Article Text

Statistics from Altmetric.com
My grandfather was a general practitioner in a small town in the USA in the mid-20th century. His medical team consisted of himself and a nurse (who was also my grandmother). He even served as his own pharmacist. In stark contrast, the team in my primary care practice consists of my physician partners, several trainees, nurses, medical assistants, referral coordinators, pharmacists, the subspecialists and their teams, home health nurses and therapists, and more. Such large and disconnected teams can provide comprehensive care for complex and chronic illnesses, but when they malfunction, they can harm patients.1
Teams are larger and more dispersed in time and space, and there are now many more types of teams. They vary from teams whose members repeatedly work together over many years (eg, highly specialised cardiac surgery teams) to teams that are formed quickly and temporarily to resuscitate a patient. Teams are also formed for quality improvement (QI) projects, and they may work together for a few months or a few years. Unfortunately, education for healthcare professionals in most parts of the world still assumes that healthcare teams are like those during my grandfather's time. Professional school and continuing education curricula have not been updated to teach the skills needed to work effectively in these varied teams.
To fill this gap, team training programmes that address teamwork and communication for healthcare providers are increasing in number, becoming more heterogeneous and being evaluated more frequently.2 Here I propose three general approaches that have been developed to improve teamwork in healthcare, and I discuss their strengths, weaknesses and which of their aspects require further research (table 1). Finally, I suggest that these approaches complement one another, and by purposefully exposing care givers to them during their training and careers, we can eventually improve teamwork and patient outcomes.
Three approaches to improve teamwork in healthcare
Comprehensive and generic team training
Team training in healthcare initially took its cue from successes in commercial aviation and the military. Researchers like Robert Helmreich and Eduardo Salas helped the healthcare profession appreciate the potential for training based on Crew Resource Management (CRM). CRM focuses on communication skills such as briefings, speaking up, monitoring and repeating back critical communications and information.3 TeamSTEPPS, developed by the Agency for Healthcare Research and Quality, is the best example of a comprehensive and generic curriculum applicable to most providers and sites of care.4 Similar curricula have been provided by private consultants—often individuals with CRM training experience in commercial aviation—for many years.5 Entire staffs from patient care areas may be pulled from clinical activities to participate in training that may last 1–2 days. The TeamSTEPPS instructors' manual is a 4-inch binder of paper, DVDs and handouts. Thus, the training is extremely time intensive and can result in a large financial cost (shutting down operating rooms) and opportunity cost (these care givers and quality leaders could have used the time to pursue other initiatives). TeamSTEPPS is derived from a substantial body research, but most of it is not related to healthcare and it has not been proven to reduce harm to patients. Most of the research on generic versions of TeamSTEPPS and similar curricula have relied upon intermediate outcomes reported by participants (ie, attitudes about teamwork) or used study designs that make it difficult to determine causality.6 Another limitation is that by itself the curriculum does not account for organisation-specific characteristics, a feature believed to be important for team training programmes.3 Nevertheless, the training has high face validity, is unlikely to harm patients, has been endorsed by expert groups and malpractice insurers in the USA and can be applied to multiple types of care givers. Also, as consensus grows for introducing team training into medical and nursing schools,7 programmes like TeamSTEPPS may serve as their foundation.
Brief and task- or activity-specific team training
A second approach has been to develop brief and focused team training curricula for specific healthcare tasks or activities. Examples include team training for resuscitations,8 surgery,9 10 handoffs among care givers11 and daily rounds.12 13 Research on activity-specific team training is just beginning to show benefits for patients,9 and it may at least temporarily change behaviour. Our assessor-blinded randomised controlled trial of a 2-hour team curriculum for neonatal resuscitation found that it improves team behaviours and reduces the duration of neonatal resuscitations in a high-fidelity simulator.8 Interestingly, even a remarkably brief 10-minute training session can improve leadership skills in a simulated environment.14 Like the comprehensive and generic curricula, this approach also lacks substantial proof of its ability to improve patient care. Another limitation is that training for one task or activity will have limited generalisablity. Thus, there will be a need to develop a large number of customised team training programmes. Future research may focus on even more discrete activities and procedures like intubation, cardiac catheterisation or chest tube insertion. Methods such as task analysis will be useful to parse the precise types of communication needed to improve care, and simulation labs can be used to test the effectiveness of task-specific training.
