Article Text

Abstract
Background Despite the widespread implementation of Tall Man lettering, little evidence exists regarding whether this technique has reduced drug errors due to look-alike sound-alike (LA-SA) drug names. This study evaluated rates of potential LA-SA drug errors in the drug management process through to the point of dispensing before and after implementation of Tall Man lettering in 2007.
Methods We used detailed pharmacy data for paediatric inpatients (<21 years old) from 42 children's hospitals in 2004–2012. After prespecifying a set of 8 potential LA-SA drug error patterns we searched within each hospitalisation for the occurrence of one of these patterns for a total of 12 LA-SA drug pairs deemed highly relevant to paediatric inpatients. To assess for potential change of error rates before and after Tall Man lettering implementation, we performed segmented regression analyses for each of 11 LA-SA drug pairs (because 1 pair had no detected potential errors) and for the overall total errors of all 11 LA-SA drug pairs.
Results Among 1 676 700 hospitalisations, no statistically significant change was detected for either the intercept or the slope of LA-SA error rate for each of the 11 drug pairs or for the combined error rate. In a sensitivity analysis of the moving average of the potential error rate over the entire study period, no downward trend in potential LA-SA drug error rates was evident over any time period 2004 onwards.
Conclusions Implementation of Tall Man lettering in 2007 was not associated with a reduction in the potential LA-SA error rate. Whether Tall Man lettering is effective in clinical practice warrants further study.
- Medication safety
- Paediatrics
- Hospital medicine
Statistics from Altmetric.com
Introduction
Medication errors are a major concern for patient safety, causing 1 of 131 outpatient and 1 of 854 inpatient deaths.1 Children may be at special risk of adverse effects caused by medication errors due to size and physiological variability, limited communication ability and treatment by non-paediatric healthcare providers.2 The safe delivery of medications to patients requires a number of sequential steps to occur without error, beginning with prescription of the correct medication and proceeding through to the safe administration of the correct medication.3 Drug names that look alike or sound alike can lead to errors at the level of the prescriber, pharmacist or bedside clinician.4 By 2008, over 1500 drug pairs had been identified as look-alike sound-alike (LA-SA) drugs.5 Reportedly as many as 3.9 million annual prescriptions involve a situation where an incorrect LA-SA drug is dispensed in community pharmacies instead of the correct LA-SA drug.6
To reduce errors attributable to LA-SA drugs, a number of typographical approaches have been explored, such as the use of bold or italic fonts or underlines. In particular, a text format known as ‘Tall Man’ lettering was recommended in 1999,7 and by 2001 Tall Man lettering was implemented as part of the US Food & Drug Administration (FDA) Name Differentiation project for the display of a set of drug names identified as highly confusable.8 Tall Man labelling uses rule-based mixed-case labelling in order to visually emphasise differences in drug names that look alike or sound alike.9 ,10 This technique aims to aid healthcare professionals in distinguishing between similar drug names and, thereby, reduce erroneous prescriptions. For example, the cephalosporins ‘cefuroxime’ and ‘cefotaxime’ look alike and sound alike. Tall Man lettering for these drugs helps highlight and distinguish the differences (cefUROXime and cefOTAXime).
Initially adopted by FDA, the Tall Man lettering scheme has since been endorsed by multiple safety regulatory and accreditation bodies in the USA and other parts of the world,11 ,12 including the Joint Commission and the Institute for Safe Medication Practices (ISMP). In one of the 2007 National Patient Safety Goals (NPSGs), the Joint Commission on Accreditation of Healthcare Organizations (JCAHO, now renamed as ‘the Joint Commission’) stated that health organisations should compile a list of LA-SA drugs and recommended to use boldface, colour or capital letters (‘Tall Man’ letters), to call attention to the difference between similar drug names.13
Despite the broad use of Tall Man lettering, little evidence exists to determine whether this technique is effective. Previous publications regarding Tall Man lettering were mostly case reports, conceptual papers or qualitative assessments. Several studies have examined the impact of Tall Man lettering on the differentiation of similar drug names in laboratory-based tasks; and evidence from these studies was not conclusive that Tall Man lettering was effective in reducing drug name errors.14–20 There are few studies that have quantitatively examined whether the widespread adoption of Tall Man lettering has been associated in clinical practice with a reduction in the number of LA-SA drug errors.
