Article Text

Abstract
Objectives Redesign in healthcare has increased the focus on the needs of the patient. The redesign process typically involves a review of current practice using the patient pathway before considering possible improvements. The patient pathway can serve various roles, and it may be mapped in different ways using a variety of media. This paper reviews the evolution of the patient pathway comparing the merits of different media.
Methods Simple approaches to mapping pathways can be most useful. However, experience in the redesign of Unscheduled Care in NHS Fife suggests that computer-based, hierarchical pathway models using stylised icons offer many advantages.
Results and Conclusions Such approaches can increase the effectiveness of pathways in the redesign process, providing both the detail and the system view in an accessible graphical form. This enhanced capability helps staff analyse current practice and visualise and assess redesign options. In addition, the pathway can fulfil new roles as a training tool and an effective basis for organising knowledge about patient care.
- Emergency medical services
- clinical pathway
- process mapping
- redesign
- healthcare
Statistics from Altmetric.com
The National Health Service (NHS) in the UK has initiated a significant programme of redesign to improve service delivery.1 The redesign methodology has been developed from techniques that been have been effective in industry while ensuring that the main focus is the patient's needs.2 The programme of redesign was pioneered by the Modernisation Agency in England, which has the task of disseminating best practice and stimulating change.3 An important tool in understanding patients' needs is the patient pathway. A variety of pathway models are available, employing a range of media. Some are simple and accessible but with limited capability; others exploit computer technologies. Some pathway models aim for a very precise definition of the activities, as required when specifying an engineering system; others place a greater emphasis on communicating a systemic vision to a wider audience. This paper compares the requirements for patient pathway mapping in redesign with the capabilities of different pathway models and demonstrates the benefits of one particular method used in the redesign of Unscheduled Care.
The development of the redesign process
Redesign methodology has its origins in Business Process Reengineering (BPR). This has been widely used in industry for >30 years and has evolved into a collection of recommended practices.4 BPR has been used in the NHS with some success; in one application,5 it was claimed that redesign can improve the quality of care, staff moral and job satisfaction as well as provide cost savings of 10% to 15% by reducing duplication and waste. The method of redesign proposed for the NHS was a mixture of BPR with elements of Total Quality Management and the Theory of Constraints6 ,7 but with the patient being at the centre of the process.8 The Theory of Constraints' emphasis on adopting a systems view is particularly relevant in healthcare, which often involves the co-ordination of numerous services.9 The development of an understanding of a complete system implies a requirement for mapping and communicating patient pathways. Pathway mapping is often a major element in the deliberations of Plan Do Study Act meetings of local staff, helping them appreciate the whole system when identifying and managing constraints.10 Redesign aims to improve the processes and also question component activities, reducing organisational waste. The historical organisation of healthcare was typically functional, requiring the patient to move between services as treatment progressed. This can imply a number of patient visits with intermediate waits. The aim is to redesign care adopting a process-orientated system, with the main focus on the needs of the patient as represented in the pathway.11 ,12 This should result in fewer patient visits, less waiting and more efficient use of staff and facilities.
The redesign process typically involves establishing a multi-disciplinary team under clinical leadership,3 with a range of clinical and management staff6 representing the main specialties and services associated with the pathway. Mapping the current pathway is the initial step in redesign,6–8 14–16 usually beginning with high-volume pathways that might offer the greatest benefits.17 The process should develop a common understanding of the pathway capturing the physical patient journey, the flows of information and staff responsibilities. The mapping process itself can be most valuable, provoking debate so that the staff gain a greater appreciation of their role in the whole care system. The maps may be used to highlight duplicate and redundant activities, causing staff to question activities that do not add value to the patient's journey or to re-examine established routines; this may involve comparisons with pathways from other hospitals, or specialties. Revised pathway maps are then developed and distributed, allowing staff to consider the proposals carefully before agreeing on the new design.
