Article Text

Abstract
Background Patients on general hospital wards who deteriorate clinically are often not recognised as needing an escalation in care, and effective interventions are delayed. This study reviews a multifaceted approach to the identification and management of these patients in a large metropolitan hospital in Auckland, New Zealand.
Strategies for change Four interventions were combined into the Physiologically Unstable Patient (PUP) programme. These were: (1) redesign of the vital sign observation chart; (2) introduction of an early warning scoring system; (3) deployment of a nurse-led rapid response team; and (4) a comprehensive ward-based education programme.
Key measures for improvement Completeness and accuracy of routine observations; actions taken in accordance with the algorithm; impact on medical emergency team callouts, cardiac arrest calls and unplanned intensive care unit admissions.
Effects of change The PUP programme was implemented in 16 wards over 15 months. Vital sign recording improved, and the PUP score became a recognised metric for prioritising patients for review. Consistent with others' experience, there was a reluctance to call for help. Raised PUP scores prompted action around 30% of the time on average. Medical emergency team calls increased significantly from a median of 27.5 calls per month to 70.5. There was no significant change in unplanned transfers to intensive care unit or in cardiac arrest calls.
Lessons learnt A multifaceted programme to identify physiologically unstable patients on general wards can be introduced and can improve the recognition of such patients, but there are still barriers to ensuring that these patients receive the extra care that they require. These systemic failings need to be investigated and addressed for real change to occur.
- Quality improvement
- early warning scoring systems
- rapid response teams
- emergency service
- hospital
- critical illness
- patient safety
- quality of care
- healthcare quality
- medical emergency
Statistics from Altmetric.com
- Quality improvement
- early warning scoring systems
- rapid response teams
- emergency service
- hospital
- critical illness
- patient safety
- quality of care
- healthcare quality
- medical emergency
Background
Over the past two decades, patient safety has been highlighted.1–7 Due to an ageing population, increased complexities of medical and surgical interventions and shorter hospital stays, patients are now generally sicker and at greater risk of clinical deterioration.8 ,9 Furthermore, this is frequently not recognised.10–12 Several factors have been identified as contributing to the failure to recognise clinical deterioration, including: not taking vital signs, not recognising physiological deterioration in those vital signs, not communicating concern and not responding appropriately where physiological deterioration has been identified.13 ,14
In response to these multiple factors, a multifaceted programme was launched. Implementation of the Physiologically Unstable Patient (PUP) programme began in June 2007. The objective of this paper is to describe the development, implementation and evaluation of the first 15 months, and to provide insights for others who may be contemplating such programmes.
Planning and development phase