To pursue this line of research, we developed a strategy to identify potential LA-SA prescription errors during paediatric inpatient hospitalisations using the Pediatric Healthcare Information System (PHIS) data, and used a set of temporal prescription patterns as surrogate markers of potential LA-SA drug errors to study the rate of these potential errors before and after the widespread implementation of Tall Man lettering in the USA.
Methods
Data source
PHIS is an administrative healthcare database administered by the Children's Hospital Association (Overland Park, Kansas, USA), which contains inpatient data from 42 member children's hospitals. Hospital discharge data with patient demographic information and detailed day-to-day dispensed medications was available for analyses. Since the PHIS drug data in our study captures information on dispensed drugs, potential errors could have occurred at any point upstream in the workflow from this point (specifically including prescription order entry). We therefore now refer to potential errors in the manuscript as ‘potential errors in the process of drug therapy management through to the point of medication dispensing’.
This study included patients aged 0–20 years with at least one hospitalisation at the 42 children's hospitals between 2004 and 2012.
Study design
We conducted a retrospective interrupted time series analysis on the potential LA-SA error rates, and evaluated whether the implementation of Tall Man lettering was associated with reductions in the potential LA-SA error rates.
Time point of Tall Man lettering implementation: The NPSGs is a key method by which The Joint Commission promotes and enforces major changes in patient safety. In the 2007 NPSGs, hospitals were required to ‘identify and, at a minimum, annually review a list of LA-SA drugs used in the organisation, and take action to prevent errors involving the interchange of these drugs’ (requirement 3C).13 More than 90% of the hospitals in the USA used Joint Commission standards to assure the delivery of safe, quality care, and this requirement achieved 92.6% compliance, according to the 2007 annual report.21 Therefore, we designated the year of 2007 as the initiation of widespread implementation of Tall Man lettering.
Determination of LA-SA drug pairs: We began with a list of LA-SA drugs that were compiled from published lists by ISMP (http://www.ismp.org), FDA and the Joint Commission (http://www.jointcommission.org/LASA/). Using this list, we identified drugs that were present in the PHIS database. Because PHIS only records generic drug names, all brand name drugs on this list were converted to generic names. We selected 76 pairs of drugs that were frequently used in our database. Then two paediatricians and one pharmacist independently reviewed the compiled list of 76 drug pairs and selected those that were relevant to paediatric inpatients and most likely to represent a mistake when both presented in one hospitalisation. Among the consensus drug pairs, we selected 12 pairs of LA-SA drugs where each drug in the pair has a distinct clinical indication compared with the other paired drug and not those where substitution of one drug for the other could foreseeably be intended. Among these 12 pairs, 5 pairs have LA-SA generic-generic names: tramadol-trazodone, metformin- metronidazole, hydralazine-hydroxyzine, guanfacine-guaifenesin, valganciclovir-valacyclovir; 6 pairs have LA-SA brand-brand names: Celebrex (celecoxib)-Celexa (citalopram), Celebrex (celecoxib)-Cerebyx (fosphenytoin), Celexa (citalopram)-Cerebyx (fosphenytoin), Cardura (doxazosin)-Coumadin (warfarin), Prozac (fluoxetine)- Prograf (tacrolimus), Zyrtec (cetirizine)-Zyprexa (olanzapine); and 1 pair is a LA-SA generic-brand name paring: clonidine-Klonipin (clonazepam). For the sake of clarity, though, we present only generic names for these drug pairs henceforth in this manuscript.