Pathway maps: from a systems' engineering tool to universal communication
The challenge of pathway mapping is to provide both a high-level view that illustrates the whole care system and the detail of specific activities. Traditional process maps were intended for the design of information or mechanical systems using accurate, succinct language for communication between expert analysts. Such maps are essential when an unambiguous, precise specification is needed. One example used in analysing clinical information systems is Integrated Definition for Function Modelling.18 Such tools are valuable for systems analysts, but the precision is achieved at a price: the notation appears complex and can become a barrier to communication. Traditional maps employ an array of shapes and a substantial amount of text.19 Such maps can be unsuitable for multi-disciplinary teams engaged in healthcare redesign where a more accessible form of mapping is required.
In response to this need, a number of different mapping methods and media have evolved: four approaches were explored during this study. A comparison of these approaches is summarised in table 1 using criteria identified through consultation with users in conjunction with experience from other studies. Many of the criteria of table 1, notably 1–5, 8 and 9, were developed from a specific study of clinical process mapping.20 Criteria 10–12 express the standard requirements21 for a tool to be accessible, such that staff might input data to generate pathways with minimal support and provide useful outputs for two distinct audiences, the system designers and the non-experts. The potential of the pathway as a means of organising documentation and hence providing a training resource was identified in the course of this study, reflecting user suggestions; criteria 6–7 were added to reflect this requirement. The development of the criteria set and the evaluation of the different approaches were undertaken using the framework of a simple application of multiple criteria decision analysis22 incorporating the hierarchy of needs and the variations in users' priorities. The multiple criteria decision analysis scores are illustrated in table 1, reflecting the experiences of a range of users.
Pathway medium comparison (scores: ■ fulfils requirement; □ partially meets requirement; - poor)
A simple method of pathway mapping employs Post-it notes (figure 1); this method needs no specialist skills. Participants in the redesign can contribute, modifying the positions of activities while colour coding of notes can help distinguish classes of activities. There are no technological barriers, and all can be involved in the construction of the pathway map. The free form of such maps