Article Text

Abstract
Introduction Prior to this project, anaesthetists rarely received systematic feedback on the experience of patients in recovery. This could help to improve perioperative practice. Preliminary audits demonstrated variations in patient temperature, pain and nausea measures. Mapping the perioperative workflow revealed that delays in patient transfer from the Post Anaesthetic Care Unit (PACU) was stretching resources and threatening patient experience. We hypothesised that implementing sustained monitoring and feedback of data from perioperative quality indicators using an industrial process control approach would stimulate improvement on key outcomes at individual and system levels.
Methods A continuous monitoring and feedback initiative was launched drawing upon improvement science theory and quality improvement methods such as process mapping, iterative development and Statistical Process Control (SPC). Data on core temperature, patient reported pain, nausea and quality of recovery was collected for all elective surgical patients passing through the main surgical suite of a large academic teaching hospital by trained PACU nurses. Monthly reports on ward-transfer times and quality of recovery data were posted in the recovery unit and sent to ward managers to make variations in workflow visible across the care pathway. Personalised monthly reports were developed and distributed to individual consultant anaesthetists to provide detailed longitudinal and normative feedback on performance and details of special cases as an aid to improving use of analgesics and antiemetics, perioperative normothermia and to facilitate personal professional development. A comprehensive parallel evaluation and multiprofessional engagement workstream was undertaken to ensure ownership and acceptability of the initiative. The evaluation used a comprehensive mixed method quasi-experimental design, with a longitudinal qualitative component to capture the experience of users, evaluative surveys at multiple time-points and quantitative analysis using SPC and interrupted time series models to determine impact upon perioperative process and outcome indicators.