QI interventions that require teamwork
Third, good teamwork is required for QI to be successful. QI is not just about changing the workflow or adding tools to help care givers do the right thing. Teams must form to lead the QI effort, and improved teamwork and communication by front-line care givers are often required to make the changes that lead to improved patient outcomes. For example, the WHO surgical safety checklist researchers reported more than 30% reduction in postoperative complications and mortality after checklist implementation.15 This improvement in outcomes is not fully explained by increased compliance with items on the checklist (eg, antibiotic administration to prevent wound infections). Instead, it is likely that the checklists and the overall QI efforts also improved teamwork during surgery.15 16 Simple acts required by the checklist like introductions among team members and discussing concerns about a procedure may markedly improve teamwork. This highlights the fact that quality interventions not explicitly about teamwork may nevertheless improve teamwork and have better results for patients than interventions and programmes that focus solely on teamwork (like those above in the category of team training for specific tasks and activities).
QI professionals have of course known for decades that most interventions to improve care must be coupled with efforts to improve teamwork on the front lines; it is an innate characteristic of improvement efforts. However, the impact of the QI effort on teamwork has been underappreciated. That impact is now easier to recognise when compared with the more recent team training efforts noted above, which have yet to show such dramatic improvement in patient outcomes. Other examples of successful QI efforts that require and probably improve teamwork include efforts to prevent catheter-related blood-stream infections17 and ventilator-associated pneumonia,18 and to improve the care of patients with chronic disease.19
The path forward: teamwork among approaches to improve teamwork
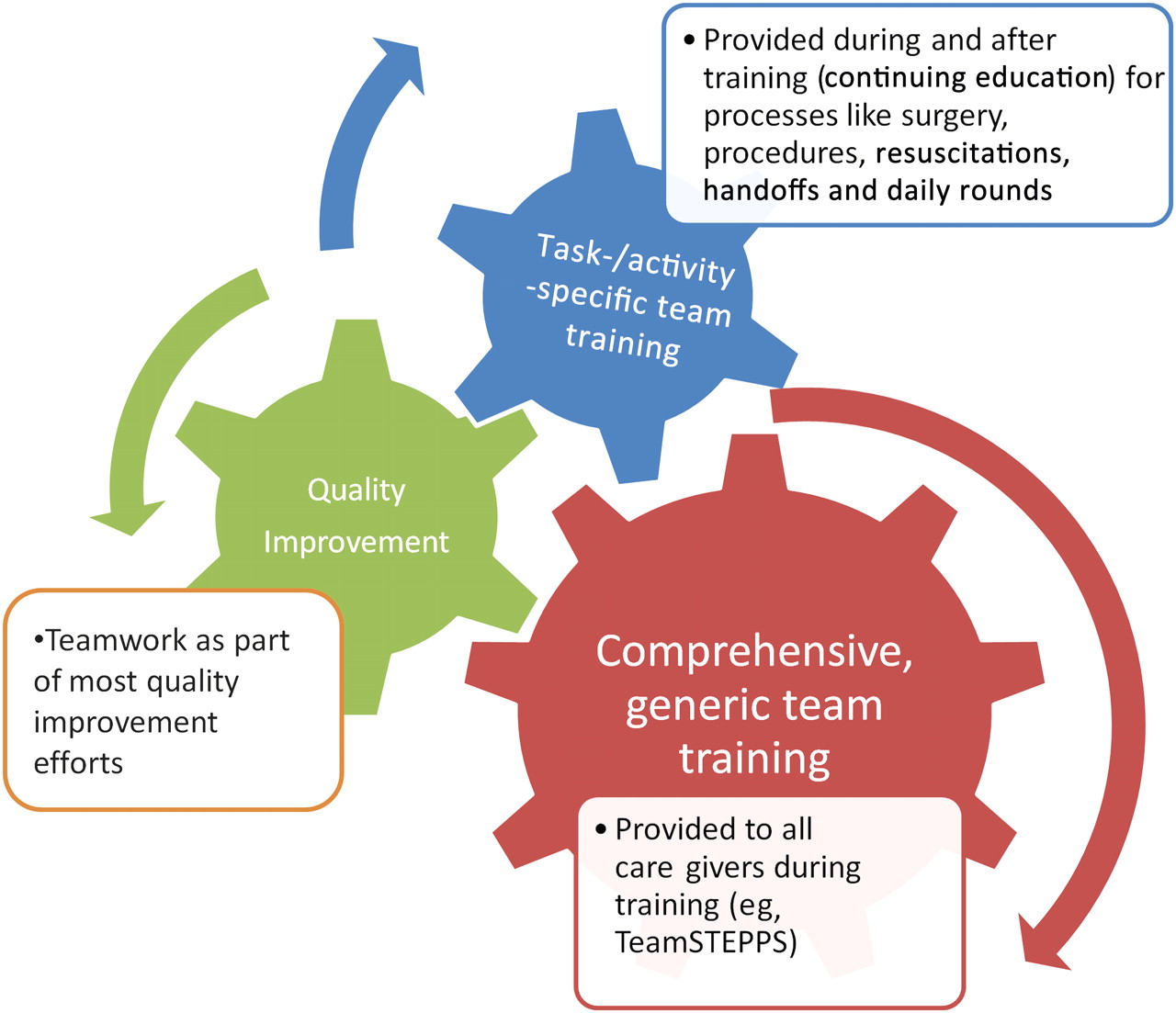
These three approaches (comprehensive and generic curricula, brief and task-specific team training and traditional QI efforts) have strengths and weaknesses that lend themselves to specific future uses and development needs (figure 1, table 1). A cross-cutting issue for all approaches is the variable strength of the research evidence to support the interventions' ability to change behaviour and improve care. Most people would not argue against the concept of improving teamwork and communication, but the effectiveness of various training programmes will vary. Given their potential high cost and widespread dissemination, it is important to conduct the most rigorous research possible to determine which ones are most effective. The generic and comprehensive approach embodied by TeamSTEPPS probably needs no more development or assessment other than updates to account for new research findings. Some institutions will continue to find it valuable for 1–2-day training sessions of large groups of personnel, especially if it is customised somewhat for specific teams and organisations (eg, operating teams in the Veterans Healthcare Administration).9 Perhaps a more important role for TeamSTEPPS-like programmes will be as the foundation for medical and nursing schools' teamwork-related curricula.6 With that foundation, trainees will be better prepared for their exposure to brief, task-specific team training for resuscitations, surgeries, handoffs, chest tube insertion and many other activities. Some task-specific team training will also contribute to career-long continuing education for teamwork as care givers periodically recertify for activities such as neonatal resuscitation. Other opportunities for team training in continuing education should be sought out as well.20 These two teamwork approaches will then make healthcare providers better equipped to join QI efforts—either as leaders or as the care givers implementing change—which have always relied on good teamwork and which probably have the greatest opportunity to improve processes and outcomes of care.

{kind=link}
Career exposure to team training for healthcare professionals.
My grandfather's days of the simple physician and nurse team are ending in many countries, but as team training curricula mature and join with traditional QI efforts, we should see marked improvements in teamwork and better care for patients. Future efforts should focus on recognising the complementary nature of comprehensive and task-specific team training, and how both of them can better prepare care givers to participate in QI efforts.
References
Footnotes
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.