is attractive, but the lack of discipline makes comparisons between pathways difficult and unsuitable for documentation. Physical limitations make the Post-it-based map difficult to disseminate or store. The mapping exercise can be useful, but further work is needed to transfer the maps into a more structured form.

Post-it note mapping.
The traditional flowchart format (figure 2) provides an accurate representation of the patient pathway, which can be easily distributed on paper. The maps contain much detail and provide unambiguous documentation. However, they quickly become complex, and the text-based format makes it difficult to assimilate information to appreciate the whole system and identify duplicate or redundant activities. Various formats of flowcharts can be used—for example, the functional representation, which has been found useful in healthcare.23
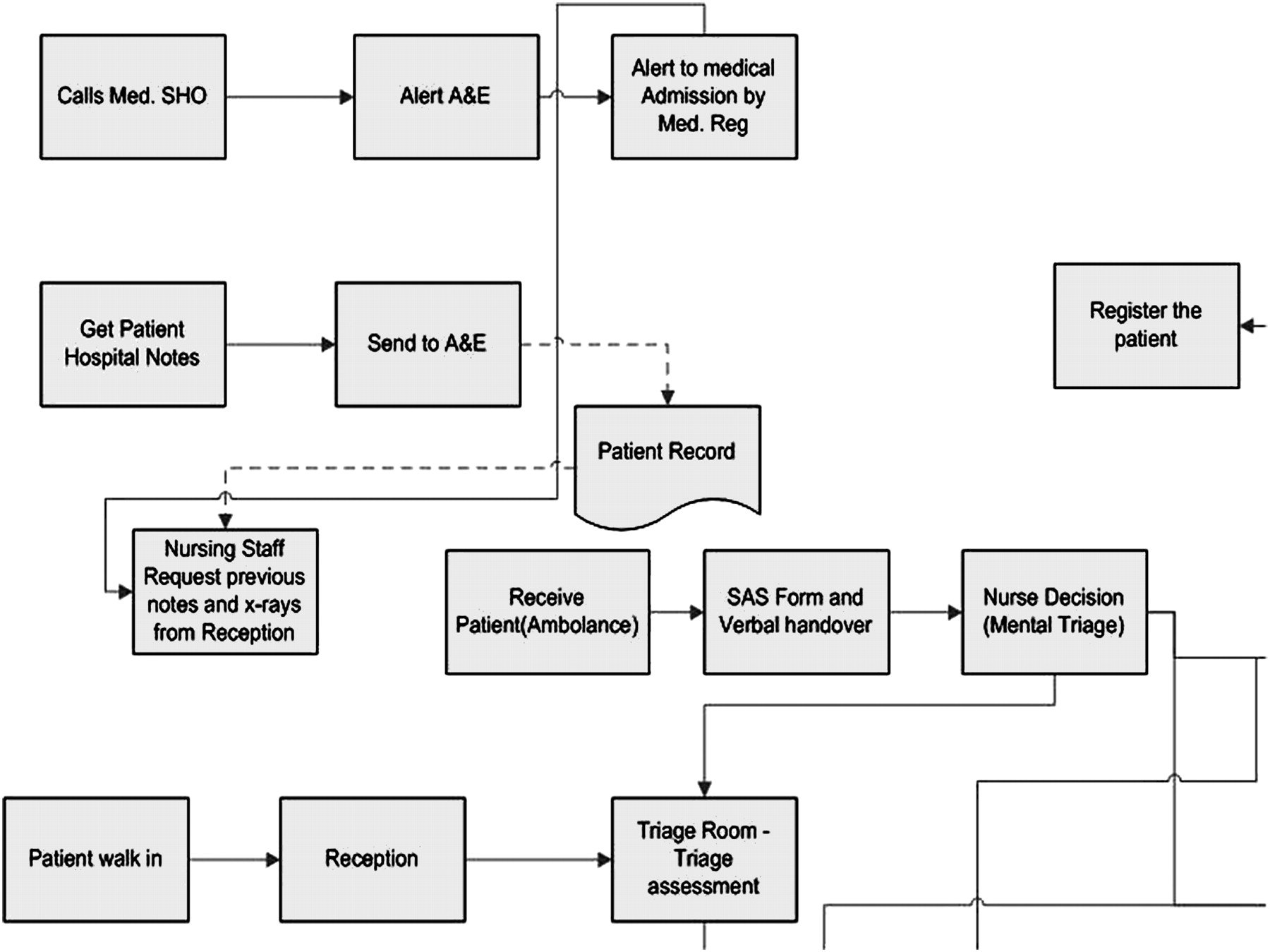
A segment of a traditional flow chart representation of the pathway.
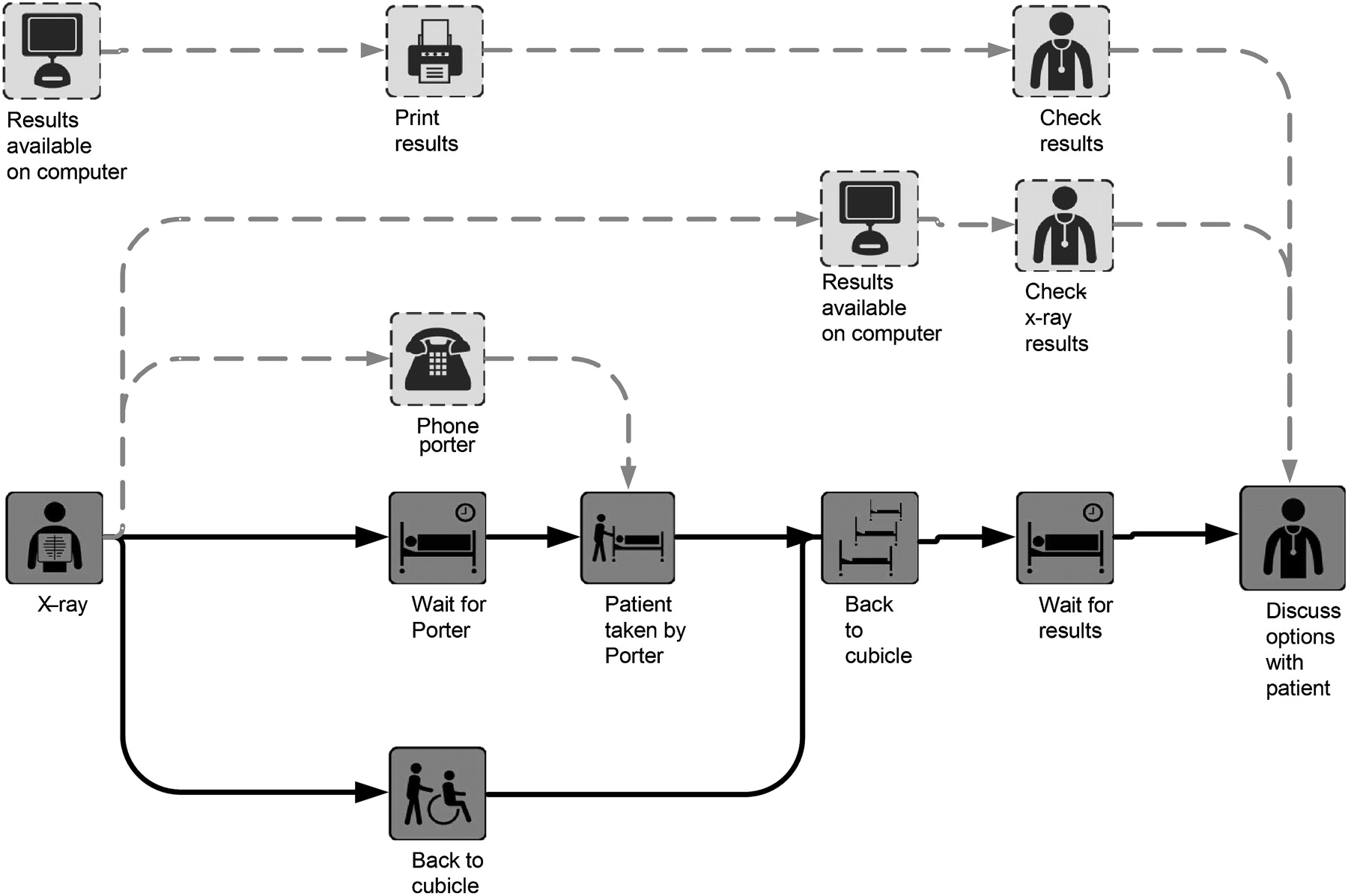
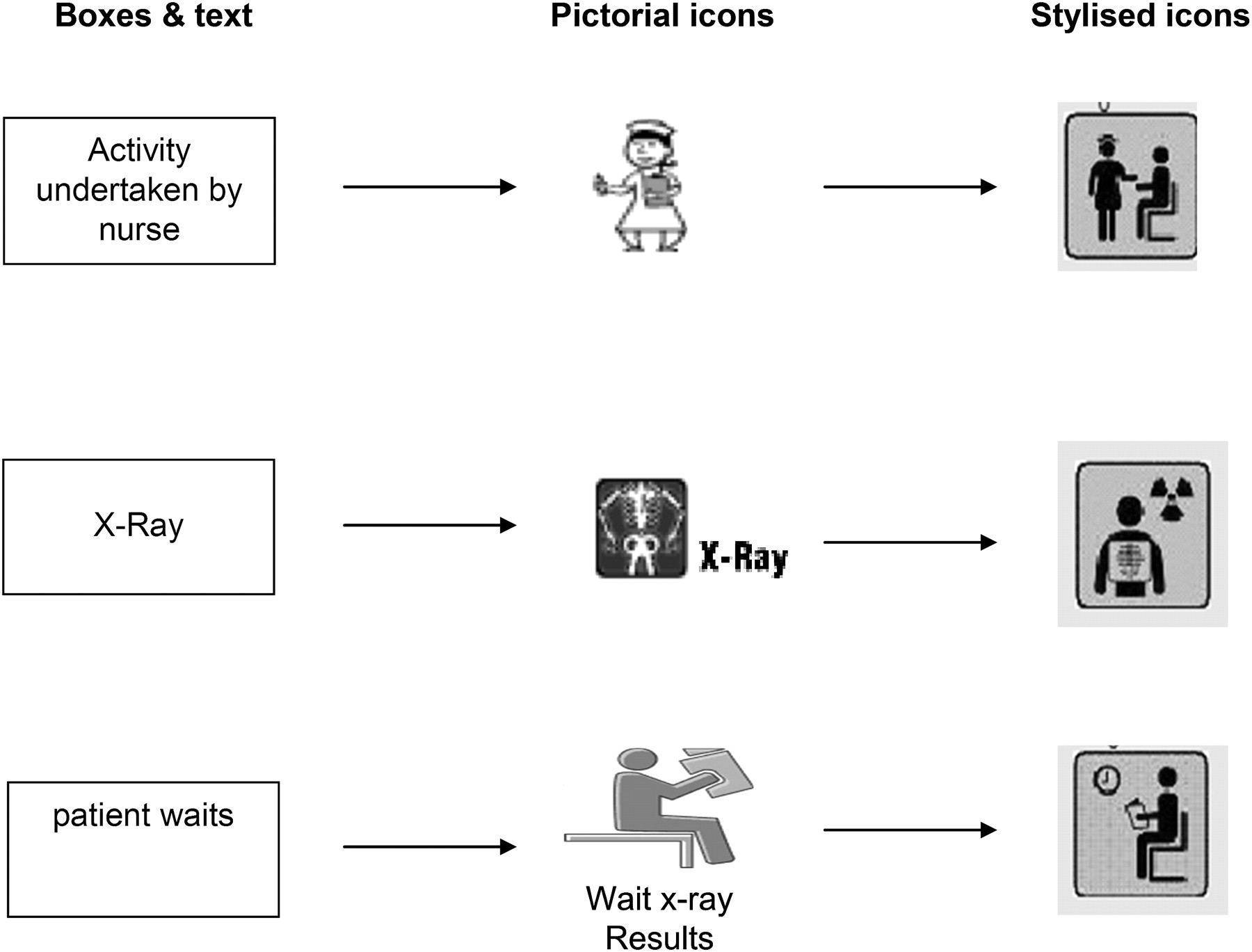
The challenge of providing a more universal language for pathway mapping has led to replacing text with symbols, chosen to relate to the target audience (figure 3). Even simple pictorial icons can provide better communication, although a more carefully designed,24 stylised set of icons offers more advantages (figure 4). This evolution from text, through simple pictorial icons to stylised icons, is illustrated in figure 5. It has been suggested25 that the design should consider five factors: styling quality, message quality, meaningfulness, locatability and metaphor. These factors have been explored in healthcare systems where the response of staff confirmed the value of using stylised icons.25 The key design principle was to strive for simplicity while ensuring that users can relate their mental models to the chosen icons. Wherever possible, text was avoided as this may include jargon, which can be a barrier to communication with users. However, even with well-designed icons, a short training session is recommended26 to minimise ambiguities. The use of icons can facilitate the analysis of the pathway, assisting the comparison between pathways and identifying those activities worthy of more investigation. However, large graphical maps can become difficult for staff to absorb and hard to modify when considering redesign options.
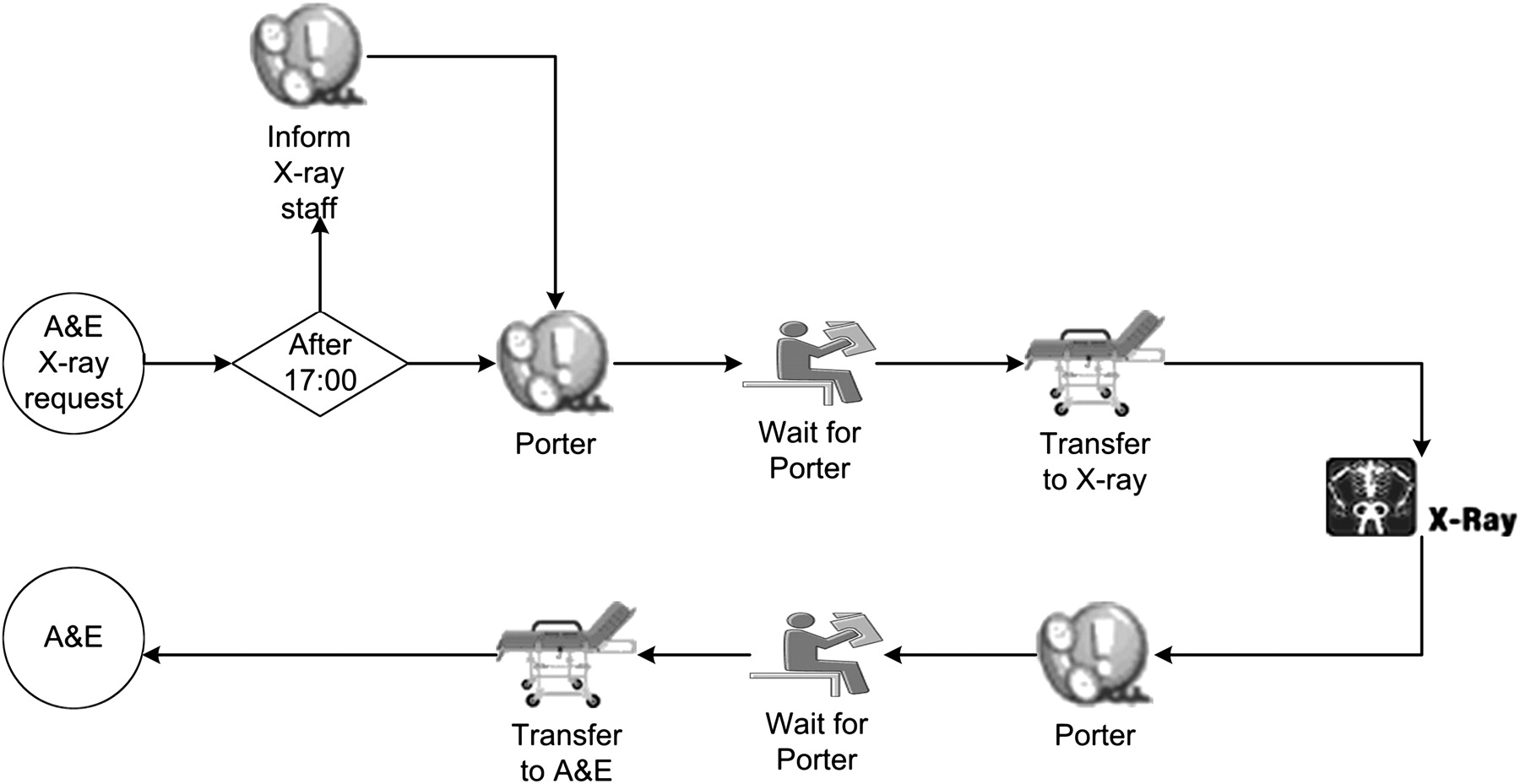
A flowchart representation of the x ray pathway from accident and emergency using pictorial icons.
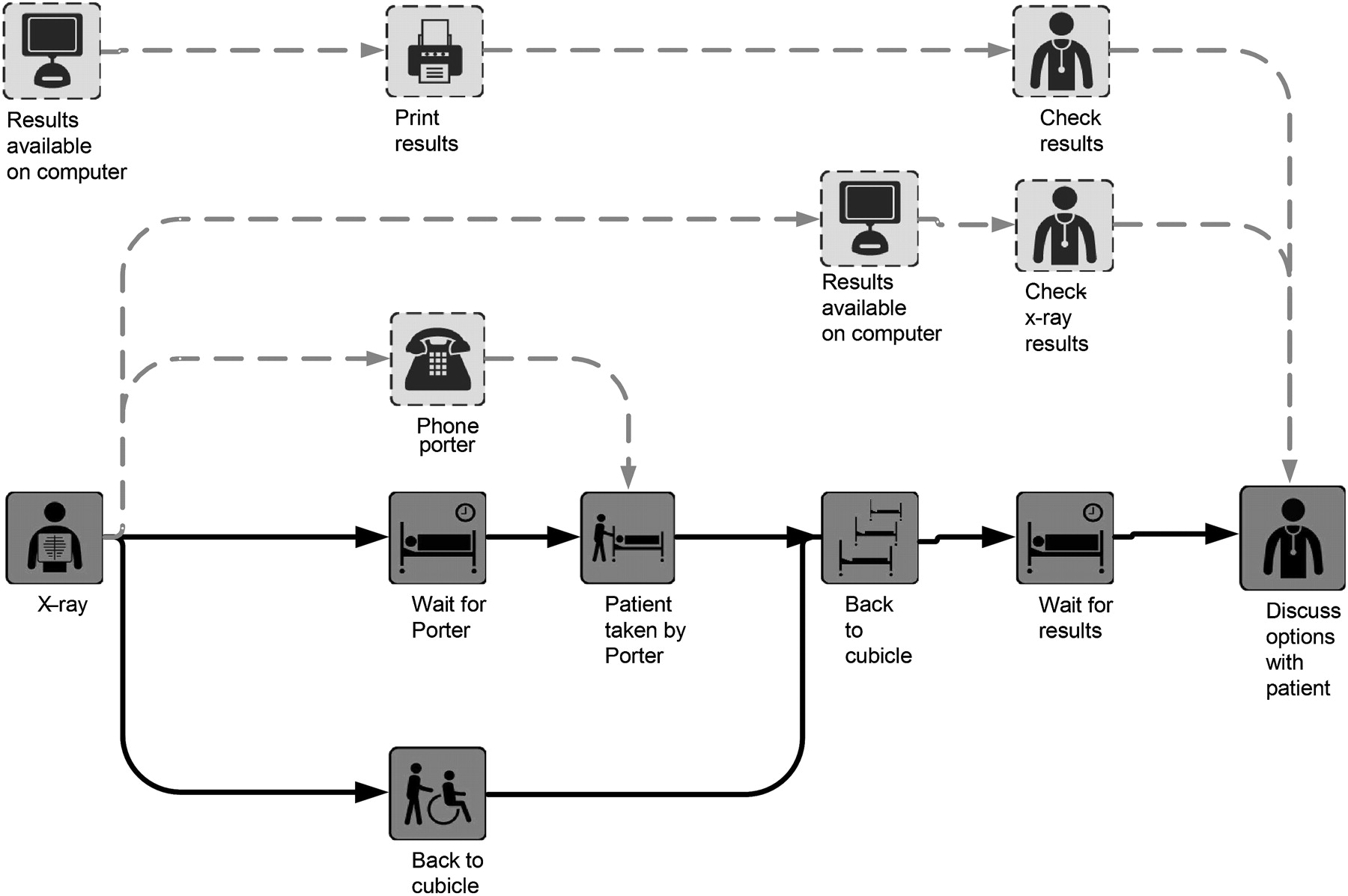
An x ray subpathway map using stylised icons distinguishing patient and information flows.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The evolution of icons.
