Article Text

Abstract
Background Respiratory distress syndrome and chronic lung disease are prevalent disorders in extremely low-birth-weight infants. Evidence demonstrates that timely surfactant administration improves respiratory outcomes.
Objective To assess whether basic quality-improvement methods can reduce the time to initial surfactant dose for premature infants.
Design/methods The study was conducted in a 48-bed neonatal intensive care unit (NICU) within a midsize academic centre. The authors included infants less than 27 weeks born from May 2007 to November 2007. Prior to the intervention, we obtained baseline data on the timing of initial surfactant dose. The intervention was designed using a series of Plan–Do–Study–Act cycles. The authors changed the process of surfactant administration to include administration of surfactant in the delivery room and a respiratory therapist on the delivery room team. The primary outcome measures were percentage of eligible infants who received surfactant in the delivery room and minutes after delivery at which the initial dose of surfactant was administered.
Results After the authors changed the surfactant administration process, 20/21 (95%) of eligible infants received surfactant in the delivery room. The authors decreased the time after delivery of initial surfactant dose from a mean of 26 min to 10.2 min (p=0.0004). The variation in timing of the initial surfactant dose also decreased.
Conclusions The authors demonstrated that quality-improvement methods can be used to improve the timeliness and reduce variation in timing of surfactant administration within a NICU. Future studies should assess whether these results can be replicated in a variety of NICU settings.
- Healthcare quality improvement
- teamwork
- continuous quality improvement
- statistical process control
Statistics from Altmetric.com
Introduction
Background knowledge
Respiratory distress syndrome and chronic lung disease are common disorders in extremely low-birth-weight infants. Evidence from randomised, controlled trials demonstrates that prophylactic surfactant, as compared with delayed rescue treatment, improves respiratory outcomes.1 The benefits of prophylactic surfactant are most pronounced in infants less than 30 weeks' gestation and include improved clinical outcomes and a decreased risk of pneumothorax, pulmonary interstitial emphysema and mortality.2 Prophylactic surfactant therapy offers the advantage of replacing necessary surfactant before respiratory insufficiency develops and decreasing the risk of prolonged ventilation and subsequent lung injury.3
This quality-improvement project was developed as one of several strategies aimed at reducing the incidence of chronic lung disease. While there have been multiple articles addressing quality-improvement initiatives to decrease chronic lung disease such as the established Potentially Better Practices (PBP) from the Breathsavers Group of the Neonatal Intensive Care Quality Improvement Collaborative, there has been a paucity of data regarding decreasing variability of clinical practice in the neonatal literature.4 The Breathsavers group identified ‘Improved use of surfactant in the delivery room’ as an improvement with the potential to reduce chronic lung disease. To our knowledge, no studies have addressed the use of quality-improvement methods to make the process of surfactant administration more timely or decrease the variation in the timing of surfactant being given. Using this premise, we aimed our improvement strategies at the implementation of surfactant administration.
Local problem
Surfactant was routinely administered after the transfer from the delivery room to the neonatal intensive care unit. This often resulted in both a delay in the receipt of prophylactic surfactant and a wide variation in the timing of administration.
Intended improvement
Our primary objective was to use the Model for Improvement5 to develop and implement a new process to decrease variation in surfactant administration for high-risk infants within 6 months. The Model for Improvement was developed as a method for accelerating improvement. The focus of this method is setting aims, selecting measures and changes, and completing Plan–Do–Study–Act (PDSA) cycles to test and implement changes in clinical settings and quickly determine if the change is an improvement. Our goals were for surfactant to be administered at less than 20 min after delivery for infants less than 27 weeks because our current practice is to administer surfactant to all neonates less than 27 weeks and for 100% of infants less than 27 weeks to receive surfactant in the delivery room. We hypothesised that this approach would improve the timeliness of the process and reduce variation within the process.
Methods
Ethical issues
The quality improvement intervention was reviewed and granted exemption status by the Biomedical Institutional Review Board at the University of North Carolina at Chapel Hill.