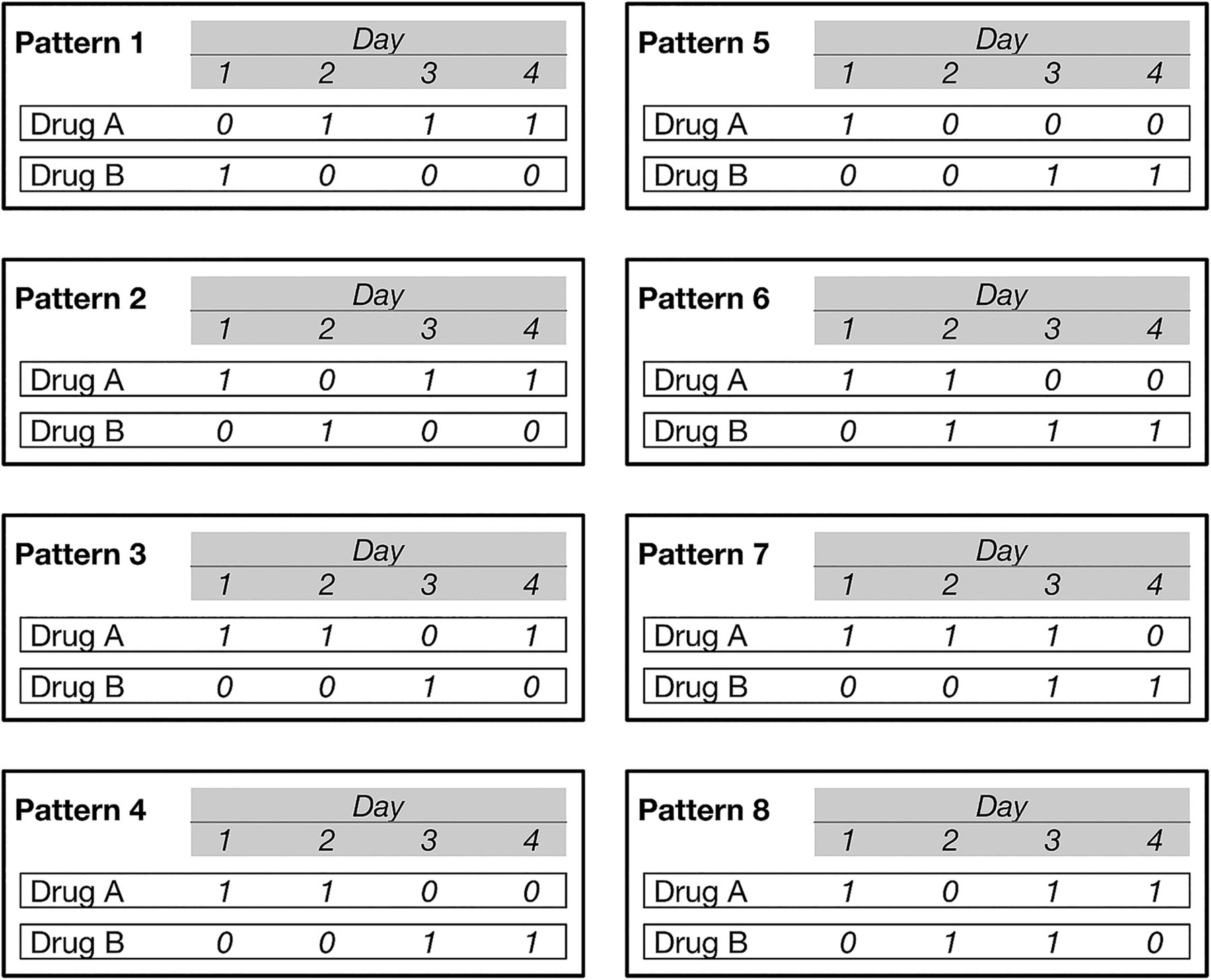
Detection of potential LA-SA errors: Under expert consultation with a clinical pharmacist and two physicians, we defined an LA-SA error as one of eight possible daily medication patterns of a pair of LA-SA drugs over a 4-day period (figure 1). Each pattern involved a ‘cross-over’ from the initial medication in the LA-SA pair (labelled as Drug A in the figure) to the other drug in the pair (Drug B), with either no overlap or a 1-day overlap where both drugs were dispensed on the same day, and in two of the patterns a ‘cross back’ to the initial drug (ie, Drug A, then Drug B, then back to Drug A). These patterns account for potential errors occurring in both directions (ie, Drug A intended, but Drug B given, or vice versa). Because this method of identifying potential LA-SA errors requires at least 4 days of hospitalisation, we only included hospitalisations that were 4 days or longer. We then used this 4-day pattern to assess all 4-day intervals throughout the entire hospitalisation, incrementing forward a day at a time, to detect all potential LA-SA errors. Once a single potential error was detected for a given LA-SA pair of drugs, the hospitalisation was classified as a hospitalisation with a potential LA-SA error for that pair.

