a low comorbidity score decreased slightly (table 1). As one would expect given the very large sample sizes, all precomparisons to postcomparisons are statistically significant but the two cohorts were in fact very similar.
Baseline characteristics of unplanned contacts before and after the reconfiguration of the emergency healthcare system
Before reconfiguration, the raw unadjusted monthly in-hospital and 30-day mortality rates at individual hospitals ranged from 1.1% to 6.6% and 1.6% to 7.6%, respectively, and after reconfiguration from 0.6% to 4.5% and 1.2% to 5.5%, respectively. The three hospitals without reconfiguration had raw unadjusted monthly in-hospital and 30-day mortality rates ranging from 0.4% to 4.8% and 0.8% to 5.7%, respectively (online supplemental figures 1 and 2).
We observed a significant annual decrease in the adjusted in-hospital mortality (pretrend) of 5.5% before reconfiguration (table 2). Reconfiguration was not associated with a significant change in the annual adjusted in-hospital mortality (adjusted slope change). The results for time periods (table 2) were like the overall findings, with an annual significant decrease (4.8%–5.8%) in the adjusted in-hospital mortality before reconfiguration (adjusted pretrend) and no effect of the reconfiguration on in-hospital mortality (adjusted slope change).
ORs for in-hospital mortality for the pretrend and slope change related to the reconfiguration of the emergency healthcare system
The overall annual decrease in adjusted 30-day mortality before reconfiguration was 3.5% (adjusted pretrend), and reconfiguration was associated with an 0.4% per year slowing in the rate of decrease (adjusted slope change) (table 3). Regardless of the time of week or day, adjusted 30-day mortality significantly decreased by 3.0%–3.6% per year before reconfiguration (adjusted pretrend). The adjusted 30-day mortality rate did not change after reconfiguration when stratifying for weekdays and weekends (adjusted slope change). When stratifying by the time of day, we found reconfiguration was associated with a significant improvement in the mortality trend for patients presenting at night-time by 1.5% per year. After reconfiguration, the adjusted 30-day mortality trend for patients presenting in the evening was unchanged, but the improvement trend slowed for patients presenting during the daytime by 0.8% annually.
HRs for 30-day mortality for the pretrend and slope change related to the reconfiguration of the emergency healthcare system
Before reconfiguration, adjusted in-hospital mortality had been significantly decreasing over time for myocardial infarction, stroke, pneumonia, bowel perforation and hip fracture (table 4 and online supplemental tables 2-15). None of these diagnoses experienced changes to in-hospital mortality trends after reconfiguration. However, the annual adjusted in-hospital mortality trend for aortic aneurysm and major trauma improved significantly after reconfiguration.
ORs and HRs for subgroups for the pretrend and slope change related to reconfiguration of the emergency healthcare system
The adjusted 30-day mortality trend improved significantly after reconfiguration for contacts with myocardial infarction, stroke and aortic aneurysm (adjusted slope change). No impact on these trends was observed for pneumonia and bowel perforation.
Discussion
Principal findings
This nationwide interrupted time series study showed that reconfiguration of the Danish emergency healthcare system was not associated with a change to in-hospital mortality trends, but it was associated with a slight slowing of the prior improvement in 30-day mortality rates.
The goal of the healthcare reform by the Danish National Health Authority was to provide equal access to uniform, high-quality treatment in every part of the country at any time of day.9 This included centralisation, hospital mergers and closures, specialists present around the clock, mandatory referral before access to the ED and longer travel times. In this study, we have investigated these as one intervention and have not considered its multiple components’ specific contributions and possible interactions. In addition, the 23 hospitals included in this study had different baselines before the reform, and some hospitals and their patients experienced more changes than others. Furthermore, hospitals have implemented reforms according to different local configurations, which were not explicitly defined by the government.29
We expected mortality to decrease for rare but dangerous and time-critical diagnoses (eg, myocardial infarction, aortic aneurysm and bowel perforation) and to remain unchanged for the more frequent and less time-dependent diagnoses (pneumonia and hip fracture). Our results confirm some of these assumptions, as there was a decreased in-hospital mortality rate for aortic aneurysm and major trauma and a decreased 30-day mortality rate for aortic aneurysm, stroke and myocardial infarction.
Comparison with other studies
Evidence from nationwide reconfigurations of an emergency healthcare system is limited. A national study from the Ireland showed a decrease in case fatality ratios for serious emergency conditions from 2002 to 2014, with a slowed rate from 2007 and onwards that coincided with a period of economic contraction.17 The authors found geographical differences in case fatality ratios. This study also addressed the complexity of evaluating a reconfiguration. Some mechanisms, such as improved healthcare staffing, may improve the outcome, whereas delay in care is more likely to affect the outcome negatively. This study confirms the complexity of evaluating the Danish reform, as it introduced several mechanisms (eg, centralisation, senior decision-makers present out of hours and longer travel distance) simultaneously and each of these on its own has been shown to affect mortality.9 Although we have not tested the single mechanisms involved in the reform, as this was beyond the scope of this paper, some mechanisms may have improved outcomes, whereas other mechanisms may have induced an increase in mortality.