Setting
The University of North Carolina Neonatal Intensive Care Unit is a 48-bed unit within a midsize academic medical centre. The maternity labour and delivery unit has 14 beds and three operating rooms located adjacent to the NICU. As an academic centre, there are attending physicians, fellows, neonatal nurse practitioners, resident physicians and medical students involved in the care of infants. Characteristics of the intensive care unit are shown in table 1. Nursing assignments are typically two patients for every one nurse, varying with the acuity of the patient. There are two respiratory therapists in the unit at all times. For routine deliveries, the neonatal delivery room team comprises at least one neonatal nurse and a resident physician or nurse practitioner. For deliveries of infant less than 27 weeks' gestation, a neonatal fellow or attending is always present in the delivery room.
Characteristics of University of North Carolina neonatal intensive care unit for 2007
Our study population included all infants less than 27 weeks' gestation born between May and November 2007. Neonates who were not born at our centre and those who were determined not to be viable (and were not intubated) were excluded from the study.
Planning the intervention
Our initial steps involved the formation of a multidisciplinary neonatal intensive care quality-improvement group of physicians, nurses, neonatal nurse practitioners and respiratory therapists to discuss project implementation. Our aim was to use the Model for Improvement method to develop and implement a more timely process of surfactant administration in the delivery room for all infants less than 27 weeks' gestational age.
The team created a process flow chart which mapped out the necessary steps for surfactant administration in the delivery room. This flow chart allowed the team to target specific processes in order to reduce the time between birth and administration of surfactant.
Prior to the intervention, the existing practice was to intubate all infants less than 27 weeks in the delivery room. After the infant was stabilised in the delivery room and transferred to the intensive care unit, surfactant was administered by a respiratory therapist. Our baseline data showed that there was substantial variability in the time surfactant was given in the unit. The team determined that time to surfactant administration could be reduced by changing the location of surfactant administration to the delivery room. This change in process flow was initially performed using a series of simulations prior to the first delivery. We identified process gaps, such as communication failures, in these simulations. Specifically, communication between the neonatal intensive care unit charge nurse and the respiratory therapist was incorporated into the process flow. Using the above information to design our study, we performed an uncontrolled, interrupted time-series study.
Our key process improvements were: (1) changing the location of surfactant administration from the neonatal intensive care unit to the delivery room, (2) adding a respiratory therapist as part of the delivery room resuscitation team and (3) training other medical staff to administer surfactant. Our outcome measures were time (min) after delivery when the initial surfactant dose was given and the percentage of infants less than 27 weeks who received surfactant in delivery room. We used a statistical process control chart6 ,7 as our primary tool to follow the outcomes of interest. A control chart uses data points representing a quality characteristic taken from the process at different times, in our case time after delivery of initial surfactant dose. Control limits of approximately three standard deviations are the standard approach used to detect statistically significant variation (also called special-cause variation when using statistical process control) in a process. By using control limits, we were able to differentiate random variability from special-cause variation for further investigation.
All attending physicians, fellows and neonatal nurse practitioners were trained to administer surfactant by the respiratory therapy team. A respiratory therapist routinely administered the surfactant during this project, but if there was not a respiratory therapist available, the fellow, nurse practitioner or attending performed this task.