Results Qualitative and quantitative analysis of the experience of anaesthetists using the feedback demonstrated high perceived value and acceptability of the initiative. A range of critical enablers for this type of intervention were identified from regression analysis, including the local relevance and credibility of the data. Analysis of SPC charts revealed large variation in transfer times between different surgical wards attributable to variations in bed management and staffing practices. Nausea and Pain scores had remained relatively stable at the department level with sub-group analysis revealing variation across individuals, due to case load. Interrupted time series analysis showed a significant increase in the mean temperature of patients arriving in recovery associated with introduction of feedback of temperature data⇓.
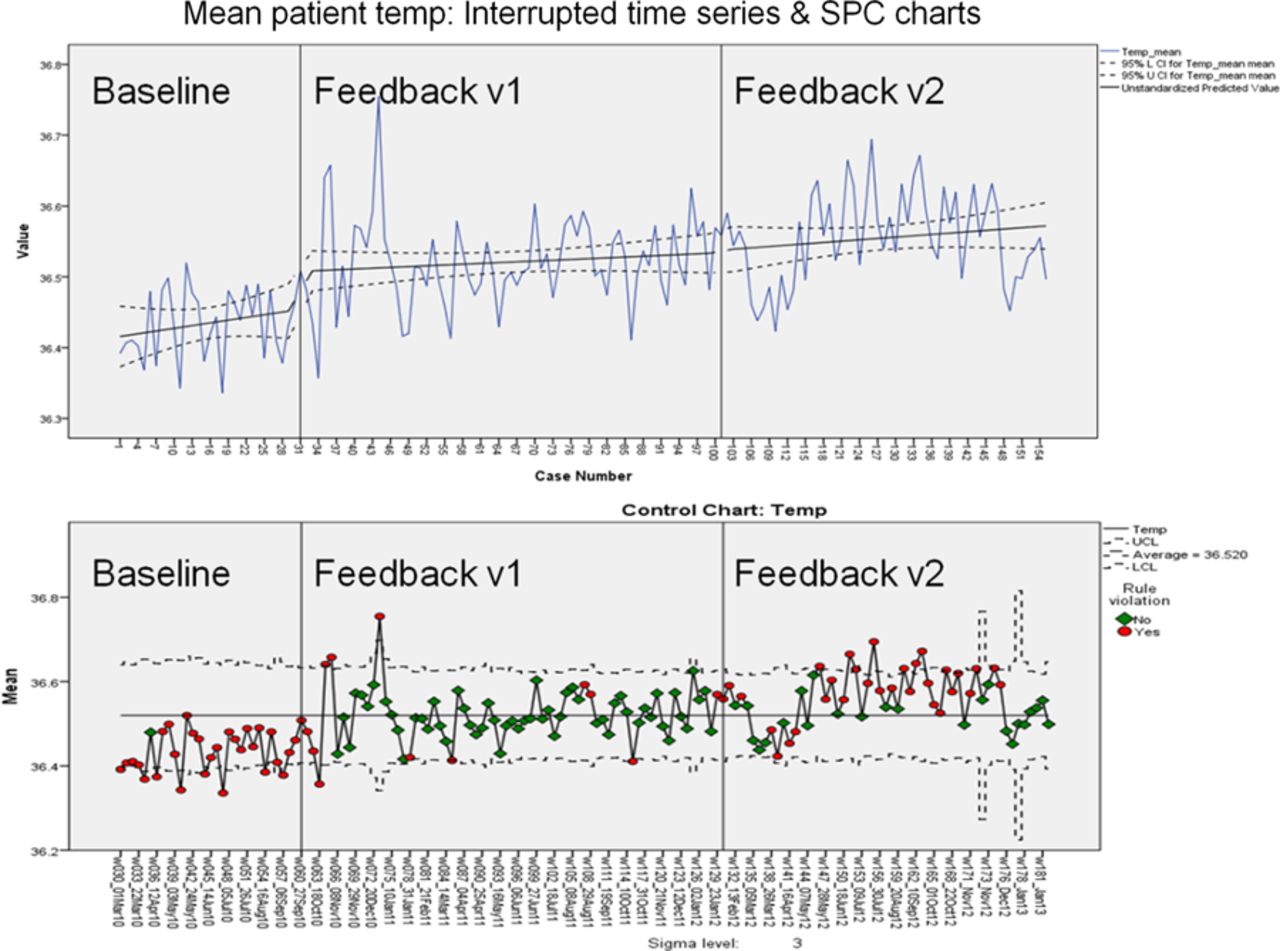
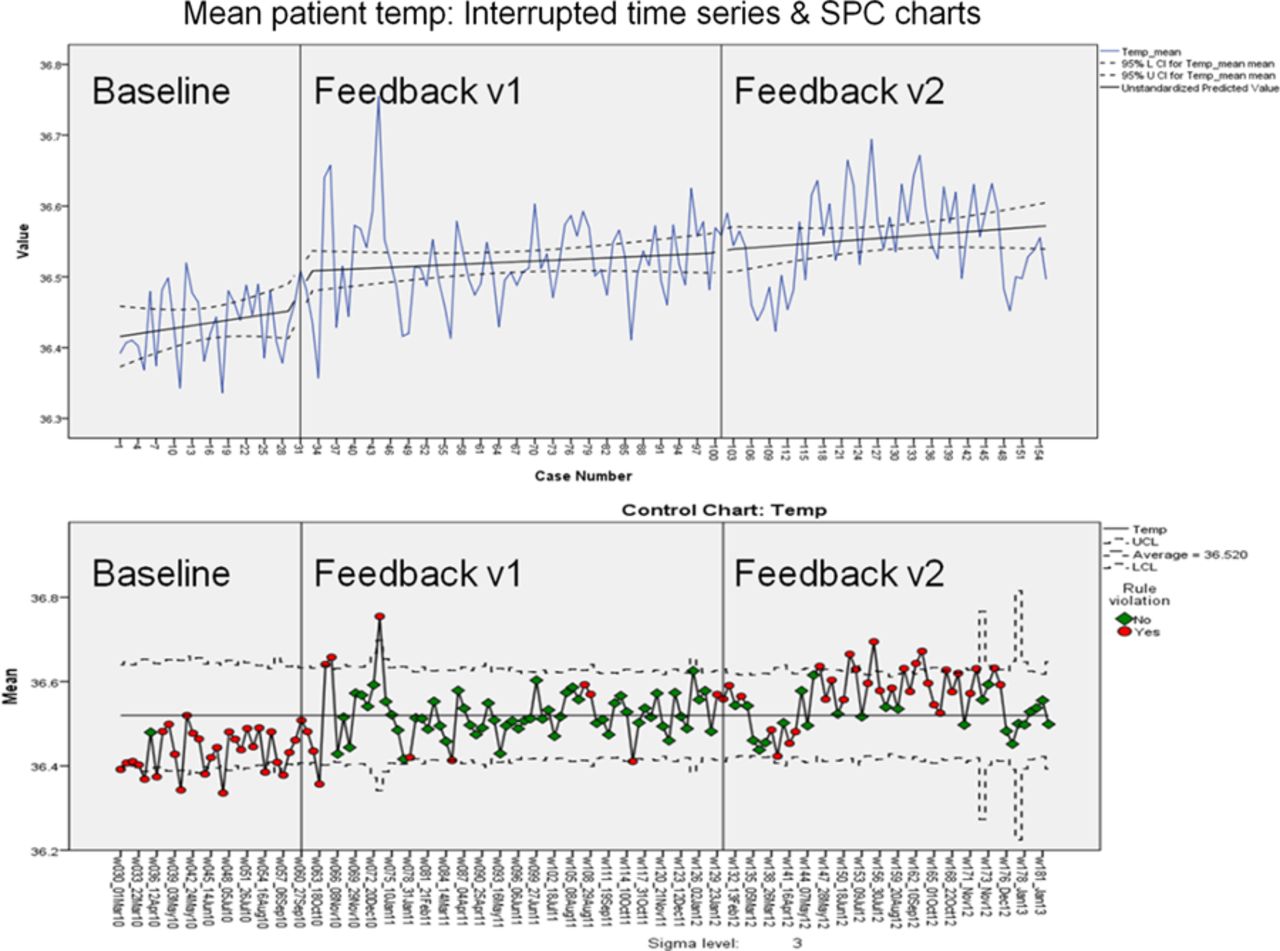{kind=link}
Discussion This study contributes important learning for both the intervention context and improvement science methods. For clinicians, data feedback that is timely, relevant, credible and acceptable to end users can be used to monitor variations in patient care and support improvement at both the personal and system levels. Findings suggest that the type of data which is often used in hospital governance is too high level for quality improvement purposes and can mask useful information concerning local variation. This project demonstrates the importance of using mixed methods and multiple outcome designs in evaluation of complex improvement interventions, in order to account for context and describe the implementation process alongside intervention outcomes.
Declaration of competing interests None.
- Patient safety
- Mortality (standardized mortality ratios)
- Patient education