A further study from England showed decreased 60-day mortality rates year 1 and 2 years after the centralisation of EDs.18 In contrast, a multicentre study found no evidence of an association between changes in emergency care and population mortality.8
Prior research has shown that care outside of normal business hours has the best potential for improvement.13 When stratifying our results for day and time of arrival, we found no difference in in-hospital mortality. However, reconfiguration did improve the overall 30-day mortality at night. Our findings on in-hospital mortality are in line with another Danish study that found no change in in-hospital mortality after introducing consultants to the ED.30
We found decreased in-hospital and 30-day mortality at night and on weekends for myocardial infarction, stroke, aortic aneurysm and major trauma, which are all time-sensitive diagnoses. Similarly, high-risk, time-sensitive diagnoses (aortic aneurysm) are best handled by experienced staff, whereas other diagnoses (pneumonia and hip fracture) do not seem to benefit from higher volumes.31 We were unable to show that in-hospital mortality from myocardial infarction improved with reconfiguration. A recent, large study from Sweden showed increased mortality in the first year after centralisation and improved survival in the following years.32 We think that the primary reason for our findings is that all Danish patients with suspected myocardial infarction have been received at four hospitals since 2003 and the reconfiguration of the emergency healthcare system did not affect this.33
A mandatory referral has been shown to reduce the number of unplanned patients by 9.4%, mostly among the young and those without comorbidity.34 The national mortality did not change during the period of the stepped-wedge implantation of mandatory referral.34
Centralisation increased the distance to the hospitals for many patients,35 but the Danish Healthcare reform included an improved prehospital system.9 A recent review of travel time and distance to EDs showed no evidence of an association between increased distance and mortality for the general population.36
Strengths and limitations of the study
We tried to address many of the mechanisms in the reconfiguration of emergency healthcare that might affect mortality, but there were still several mechanisms that were unaddressed. Severity of illness, staffing, organisation of the ED and the fact that some patients could have stayed at home because of longer travel distance were some of the known mechanisms that can affect mortality, and unknown residual confounders were a part of the reconfiguration. Although the study design took unknown confounders that were stable over time into account evaluating a healthcare reconfiguration is still complex and many known and unknown things affect mortality.37
We tried to set a fixed implementation date for each hospital, but this was somewhat arbitrary, as reconfiguration of a hospital does not happen overnight. In addition, through our design, we were unable to identify the effect of each of the individual changes made as part of the reconfiguration. When evaluating longitudinal effects, interrupted time series is a strong quasi-experimental design,38 but our model does not fully account for a non-linear or an accelerated trend. We used stepped-wedge inclusion, adjusted for known interventions, and included control hospitals.27
We are unaware of any changes in registration practice occurring during the study period. Data may have been missing from some of the registers, particularly information on education level as the registers only cover 85%–90% of education data for immigrants. The adjusted analyses were made on complete cases. We only studied national trends, which may not reflect those of individual hospitals.
We have chosen to stratify our results in time periods that reflect the Danish healthcare professionals’ working hours, although these are not completely identical to international working hours.
The strengths of the study are the nationwide design, the use of linked personal data from high-quality Danish registers,39 and the inclusion of all emergency hospital contacts. Another strength is the subgroup analyses of specific diagnoses, as these subgroups are more homogenous than the main cohort.
Policy implications and future directions
Reconfiguration of a nationwide emergency healthcare system is a complex and massive investment. As such, we can never describe and attest to all mechanisms. Our results should be interpreted with caution, and additional studies are needed to clarify whether the severity of illness in unplanned patients has changed. In addition, studies on the effect of increased travel time are needed. Mortality is one of the last things to be affected by systemic change. We previously investigated the length of stay in the same study cohort and found no changes after the reconfiguration.40 Our findings suggest that reconfiguration in Denmark was not associated with a change to in-hospital mortality trends, and was actually associated with a slowing of prereconfiguration improvements in 30-day mortality trends. This may be because of poor implementation, as 10 years after the reform, three hospitals have still not been reconfigured. Geographical and hospital differences may also affect the results. Further research is needed at the geographical level.
Conclusion
An evaluation of the Danish emergency healthcare reconfiguration from 2007 to 2016 found it was associated with no change to in-hospital mortality trends and a slight slowing of 30-day mortality trends. Subgroup analyses showed an improvement in in-hospital or 30-day mortality trends for myocardial infarction, stroke, aortic aneurysm and major trauma.
Data availability statement
Data may be obtained from a third party and are not publicly available. Data may be obtained from a third party and are not publicly available. According to Danish law, data cannot be shared. However, the data sources are available for other researchers pending approval from the Statistics Denmark.
Ethics statements
Patient consent for publication
Ethics approval
In compliance with Danish law, register studies are exempted from gaining approval from an ethics committee; however, we did gain approval from the Danish Data Protection Agency (file no. 17/18411).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @BieBogh
Contributors MF are the guarantor, managed and analysed the data and drafted the manuscript. SBBB contributed to data management. MBr performed critical appraisal of the manuscript. MF wrote the paper. SBBB, DPH, MBe, SPJ and MBr contributed to writing, reviewing and revising the paper. All authors interpreted the data and critically reviewed drafts of the manuscript. All authors edited and approved the final manuscript.
Funding This study was funded by Region of Southern Denmark (J.nr.: 18/17846) and Syddansk Universitet (18/17079120-090987).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.