Methods of evaluation
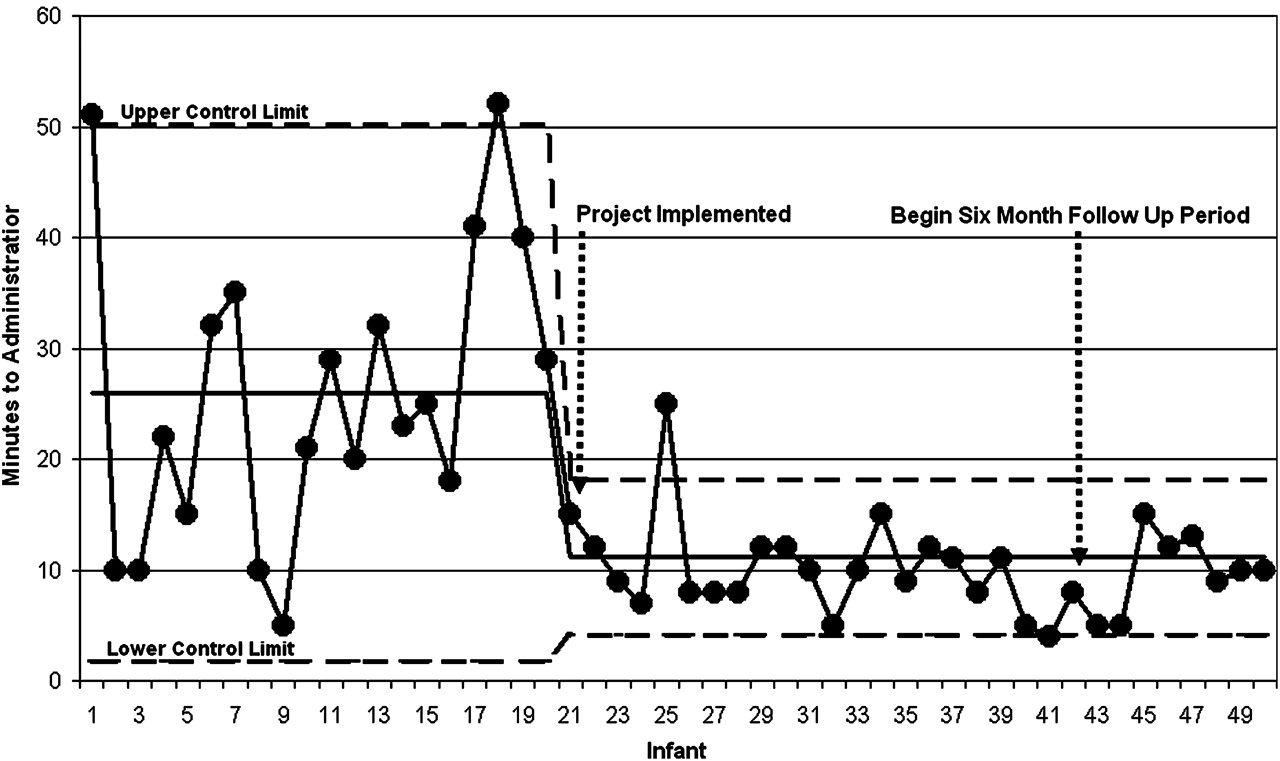
We obtained baseline data on timing of the initial surfactant dose through a retrospective chart review of a consecutive sample of twenty infants less than 27 weeks born the year prior to the intervention (figure 1; infant 1–20).

{kind=link}
Time to surfactant administration of premature infants.
We created a data-collection sheet to document the patient's gestational age, the date the surfactant was given, the identity of the provider overseeing the delivery, the time after delivery surfactant was given, if there was a respiratory therapist present at the delivery and any unexpected problems. All data-collection sheets were completed by the most senior physician at the delivery. Details of the delivery were verified for quality assurance against the delivery and admission note as a check for accuracy of surfactant administration timing.
The second phase of our initiative was to measure the sustainability of the project. Six months after the end of initial data-collection period, we performed an audit of the current system. We collected another sequential sample over a 3-month period.
Analysis
We used Microsoft Excel 2003 software (Microsoft, Seattle, Washington) for the statistical analysis. We calculated mean administration time and standard deviation of the time to surfactant delivery. To determine statistical significance, we used a two-sided unpaired Student t test with a p value of <0.05 considered statistically significant.
Results
The population for this intervention included all inborn infants less than 27 weeks between May 2007 and November 2007. All infants of this gestational age born at UNC Hospitals during the study period were included.