Patterns of potential errors in any continuous 4 days of hospitalisation. 1: prescription present, 0: prescription not present. These patterns account for potential errors occurring in both directions (ie, Drug A intended, but Drug B given, or vice versa).
Statistical analysis
We calculated the rate of potential LA-SA errors as the number of hospitalisations with potential LA-SA confusion errors per 1000 hospitalisations that had exposure to either drug in the LA-SA pair. We aggregated the rates into monthly intervals for time-series analysis to estimate the effect of Tall Man lettering implementation on the error rates, adjusting for trend before implementation of Tall Man lettering and other autocorrelation, including seasonal effects (such as might occur with new trainees starting in the summer months). We used segmented regression analysis, which is the strongest quasi-experimental approach for evaluating longitudinal effects of implementations, and has been demonstrated to be a powerful method to evaluate policy and education implementations intended to improve the quality of medication use.22 We used PROC AUTOREG procedure in the SAS software for the segmented regression analyses.
In the segmented regression model, the first 36 months (January 2004 to December 2006) were treated as the preimplementation period, the 12 months of 2007 were treated as the transitional period for the implementation of Tall Man lettering and the last 60 months (January 2008 to December 2012) were the postimplementation period. The model estimated the change of the level of the potential error rate (which represents an immediate intercept change in the error rate after implementation), and also the change in the trend of the potential error rate (which represents a change in the slope of error rate after implementation). We assessed autocorrelation by means of the Durbin-Watson statistics, and if a significant autocorrelation was detected, we included the autocorrelation parameter in the model (autocorrelation was found and corrected for models with drug pair celecoxib-citalopram, and with celecoxib-fosphenytoin). No seasonality was detected. Because among the original 12 drug pairs we did not find potential errors with doxazosin-warfarin, we included only the remaining 11 drug pairs in the analyses. We conducted segmented regression for each of the 11 drug pairs, and we also conducted the segmented regression for the combined errors from all the 11 drug pairs. For the combined error rate, the denominator was the number of hospitalisations that had exposure to any of the 19 drugs (which accounted for the 11 drug pairs). In addition, since it may be the case that year 2007 was not the uniform year of Tall Man lettering implementation, as a secondary sensitivity analysis, we used local polynomial smoothing (implemented by Stata ‘lploy’) to fit the observed potential error rates for these LA-SA drugs to assess the time trends across all the study years.
Data management and statistical analyses were conducted with SAS V.9.3 (SAS Institute, Cary, North Carolina, USA) and Stata V.13.1 (StataCorp, College Station, Texas, USA). A p value of <0.05 was considered statistically significant. This study of de-identified data was determined by our IRB to not constitute human subjects research.
Results
We screened a total of 1 676 700 hospitalisations that occurred during 2004–2012 for children ≤20 years old with hospitalisation length of at least 4 days or longer, which accounted for 37% of total hospitalisations with drug dispensing. The number of hospitalisations involving at least one of the 19 drugs generally increased from 2004 to 2012, and ranged from 29 794 to 48 693 per year. The yearly rate of potential errors for all the LA-SA drug pairs ranged from 0.5 to 1.4 per 1000 hospitalisations, and the overall rate for the entire study period was about 0.9 per 1000 hospitalisations (table 1).
Numbers and rates of potential errors of LA-SA drug pairs
For each specific LA-SA drug pair, the yearly rate of potential errors ranged from 0 to 2.9 per 1000 hospitalisations. There were four drug pairs (celecoxib-citalopram, celecoxib-fosphenytoin, guanfacine-guaifenesin and fluoxetine-tacrolimus) that had five or fewer potential errors for the period 2004–2012. The number of hospitalisations, the number of potential errors, and the rate of potential errors for the 11 drug pairs are shown in online supplementary table S1.