The development phase took a year and involved extensive consultation with nursing and medical staff. The programme was promoted through presentations at meetings, newsletters and a webpage. A Patient Safety Committee was convened to act as a steering group for the project.
Changes introduced
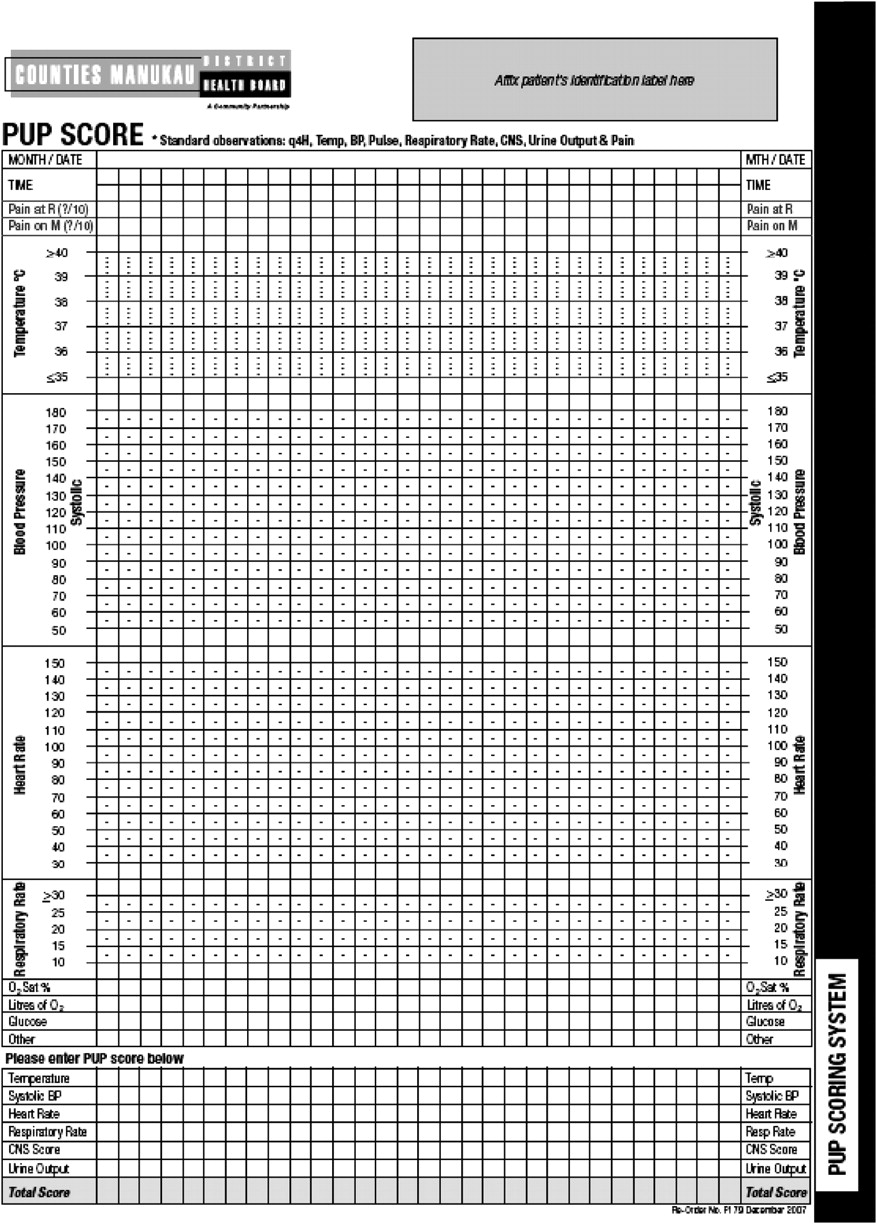
Design of a new vital sign chart
This included a number of features to facilitate the recognition of physiological deterioration. Vital signs were physically separated on the chart, enabling trends to be more easily recognised. The chart was colour-coded so that vital signs which fell outside the normal range could be easily identified. Such recordings in the ‘pink zone’ alerted the nurse to ‘stop and think’ (figure 1).

New vital sign chart.
Introduction of a modified early warning score
Our early warning scoring system (EWS) was developed from a number of sources, including a previously validated scoring system,15 and other local examples. The final scoring system was modified to reflect our patients' higher acuity and to avoid excessive false-positive triggers (figure 2). It included six vital signs: temperature, systolic blood pressure, heart rate, respiratory rate, ‘AVPU’ (alert; reacts to vocal stimuli; reacts to pain; unconscious) and urine output (catheterised patients only). Respiratory rate was chosen instead of oxygen saturation, as it has been found to be a more sensitive indicator of clinical deterioration.16 The AVPU scale was chosen, as it provides a quick and simple assessment for ward nursing staff and is used in the majority of scoring systems.17 Scores for each vital sign were determined by how far they deviated from normal and were added to derive a ‘PUP score,’ which triggered a graded response according to the PUP algorithm (figure 3). Ward nurses were encouraged to use the algorithm as a guide to their clinical judgement when managing patients.

Physiologically Unstable Patient (PUP) early warning scoring system.

Physiologically Unstable Patient (PUP) algorithm. RRT, rapid response team.
Deployment of a nurse-led rapid response team (RRT)
A number of response strategies have been described in the literature, including RRTs, medical emergency teams (MET) and intensive care outreach. Essentially all comprise a team of clinicians providing critical care expertise at the bedside to assess and manage the PUP.9 Middlemore Hospital elected to operate a two-tiered system introducing a nurse-led RRT and revitalising the existing physician-led MET.
The RRT led by the PUP Clinical Nurse Specialist operates 24 h/7 days a week and is the first port of call for nursing and junior medical staff managing patients with early signs of instability (PUP scores 2–4) or where the staff members are concerned about the patient irrespective of the score. These clinical nurse specialists have additional training and experience in managing critically ill patients.9 They attend on average 10 patients a day, mostly referred by ward nursing staff, but they also assist at emergency team callouts. Their workload comprises mostly surgical (50%) and medical (43%) patients. Their primary role when called is to assess patients and to support nursing staff in providing appropriate care to either stabilise the patient where possible or initiate a call to the MET for more advanced care.