A further development is the use of an electronic format (HTML) with hyperlink facilities to display different levels of detail. Modern software, such as Microsoft Visio, enables non-expert users to quickly produce pathway maps. This approach offers a number of technical benefits: ease of modification, distribution via an intranet, hierarchical maps, hyperlinks to further sources of information. These capabilities allow maps to be readily modified to record variations in practice, reflecting local conditions or capturing suggestions for improvement. Intranet distribution can increase dissemination and feedback, and using a hierarchy of maps, it is possible to offer a high-level view and the option of more detailed subpathway maps (figure 4). These detailed maps can include flows of information and patients, with the option to highlight specific flows as required. In addition, the pathway has the potential to provide a repository of knowledge with the hyperlinks from the icons directing the user to relevant reports, statistics and training materials.
Example: redesign of Unscheduled Care
The pathway mapping tools were developed in NHS Fife with the initial focus on the redesign of Unscheduled Care. In July 2005, NHS Scotland formed the Unscheduled Care Collaborative Programme27 to improve services; one high-profile target was the 4-h maximum time for treatment in accident and emergency (A&E). Teams comprising of clinicians, managers, representatives from associated services and an analyst met regularly to redesign patient pathways. The mapping process entailed the analyst working with the team to produce a draught pathway. Initially, the map used the traditional text-box representation (figure 2). This detailed map was not readily understood by the redesign team. They accepted that it provided accurate documentation, but they could not see how it could help in the redesign process. The complexity of the map made it difficult to identify redundant tasks; the flow of information could not easily be distinguished from the flow of the patient, nor could categories of patients be differentiated.
Simulation is an example of a process modelling tool that uses graphics to enhance communication, and it was thought that a similar approach might be employed in pathway mapping. Permission was obtained to use Simul828 pictorial icons, and the maps were redrawn (figure 3). In addition, HTML facilities were used to produce a hierarchy of maps: a simplified high-level map incorporating the ability to drill down to detailed maps of specific subprocesses. The team found that these maps enabled an appreciation of the whole system of care while still providing precise details of individual activities.