After our changes to the surfactant administration process, 20/21 (95%) of eligible infants received surfactant in the delivery room (figure 1; infant 21–42). The intervention led to a decrease in the time after delivery of initial surfactant dose from a mean of 26 min to 10.2 min (p=0.0004). Prior to the process initiative there was a large variation in the timing of the initial surfactant dose, with a range of 5–51 min after birth. After the initiative was implemented the variation decreased to a range of 4–25 min. The intervention led to a decrease in the variation in timing of the initial surfactant dose, with the standard deviation decreasing from 13.3 min to 4.4 min. The reduction in the variation of surfactant administration is illustrated in the control chart which shows less variation postintervention (figure 1).
The second phase of our initiative was to measure the sustainability of the project. We found that all eight infants continued to receive surfactant at less than 20 min of age, with the average time to initial dose being 10 min (figure 1; infant 43–50).
Discussion
In this study, we found that with quality-improvement methods, we were able to improve the timing of surfactant administration for infants less than 27 weeks. We were also able to reduce the variation in the timing of surfactant administration.
There are several publications that exist on the issue of quality-improvement methods that are specific to neonatology and critical care.8–10 The Breathsavers Group and the Vermont Oxford Network cite a decrease in variation as a foundational principle in quality-improvement practices.8 Our project supports the existing evidence, and also provides additional information as to how we decreased variation in our unit.
Limitations
This study has several limitations. We did not include a control group in our initiative. Thus, it is possible that some change other than our initiative resulted in the improved timing for surfactant administration and reduction in variation. However, we know of no such change that could explain this improvement. Further, as illustrated in our control charts, the improvements in time to surfactant delivery were at the exact same time as the study intervention. Another potential limitation is that our process improvement may not be applicable to other NICU settings. Although the specific steps outlined in our process improvement may not be applicable to other clinical units because of differences in surfactant administration routines, the quality-improvement process we used may be applicable to many clinical units.
Interpretation
We ascribe the success of the use of quality-improvement methods to several key factors. It is vital to include team members from all disciplines involved in the process being improved. We began our project by convening with all concerned disciplines in group discussions of the problem. We also jointly brainstormed solutions. The recognition of personnel limitations and the cross-training of staff in the administration of surfactant was a requirement for us to be successful.
Enthusiastic leaders within the various disciplines were recruited and were vital to the success of the project. The incorporation of PDSA cycles in our learning process allowed us to continually refine the process and eliminate variation. Since members of our improvement group are not always in the unit, after implementation of the process we created a very brief questionnaire to be filled out every time surfactant was given in the delivery room. This allowed us to follow-up with any difficulties or concerns in the new process.
The use of the control chart during the study helped better design our process. The infant who represented the outlier of the process (infant 25 was above the upper control limit in figure 1) was unable to receive surfactant in less than 20 min after delivery because the proper equipment was not brought to the delivery room by the respiratory therapist. The problem was addressed, and through rapid PDSA cycle change, we created a surfactant administration package that contained all necessary equipment for surfactant administration in the delivery room. Our upper control limit after implementation of our intervention was less than our goal, demonstrating that we achieved a system of high reliability in delivering surfactant to every infant less than 27 weeks within 20 min or less.
The challenge in quality-improvement work is sustaining the change. As documented in the results, 6 months after the initial project, our unit continues to maintain early surfactant administration at less than 20 min after delivery. We plan continued reviews of the data and to feedback the results to the entire staff.
Conclusions
We found that basic quality-improvement methods, using the Model for Improvement with rapid cycle (PDSA cycles) changes as well as statistical process control charts, can be successfully used to improve the timeliness and reduce the variation in surfactant administration. These methods also yielded other benefits as well. The work performed in successfully completing this project allowed us to develop an appreciation for the unique characteristics of our unit which impact quality. In successfully executing this initiative, we have improved teamwork within the unit and gained insight into our unit processes, patterns, personnel and the characteristics of our patients and families. The experience gained in transitioning our unit to surfactant administration in the delivery room will serve as an introduction to improving other processes in our unit as we continue to seek to improve the quality of care we deliver.
Footnotes
Competing interests None.
Ethics approval Ethics approval was provided by the University of North Carolina at Chapel Hill School of Medicine.
Provenance and peer review Not commissioned; externally peer reviewed.