PUP education programme
Roll-out on each ward was accompanied by an extensive 6-week education programme led by a team of resuscitation nurse specialists. The programme started 2 weeks prior to PUP implementation, with sessions on the ward to review vital sign physiology, introduce the new charts and instruct nursing staff on how to calculate a PUP score. Daily teaching sessions and intensive support on the ward continued over the 2-week period following the introduction of the new process. Over the final 2 weeks, teaching focused on troubleshooting specific problems.
The importance of the role nurses play in tracking vital signs to keep patients safe during their stay in hospital was reinforced. Meetings were held with charge nurses, senior nursing and management staff to emphasise the role of clinical leadership in achieving compliance with the programme in each ward.
Differences in communication styles often contribute to poor management of deteriorating patients.18 ,19 Nurses were therefore encouraged to use the Situation–Background–Assessment–Recommendation communication tool when contacting medical staff to request a patient review. Education for medical teams focused on the evidence for the programme with presentations made at medical forums to emphasise the importance of a timely and appropriate response to requests from nurses for patient review. For both nursing and medical staff, ongoing training and education about managing the critically ill patient on the ward was incorporated into the Advanced Cardiac Life Support training, required for both groups to maintain competency and registration.
Key measures for improvement
Monthly compliance monitoring was undertaken on each ward to determine whether staff were taking a complete set of vital signs, accurately calculating the PUP score and taking appropriate action in accordance with the algorithm. Random samples of 10 charts per ward were used to assess a 24 h period of observations. To achieve a correct PUP score, all vital signs had to be taken, scored and accurately summed. For the same period, the required number of actions based on the algorithm were counted and compared with the actual number of actions taken.
The impact on MET callouts and callouts for cardiac arrests were evaluated based on switchboard records. Unplanned intensive care unit (ICU) admissions were based on patients admitted to the ICU from the wards, excluding patients from the emergency department and postanaesthetic recovery area.
Effects of change
Sustainability: monitoring and feedback
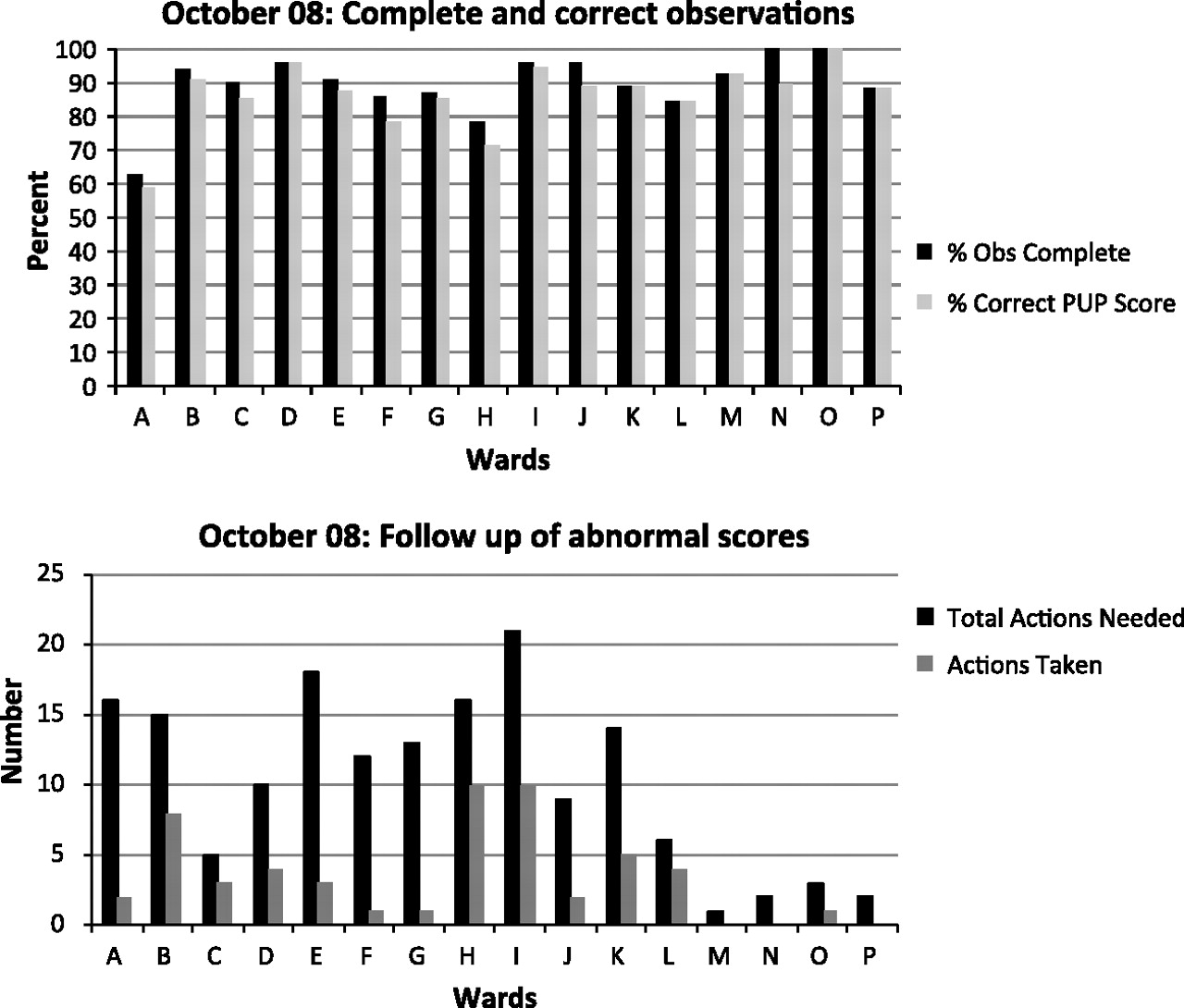
Compliance reports were sent to charge nurses each month. These included results for all wards for accuracy of vital sign recording (percentage complete and correct) and follow-up of abnormal scores (actions taken compared with required actions). See figure 4 for a ‘snapshot’ of the October 2008 result. Results averaged over all wards showed that over the latter 8 months of the implementation period, 91% of observations were complete, and PUP scores were 86% accurate. This compares with preimplementation baseline data collected over 7 weeks in two surgical wards showing that complete observations were taken 80% of the time, so there was a slight improvement. The relatively high preimplementation figure could be attributed to the high profile of the programme in the hospital prior to implementation and the fact that one of the wards had been a pilot site the previous year. Concurrent measures from our geographically separate elective surgical services site showed that complete observations were taken on average 63% of the time, which is perhaps a more realistic representation of usual practice. The average follow-up of abnormal PUP scores across all wards for the same time period was variable, occurring on average only 30% of the time.

Example of monthly compliance report to charge nurses. PUP, Physiologically Unstable Patient.
Impact on emergency response teams and unplanned ICU admissions
Although the monitoring revealed that MET calls were initiated in only 30% of patients who met the criteria, the demands on the MET (figure 5) increased significantly. MET calls increased from a median of 27.5 calls per month prior to the PUP programme to 70.5 per month with a peak of 125 calls in July 2008. Cardiac arrest calls remained steady with a median of five calls per month across the wards in which the PUP Programme was operational. Cardiac arrests in the Emergency Department, ICU and Coronary care units were excluded. We were unable to demonstrate a reduction in unplanned admissions to ICU from the wards.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Medical emergency team (MET) calls 2007–2008.
Lessons learnt
The PUP programme was phased in over 15 months on 16 wards, including general medical and surgical wards, specialist care units (Gynaecology, Plastic Surgery and Burns) and Older Adult Rehabilitation wards. The programme is also being used in the Emergency Department, ICU and Post Anaesthetic Recovery Unit to avoid transferring unstable patients back to the wards. It has had a significant effect on the calls made to the MET. We consider this increase an indication that patients who previously had not been identified as at risk of deterioration were now being seen.
In contrast to other studies,20–22 we have not been able to demonstrate an impact on cardiac arrests and unplanned ICU admissions. This could be attributed to the fact that numbers of events were small to start with, and we are still at a relatively early stage in the process. At our institution, the supply of ICU beds was markedly constrained during the study (seven-bed unit in a 900-bed hospital—2.3 beds/100 000 population), and there were often patients competing for ICU beds. This meant that few patients were transferred from the wards to ICU.
Monitoring and feedback mechanisms have successfully lifted the rate of complete vital signs taken, but there are still barriers to nurses taking action when a patient becomes clinically unstable. This is not a new problem. As Buist states in his editorial “The rapid response team paradox: why doesn't anyone call for help?”23 studies show that in patients satisfying MET criteria, a MET call is put out in only 30% of cases (identical to our experience).24 ,25 The barriers appear to be multiple, but one problem identified is the hierarchical nature of ward care—nurses are reluctant to call the MET without calling the patient's primary team first,26 and junior medical staff may not want to show superiors that they cannot cope. Certainly, any disparaging comments made by MET members live for a long time in the collective consciousness of the ward environment. In our experience, part of the problem was that with an additive EWS (instead of a single threshold MET criteria), the MET team was being called to patients earlier. They had traditionally been called when the patient was in extremis or peri-arrest, and their roles were clear. With the earlier callout, their role was more challenging.
Another barrier to the success of the PUP programme was the poor understanding of vital sign physiology among junior nursing staff and a lack of appreciation among nursing staff in general of the important role they play in monitoring patients. In some instances, this task had been delegated to healthcare assistants who have minimal training in taking vital signs and no training in their interpretation. It was also clear that good leadership from charge nurses was a key driver of success. Setting high standards of performance and supporting staff to achieve these were instrumental in achieving a good result.
We did take a number of approaches to overcome the anticipated barriers. The extensive education and promotion campaign focused on both medical and nursing staff and aimed to provide the knowledge, skills and leadership to support the programme. We were unable to deliver multidisciplinary simulation training as planned due to staff shortages and high workloads, and therefore missed opportunities to address knowledge gaps and facilitate more effective team communication.
The barriers we have described are consistent with some other descriptive accounts of introducing interventions to identify and manage unstable patients.27–32 They are also similar to those described in a recent study undertaken by the National Patient Safety Agency,13 which investigated the root causes of failing to recognise and take action for the deteriorating patient. This study revealed systems weaknesses including factors relating to communication, working conditions, education and training, and team factors.13 Improvements such as EWS, RRT and METs were designed primarily to address problems at the point of patient deterioration, but it is clear that fundamental systems issues will continue to hamper the success of such programmes unless identified and addressed. While this is now our primary challenge, we are encouraged by some modest but not insignificant benefits.
In general, there is widespread support for the programme and the importance of early recognition of deteriorating patients. The design and use of colour in the observation chart greatly enhanced the ability to identify trends. The PUP score is now used as a common metric throughout the hospital. It is used in most wards as part of the handover process to prioritise care, and between specialist units and wards to ensure the safe transfer of patients. An added unexpected benefit has been that there is now regular handover between the after-hours supervising nursing service and the RRT providing much better continuity of care for sick patients across the hospital, particularly at night. Overall, it provided an excellent framework for the identification and management of deteriorating patients. This is particularly so for new nursing graduates and foreign trained nurses who are less familiar with our systems.
Future areas for improvement
From our experience, introducing a multifaceted initiative has gone only part of the way towards improving the identification and management of unstable patients. If we are to improve the outcomes in these patients, we will need to address some of the fundamental systems issues (communication problems, the hierarchical nature of care, culture of fear, etc) that continue to limit success.
There is undoubtedly a future role for innovative information technologies to facilitate the transmission of patient information between nursing and medical teams. Refinement of the nurse-led RRT is also an area for development and will be addressed with the establishment of a new Critical Care Complex, comprising an expanded ICU and a High Dependency Unit. Advanced training is planned to enhance the team's clinical skills with the potential to expand their role in the management of critically ill patients across the hospital.
Conclusion
Few would dispute the need to identify the deteriorating patient early. EWS and RRTs are intuitively an appropriate response, but introducing such an initiative is complex. It has impacted on our traditional systems of care and fundamentally changed roles and responsibilities. We have seen positive changes in the culture of care but are yet to see this translated into better health outcomes. As we continue to develop the systems that support our EWS and RRT, our focus remains on improving the recognition and management of these vulnerable patients.
Acknowledgments
The authors wish to thank the Patient Safety Committee for their support and advice. In particular, we want to acknowledge all who contributed to the development and implementation of the PUP programme, in particular our Clinical Training and Education Team.
References
Footnotes
Funding Counties Manukau District Health Board.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.