The pictorial icons facilitated easy recognition of similar or redundant activities. For example, the 17 opportunities for telephone calls during a patient's journey through A&E were questioned. The duplication of clerking-in in both A&E and the in-patient admission ward was also identified; this problem was well known among the nursing staff, but the pictorial maps enabled the issue to be appreciated by the whole team. The pathways also highlighted the patients' waiting between activities: the availability of porters was recognised as a significant cause of delay, and a porter was recruited specifically for A&E. Further delays were identified among patients awaiting assessment by therapy staff, and in response, therapy services were introduced earlier into the patient pathway, enabling more parallel working. Performance statistics were added to the maps to provide more analytical power. These highlighted the waiting associated with assessment by a doctor and led to a review of staffing and shift patterns. The user could also select a particular category of patient—for example, major/minor, surgical/medical—and view only the activities relevant for that patient. This encouraged discussion about specific patient categories and their needs. It was recognised that many minor patients could be treated by nurses, allowing doctors to concentrate on more seriously ill patients. Examination of the pathways led to questioning the value of triage and a proposal for a multi-disciplinary team of clinicians that could be assembled for the rapid assessment of major trauma patients, ensuring good care for such patients while minimising the disruption of the treatment for other patients.
In addition to debates among the redesign teams, the pathway maps were distributed, and comments were invited by email. This encouraged the participation of junior members of staff who may be reluctant to speak in large meetings. The maps were then revised and redistributed for further feedback. The mapping process could lead to disagreements about current practice; such disputes were typically resolved by tracking a small sample of patients to confirm the detail of the pathway. The response to the pathway mapping from both management and clinicians was very positive. The staff felt that the mapping tool could provide the detail required for documenting processes and also communicate the relationship between individual processes and the whole system of care. As the applications expanded, the range of pictorial icons was increased and a graphic design company24 was employed to produce a consistent set of stylised icons (fig 4) that could be used for signage and mapping.
The maps were used, with the performance statistics, to compare practices in two acute hospitals in NHS Fife. This provided greater insight, helping staff identify differences in practice and local conditions that explained some of the variations in performance. The comparison led to a transfer of practice between the hospitals. As a result of the programme of change throughout Unscheduled Care, NHS Fife comfortably met the targets. Many staff and actions contributed to this success, with the pathway maps playing a variety of roles in analysing current practice and identifying redesign options.
The evolution of the pathway mapping tools from the traditional text box flowchart to the stylised icons took 18 months. The experience demonstrated the value of the pathway in providing: a more systemic appreciation of care activities; better communication and a shared understanding of the current organisation of care; a means of comparing practices; a tool for analysing the current system; a focus for debating changes to current practices. The ability to revise the pathway maps meant that it was relatively easy to provide a variety of possible pathways representing possible variations in practice. The structured, computer-based nature of the maps, combined with stylised icons, aided communication and dissemination, helping share proposals and encourage feedback from a range of stakeholders. Further roles for the maps were identified, including training and a framework for organising relevant documentation, which also include useful literature and statistics. Simple approaches are often valuable and can sometimes be the most appropriate, but this full range of benefits was only possible using the more technologically advanced media.
Further developments
Following the success in the redesign of Unscheduled Care, the pathway mapping tools have been widely used throughout NHS Fife in services as diverse as mental health and physiotherapy. The tools are now being deployed in Planned Care to meet the target of achieving referral to treatment times <18 weeks. Many staff have been trained in the use of the tools so that the patient pathway map has become a routine component of redesign in NHS Fife.
Acknowledgments
The authors would like to acknowledge the help and support of Mr Ken Laurie, Director of Strategic Change in NHS Fife, who contributed many ideas and gave important feedback during the development of the pathway mapping technique.
References
Footnotes
Funding The work was undertaken as part of a 3-year Knowledge Transfer Partnership project (No. 537) between the University of Stirling and NHS Fife. The funders were NHS Fife and Momenta (on behalf of the ESRC).
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed