Article Text

Abstract
Background Teamwork—that is, collaboration and communication—is an important factor for safe healthcare, but professions perceive the quality of teamwork differently.
Objective To examine the relationship between simulation-based team training (SBTT) and different professions’ self-efficacy, experienced quality of collaboration and communication, perceptions of teamwork and safety, together with staff turnover.
Methods All staff (n=151; physicians, nurses and nurse assistants) in an intensive care unit (ICU) at a university hospital were systematically trained over 2 years. Data on individual self-efficacy were measured using the self-efficacy questionnaire; the experienced quality of collaboration and communication, teamwork climate, safety climate and perception of working conditions were sampled using the ICU version of the safety attitudes questionnaire (SAQ). Staff turnover and sick leave was measured using the hospital's staff administration system for the intervention ICU and a control ICU in the same hospital.
Results The perception of safety differed between professions before training. Nurses’ and physicians’ mean self-efficacy scores improved, and nurse assistants’ perceived quality of collaboration and communication with physician specialists improved after training. Nurse assistants’ perception of the SAQ factors teamwork climate, safety climate and working conditions were more positive after the project as well as nurses’ perception of safety climate. The number of nurses quitting their job and nurse assistants’ time on sick leave was reduced in comparison to the control ICU during the study period.
Limitations Results for SAQ factors must be interpreted with caution given that Cronbach's α and inter-correlations for the SAQ factors showed lower values than benchmarking data.
Conclusions All team members benefited from the SBTT in an authentic composed team, but this was expressed differently for the respective professions.
- Team training
- Crew resource management
- Critical care
- Safety culture
- Simulation
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/3.0/ and http://creativecommons.org/licenses/by-nc/3.0/legalcode
Statistics from Altmetric.com
Introduction
Improving patient safety is a challenge for healthcare. Teamwork has been recognised as an important factor for patient safety, and staff perception of teamwork is related to the quality and safety of care.1–3 Healthcare professions have discrepant attitudes about teamwork: physicians seem more pleased than nurses with nurse–physician collaborations and communication, which can be attributed to traditional hierarchy within the team.4–9 Different perceptions of teamwork and communication might also reflect a lack of understanding among team members regarding team goals, teamwork structure and teamwork processes. Research from flight–combat simulations shows that shared team mental models relate positively to team performance.10 Risk-adjusted morbidity of surgical patients correlated with the experienced quality of collaboration and communication in a study on surgical teams.11
There is support for team training programmes being effective for important team processes such as communication and coordination and outcomes; that is, knowledge, skills, attitudes and perceptions.10 Structured interventions targeting teamwork have shown a relationship with improved teamwork and safety climate.12–14 In addition, there are results describing an association between patient outcome and the perception of teamwork and safety climate.15–17 Teamwork climate and safety climate are two of the six factors in the safety attitudes questionnaire (SAQ), one of the most validated questionnaires for use in intensive care units (ICU), also comprising assertions about the experienced quality of collaboration and communication between professions.18
Restructuring work processes towards a team-based approach may improve not only the quality and safety of patient care but also staff wellbeing.19 Teamwork and safety climate of good quality has a positive effect on nurses’ intent to stay.20
Training in team processes such as communication has also been shown to increase self-efficacy.21 Self-efficacy is a belief in one's personal capability to perform given actions.22 Those with high self-efficacy in a specific task are more likely to make more of an effort and sustain effort longer than those with low self-efficacy.23 Self-efficacy is also an important prerequisite for learning and a predictor for performance.22 Medical simulation training can improve individual as well as team self-efficacy.24
In 2005 the staff and management of the ICU at Karolinska University Hospital, Huddinge, Sweden, identified teamwork and communication as areas for improvement. In order to improve inter-professional collaboration, a programme was initiated in which the major intervention was in-situ simulation-based team training (SBTT). The initiative opened an opportunity to study teamwork climate in response to a systematic and structured intervention targeting all interdisciplinary staff in an ICU.
This SBTT project was also evaluated in a qualitative study by Sandahl et al,25 who performed observations and interviews critically reviewing the content of the training, the process of putting the programme into practice and final outcomes. They also covered contextual factors related to the organisation.
The primary goal of this study was to explore differential individual training effects for physicians, nurses and nurse assistants on self-efficacy and experienced quality of collaboration and communication between professionals. As a secondary aim, we examined training effects on organisational factors; that is, teamwork climate, safety climate, perception of working conditions, staff turnover and sick leave.
Methods
Participants and setting
Preparation for the project started in 2006 with the collection of data for sick leave and staff turnover and ended in 2010 in order to include the whole study period. The complete ICU staff—that is, physicians (specialists and residents in anaesthesiology and intensive care), nurses and nurse assistants—was scheduled for 1 day of mandatory SBTT during the training period November 2007 to November 2009. Participation in the evaluation study was voluntary. The participants were given a personal code to label their questionnaire for confidentiality. The institutional review board (Regionala etikprövningsnämnden i Stockholm) approved the study and informed consent was obtained from all participants.
All but one of those trained (n=152) agreed to participate in the study. In total, 151 persons (119 women; 79%) participated in the study. Fifty-one physicians (30 women; 59%), 75 nurses (64 women; 85%) and 25 nurse assistants (all women) aged between 20 and 62 years participated. The response rate for those answering both before and after the training was 67% (n=102) for self-efficacy (75% women) and 75% (n=114) for SAQ (72% women).
The in-situ SBTT was carried out in a general ICU, the sole ICU for both paediatric and adult patients at Karolinska University Hospital, Huddinge. During the daytime physicians are responsible for up to five patients depending on the care given and the physician's training level. Nurses work bedside with one or two patients, and nurse assistants with one to four patients depending on patient condition and the number of patients. In 2005 staffing was reorganised. Nurse assistants were replaced by nurses, which decreased the patient/nurse ratio to one patient per nurse during the daytime and one to two patients during evening and night shifts.
Simulation-based team training
The training started with 4 h of interactive seminars concerning safe teamwork during times of stress, in which the main learning objectives were knowledge and understanding of safety in complex organisations, errors due to human fallibility in a stressful environment that can be avoided and safety tools for stress management. The introductory seminars were repeated 16 times during 2007–9 for groups of six to 22 participants.
In-situ simulator-based team training
The seminar was followed by 1 day of SBTT with a team comprising six persons; one or two physicians, two or three nurses and one or two nurse assistants. The interval after the seminar for each team was between a few days to some weeks. Training sessions were repeated 28 times. The SBTT was carried out in an authentic and ordinary equipped intensive care single-bed room where a high-fidelity patient simulator (human patient simulator, METI Inc., Sarasota, Florida, USA) replaced a real patient. Five standardised scenarios were pre-programmed: urosepsis, pneumothorax, aortic rupture with re-bleeding after operation, anaphylaxis due to administration of a drug in the ICU and hypovolaemia due to ruptured spleen. Each team experienced three to four of the scenarios.
The training method used was structured team coordination training, as described earlier, and was carried out by a physician who specialised in anaesthesia and intensive care and a nurse who specialised in intensive care, both with many years’ experience in crew resource management training at the Centre for Advanced Medical Simulation and Training.26
The SBTT included familiarisation with the patient simulator, demonstration of a scenario by the trainers underlining the targets for training (box 1) and repeated scenarios with structured debriefing.27 ,28 The strategy for collaboration used during SBTT, the all team members’ behaviour (A-TEAM) programme, is focused on a rational use of available competence in order to provide safe, effective patient care.29 The roles within the team, how to support each other and communicate in order to recognise all competence in the team was discussed according to the targets for training (box 1).
Targets for training
Behaviour targets (1–5)
-
Take a team member role
-
Gather information and communicate
-
Contribute to a shared understanding of the situation
-
Make collaborative decisions
-
Coordinate and execute tasks
Clinical performance (6–7)
-
Time to call for help in seconds
-
Frequency of top-to-toe examinations
-
Frequency of team sum-ups (n×h-1)
Medical target (8)
-
Stabilise the vital functions of the patient
Measurements
Self-efficacy
Self-efficacy is the self-reported belief in the ability to understand and manage an emergent clinical situation. A four-item questionnaire was used in which each proposal was rated on a seven-point Likert-type scale from ‘not true at all’ (1) to ‘very true’ (7).30 A self-efficacy score was calculated as the mean value of these four items. The self-efficacy questionnaire was distributed twice to the participants, first at the introductory seminar and a second time when the SBTT had been completed for all participants.
Safety attitudes questionnaire
Data were collected using a Swedish translation of the SAQ, ICU version.18 The SAQ is a 64-item validated instrument estimating healthcare workers’ perceptions of safety climate and has been described elsewhere.18 Translation was done according to the International Society for Pharmacoeconomics and Outcomes Research guidelines.31 The SAQ was used twice together with the self-efficacy questionnaire.
Experienced quality of collaboration and communication between professionals
The SAQ included one item about the experienced quality of collaboration and communication between respondent and consultants, residents, nurses and nurse assistants, respectively. Each item was answered using a five-point Likert scale from ‘very low’ to ‘very high’.
The SAQ factors
Each item was answered using a five-point Likert scale from ‘strongly disagree’ to ‘strongly agree’. Groups of four to seven items provide six factors: teamwork climate, safety climate, job satisfaction, stress recognition, perceptions of management and perception of working conditions. Although SAQ data are ordinal, the usual method—also used in this study—is to calculate and present SAQ data as a mean percentage (SD).32 The scores were reversed for all negatively worded items and the scale was converted to a 0–100% scale. The ordinal data thus corresponds to following n% with the conversion: disagree strongly, 0%; disagree slightly, 25%; neutral, 50%; slightly agree, 75%; and strongly agree, 100%.18
Staff turnover and sick leave
The Department for Human Resources provided anonymous yearly data for staff turnover and sick leave for the ICU studied together with data for a reference ICU at Karolinska University Hospital, Solna, Sweden. The reference unit has about the same level of burden of care. Data were not possible to obtain for physicians in the ICU as these were inseparable from the complete department of anaesthesia and intensive care.
Staff turnover was calculated as the number of employees quitting their job during the fiscal year divided by the average number employed the same year. Sick leave is presented as a percentage of sick leave out of scheduled working time.
Design of the study
The design of this exploratory study, including the flow of data sampling and lost data, is presented in figure 1.

Flow chart for the study. All except one trainee agreed to participate in the study (n=151). Matched pre/post safety attitudes questionnaire (SAQ) and self-efficacy questionnaires were obtained from 114 and 102 participants, respectively. ICU, intensive care unit.
Power calculation
An improvement of 10% in three of the factors of SAQ, teamwork climate, safety climate and working conditions would be of clinical importance.13 ,33 As the present Swedish translation of the SAQ has never been used before, we used preliminary data for mean and SD from our first sampling together with data from other studies for perception of safety climate, teamwork climate and working conditions for a conservative power calculation. We assumed a mean value of 55 and a SD of differences of 15.5, which resulted in a sample size of 65, which would have 80% power to detect a difference in means of 5.5 with a 0.05 two-sided significance level.
Statistical analysis
Internal consistency was calculated by Cronbach's α for self-efficacy and for the six factors of SAQ. Pearson correlation coefficients were used to measure the association between the six factors of SAQ.
A two-way repeated measures analysis of variance (ANOVA) was used to analyse the improvement effect and the difference between the three professions; that is, physicians, nurses and nurse assistants. In addition, post-hoc contrasts were performed to estimate the improvement effect for each of the professions. In the case of significant interactions in the ANOVA, simple effects were examined; that is, effects of one factor while holding the other factor fixed. Due to the uneven distribution of sexes within the professions studied, we performed analyses of sex differences for the variables self-efficacy and SAQ factors using a three-way repeated measure (ANOVA).
The data for staff turnover and sick leave were analysed by multiple regression analyses with the independent variables of time, professions, units and interactions with time. Results are presented as regression coefficients and 95% CI; p<0.05 was considered statistically significant.
Results
Self-efficacy
Internal consistency
The Cronbach's α for self-efficacy was 0.89 before training and 0.90 after the project.
Data
Data for perceived self-efficacy were analysed only for questionnaires that could be matched before training and after the project (n=102; table 1). There was no difference between the level of scores of self-efficacy before training and after the project between sexes (not shown). There was a significant interaction between increase and sex (p=0.022), displaying a larger effect for men. Each sex was analysed separately using a simple effect test; both women's (p=0.016) and men's (p<0.001) scores improved. The effect for women was 0.21 (95% CI 0.039 to 0.371) and for men 0.59 (95% CI 0.308 to 0.876).
Self-efficacy (1–7) and SAQ factors (%)
The SAQ
Experienced quality of collaboration and communication with professionals
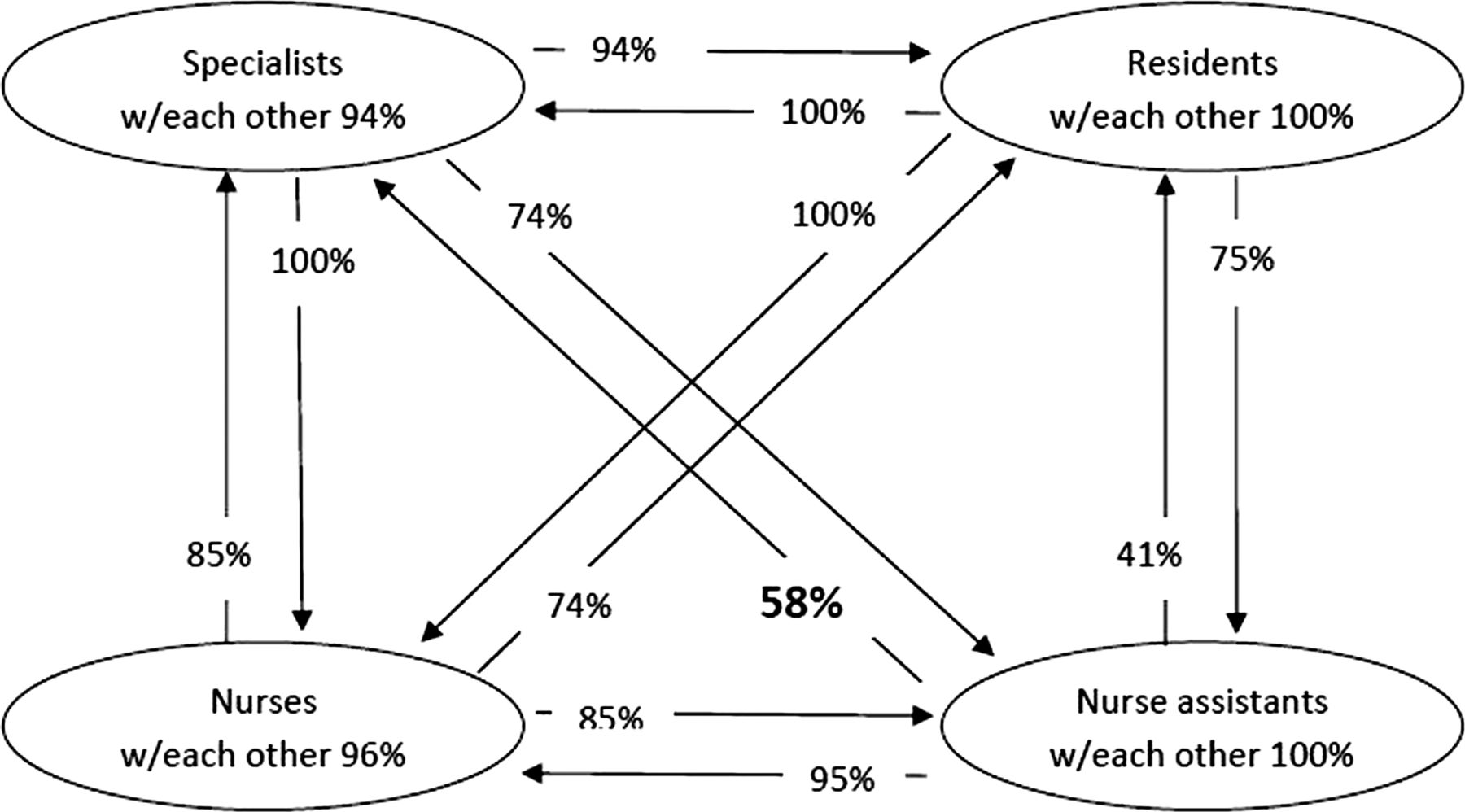
The percentage of each profession reporting ‘high’ or ‘very high’ quality of collaboration and communication between themselves and the professionals in the ICU is shown in figures 2 and 3.

Percentage of each profession reporting ‘high’ or ‘very high’ level of collaboration/communication with other members of the intensive care team before simulation-based team training.

{kind=link}
{kind=link}
{kind=link}
Percentage of each profession reporting ‘high’ or ‘very high’ level of collaboration/communication with other members of the intensive care team. Compared to data before simulation-based team training (figure 2) the only difference was registered for nurse assistants who reported a better collaboration/communication with specialists (58% vs 41%, p=0.04).
SAQ factors
Internal consistency
The Cronbach's α for each factor of the SAQ showed values from 0.43 to 0.71 before and 0.61–0.75 after the project. Each SAQ factor requires all items in the factor to be complete, disqualifying all items with one missing value, which explains the disparity in numbers (76–109).
Inter-correlation
The inter-correlations between the SAQ factors showed a fair to moderate relationship (0.25–0.55), with the exception of the factor stress recognition in which the relationship with most of the other factors was very weak.
SAQ data
Data for the SAQ factors were analysed for matched questionnaires; 114 participants contributed with answers both before SBTT and after the project (table 1). The missing values in the SAQ factors were 1.5%, and the answering alternative ‘not applicable’ was chosen in 2.7% of responses to all items. There was no difference between the level of scores of SAQ factors before SBTT and after the project between sexes (not shown).
Staff turnover and sick leave
Between 14% and 24% of the nurses in the intervention ICU left their jobs each year during the fiscal years 2006–10. Corresponding data for nurse assistants were 0% and 6%. In the control ICU 7–14% of the nurses left their job each year and 4–27% of the nurse assistants over the same 5-year period.
Nurses in the intervention ICU quitting their job were reduced by a mean of 2.2% per year (95% CI −0.05 to 0.01, p=0.06) in contrast to an increase by 1.7% per year (95% CI 0.00 to 0.03, p=0.04) in the control ICU during the study period. The yearly changes in nurses quitting their job was significantly different between the two wards, p=0.006. No significant change for nurse assistants was observed.
Nurses in the intervention ICU were on sick leave 6–9% of the working time each year during the fiscal years 2006–10, while nurse assistants were on sick leave 12–29% of the working time. Corresponding data for the control ICU were 5–9% sick leave for nurses and 8–11% for nurse assistants. There was a general reduction in sick leave for nurses of 0.74% per year (95% CI −1.14 to −0.35, p=0.003). Univariate analysis of the two groups of nurses from the two ICU did not reveal any difference (p=0.24) in yearly sick leave.
Nurse assistants in the intervention ICU showed a significant reduction in sick leave over the 5-year period, estimated reduction was 4.85% per year (95% CI −7.70% to −2.01%, p=0.012). Nurse assistants in the control ICU did not show any change, 0.24% per year, (95% CI −1.39% to −1.88%, p=0.66). Univariate analysis showed a significant difference (p=0.003) in the change in yearly sick leave between nurse assistants in the two ICU.
To summarise the results shown in table 1 and in the text above:
-
Physicians experienced improved self-efficacy after the project in contrast to their experience of quality of collaboration and communication between professionals. They scored higher than nurses in safety climate before SBTT. Their scores for the SAQ factors did not improve after the project.
-
Nurses’ self-efficacy improved after the project. Their experienced quality of collaboration and communication between professionals did not change. They scored significantly lower than physicians and nurse assistants in safety climate before SBTT. Their scores for safety climate increased after the project and ended on a par with physicians’ perceptions.
-
Nurse assistants’ perceived self-efficacy did not improve significantly. Their experienced quality of collaboration and communication with physicians improved. They showed about the same level as physicians before SBTT in scoring of teamwork climate, safety climate and working conditions. In contrast to the other professions, they improved in scores for teamwork climate, safety climate and working conditions, matched by a reduction in sick leave.
Discussion
All staff in an ICU underwent systematic SBTT during a 2-year project period. The SBTT was focused on a rational use of available competence in order to provide effective patient care. Our findings confirm earlier findings on the differences between professions regarding experiences of collaboration and communication as well as perceptions of teamwork and safety climate. In addition, we noticed a diverse response among professions in association to the SBTT regarding self-efficacy, experienced quality of collaboration and communication and perceptions of teamwork, safety and working conditions.
The study's particular strengths
The strength of this study is the well-defined training method, and a multilevel and multimodal evaluation.34 ,35 The SBTT was designed, implemented and evaluated according to the 11 best practices defined by Weaver et al.27 The entire staff was trained and contributed with data. Physicians, nurses and nurse assistants who worked in the same unit were trained together and served as their own controls.
Relation to other evidence
Self-efficacy
Physicians’ and nurses’ self-efficacy in the ability to understand and manage an emergent clinical situation was stronger after the project, and men showed a larger improvement. The increase in self-efficacy is in agreement with Ammentorp et al,21 who found that communication skills training improved self-efficacy among nurses and physicians.
In contrast, nurse assistants did not show any enhancement in self-efficacy after the project.
Experienced quality of collaboration and communication with professionals
Nurse assistants reported that the quality of collaboration and communication with physicians was significantly better after the project. A qualitative study using observations and interviews describing the present project reported that the participants stated they had an increased awareness of the importance of effective communication for patient safety.25 Nurse assistants’ reactions to team SBTT have not previously been described in the literature, as far as we know.
SAQ factors
Our response rate concerning the SAQ factors and number of missing data are in accordance with others.18 ,36 Results for SAQ factors must be interpreted with caution given that Cronbach's α and inter-correlations for the SAQ factors showed lower values than benchmarking data.
The mean values for the perception of safety climate in the present ICU—56% before and 63% after the project—were lower than in ICU in the UK, New Zealand and the USA—approximately 67%.18
The perception of the safety culture in Swedish pharmacies showed higher values (approximately 80%) in all factors, with the exception of stress recognition.37 The safety culture seems to correspond more to workplace than country.
Discrepant attitudes about teamwork between physicians and nurses are in agreement with a number of studies from ICU4 ,6 and other areas.5 ,8 ,38–40 This was further extended to nurse assistants in the present study, to our knowledge not described previously in the literature. Their perceptions of teamwork climate, safety climate and working conditions in the ICU were more positive. The improved perception of teamwork after medical team training or other team process-oriented interventions is in agreement with others.13 ,27 ,41–43
The scores for safety climate also improved for nurses in our study. Physicians did not change in scores for the SAQ factors after SBTT. This is in line with the findings of Khoshbin and collaborators44 that the safety climate improved among nurses but not among physicians after the implementation of an operation room briefing safety initiative. Carney et al43 found a positive change in teamwork climate for both physicians and nurses after implementation of a medical team training programme in 101 hospitals.
The scores for stress recognition for nurses and nurse assistants decreased in our study. The interpretation of these data is difficult. Most intervention studies present data only for teamwork climate and safety climate, making a direct comparison impossible. It has been discussed whether this should actually be a part of the SAQ or not.45
Carney et al40 found sex differences for the factor teamwork climate in the operating room, a finding we could not confirm in the present study.
Staff turnover and sick leave
We found an indicative (p=0.06) reduction for nurses quitting their job at the intervention ICU. This is in agreement with a study by Timmel et al,41 who found improvements in teamwork climate, safety climate and nurse turnover rates in a unit after implementing a safety programme.
Nurse assistants in the intervention ICU decreased their sick leave from 28% in 2006 to 12% in 2010. Poor teamwork has been associated with sick leave of hospital physicians, but has not previously been described for nurse assistants.46 However, this finding should be interpreted with caution (see Limitations section).
Limitations
From a patient safety point of view, a major limitation is that this study did not include a follow-up period documenting measures that sustain positive achievements in collaboration and communication.
Several projects were run in parallel at the unit to improve inter-professional collaboration; therefore all findings in this study cannot be attributed to the effect of the SBTT project alone. On the other hand, the systematic SBTT, using the A-TEAM programme, was the only major project involving all professions, including nurse assistants.29
Due to reorganisation the year before the project started, nurse assistants had lost a number of their professional colleagues. Nurse assistants still employed during the project may have been more positive with an improved perception of working conditions and a decrease in sick leave.
Scale psychometrics for the SAQ did not reach the desired levels of 0.7; although lower than benchmarking data, patterns were similar.18 The translation of the SAQ was done by a professional, but as Waterson et al47 emphasise, appropriate validation is important before surveys are used in a different context; for example, geographical or healthcare, depending on which they were developed for. Further refinement of the Swedish SAQ ICU version is needed. As a consequence, results for the SAQ factors must be interpreted with caution; the experienced quality of collaboration and communication is probably more reliable in this study. The changes in this study are indeed significant, but are small and the exact level of clinical significance for each variable is unknown. This makes a multilevel and multimodal evaluation seem even more reasonable and conclusions can be strengthened if different end points concur.48
Interpretation
An analysis of the inter-professional relationships in healthcare, using power analysis,49 social role theory or the principle of least interest,8shows that expectations about the relationship are different and depend on the level of hierarchy: being high in the hierarchy means being more satisfied with the relationship than subordinates. The strategy for collaboration used in this project, the A-TEAM programme, is primarily focused on meeting patient needs; that is, the team has the obligation to use available competence in order to cure, relieve and care for the patient without harm. As such, the SBTT recognises all team members, lowers hierarchy and re-models relationships within the team. After SBTT, nurse assistants and nurses will be better acknowledged than traditionally, an acknowledgement that most certainly explains their greater appreciation of teamwork after the project. This explanation is strengthened by the interviews in the study by Sandahl et al,25 in which both the nurse manager and some nurses suggested that the work roles of the nurses and the nurse assistants had been dealt with during the SBTT.
Physicians and nurses, often being the leaders, have the benefit of increased support of the followers taking a more active role due to the SBTT, questioning the traditional pattern of collaboration and communication. They thus feel more confident in how to handle the acute situation, in this study noticed as increased self-efficacy. SBTT might contribute to a more common understanding in the team of goals, teamwork structure and teamwork processes—that is, the creation of a common community of practice.
Conclusions
In-situ systematic SBTT of the entire ICU staff, with a high-fidelity patient simulator, might contribute to improved self-efficacy, experienced quality of collaboration and communication between professions and perceptions of teamwork, safety and working conditions. Nurses, nurse assistants and physicians responded differently to SBTT.
Our conclusion is that all team members benefited from the SBTT in an authentic composed team, but this was expressed differently for the respective professions.
Acknowledgments
The authors acknowledge the skilled statistical assistance of Elisabeth Berg, BSc, Department of Learning, Informatics, Management and Ethics, Karolinska Institutet. They also greatly thank Petter Westfelt, MD; Mats Hedsköld, RN; Ms Annika Yamini, nurse assistant, all at the Center for Advanced Medical Simulation and Training and Lars-Gunnar Andersson, BSc, at the Department of Biomedical Engineering for their enthusiasm and professionalism during the team training. Anitta Nieminen, nurse manager; Leif Tokics, MD, PhD; Inga Tjäder, MD, PhD and Patrik Rossi, MD, PhD at the Department of Anaesthesia and Intensive Care as well as Helena Gustafsson, PhD student, Medical Management Center, Karolinska Institutet, are also gratefully acknowledged for their support during the planning and implementation of this study.
References
Footnotes
-
Contributors LM: Contribution to study conception and design, acquisition of data, analysis and interpretation of data, drafting of manuscript, critical revision and final approval of the version to be published. LH: Contribution to study conception and design, analysis and interpretation of data, drafting of manuscript, critical revision and final approval of the version to be published. CS: Contribution to study conception and design, critical revision and final approval of the version to be published. LFT: Contribution to study conception and design, analysis and interpretation of data, drafting of manuscript, critical revision and final approval of the version to be published. CJW: Contribution to study conception and design, acquisition of data, analysis and interpretation of data, drafting of manuscript, critical revision and final approval of the version to be published.
-
Competing interests None.
-
Funding This study was fully supported by research grants from Karolinska Institutet, the Stockholm County Council, Marianne and Marcus Wallenberg Foundation and by the project Innovation Implementation Systems for Better Health (application no. A2007-032), which is managed by VINNVÅRD, a joint research foundation established by the Swedish Ministry of Health and Social Affairs, the Swedish Association of Local Authorities and Regions, the Swedish Governmental Agency for Innovation Systems (VINNOVA), and the Vårdal Foundation.
-
Ethics approval The institutional review board (Regionala etikprövningsnämnden i Stockholm) approved the study and informed consent was obtained from all participants.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement Dataset available from the corresponding author at lisbet.meurling@karolinska.se. Participants’ consent was not obtained for data sharing, but the presented data are anonymised and the risk of identification is low.
-
Open Access This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/