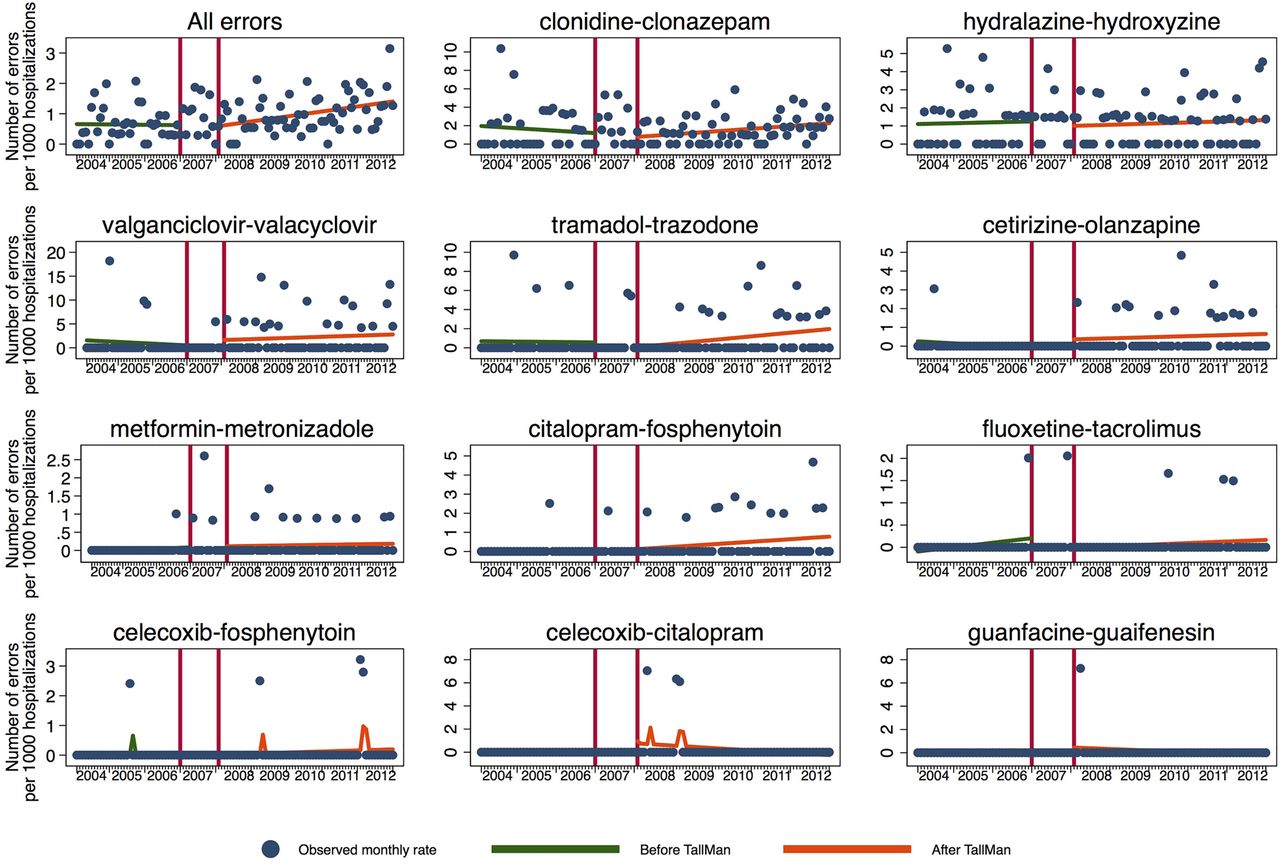
Using the 12 months of year 2007 as the transitional period for implementation of Tall Man lettering, the segmented regression analyses did not identify any statistically significant implementation effect of Tall Man lettering on the combined potential error rate for the 11 LA-SA drug pairs. Similarly, no significant effect was found when the 11 drug pairs were examined individually. We plotted the predicted rates and the observed rates of potential errors for these LA-SA drug pairs in figure 2. The level of error rate (intercept) did not change immediately after the implementation period, and the trend (slope) of the error rate did not change, after controlling for the slope before the implementation period (see online supplement table S2 for detailed results).

Trends of potential look-alike sound-alike errors before and after Tall Man lettering implementation. The green/red line is the predicted error rates before/after Tall Man lettering implementation (year 2007) from segmented regression models. The denominators are the hospitalisations that involved any of the 19 drugs (for all errors), or involved either drugs (for specific drug pairs). No significant change was found in the level or in the trend of the postimplementation rates. Total number of errors was combined from 11 drug pairs.
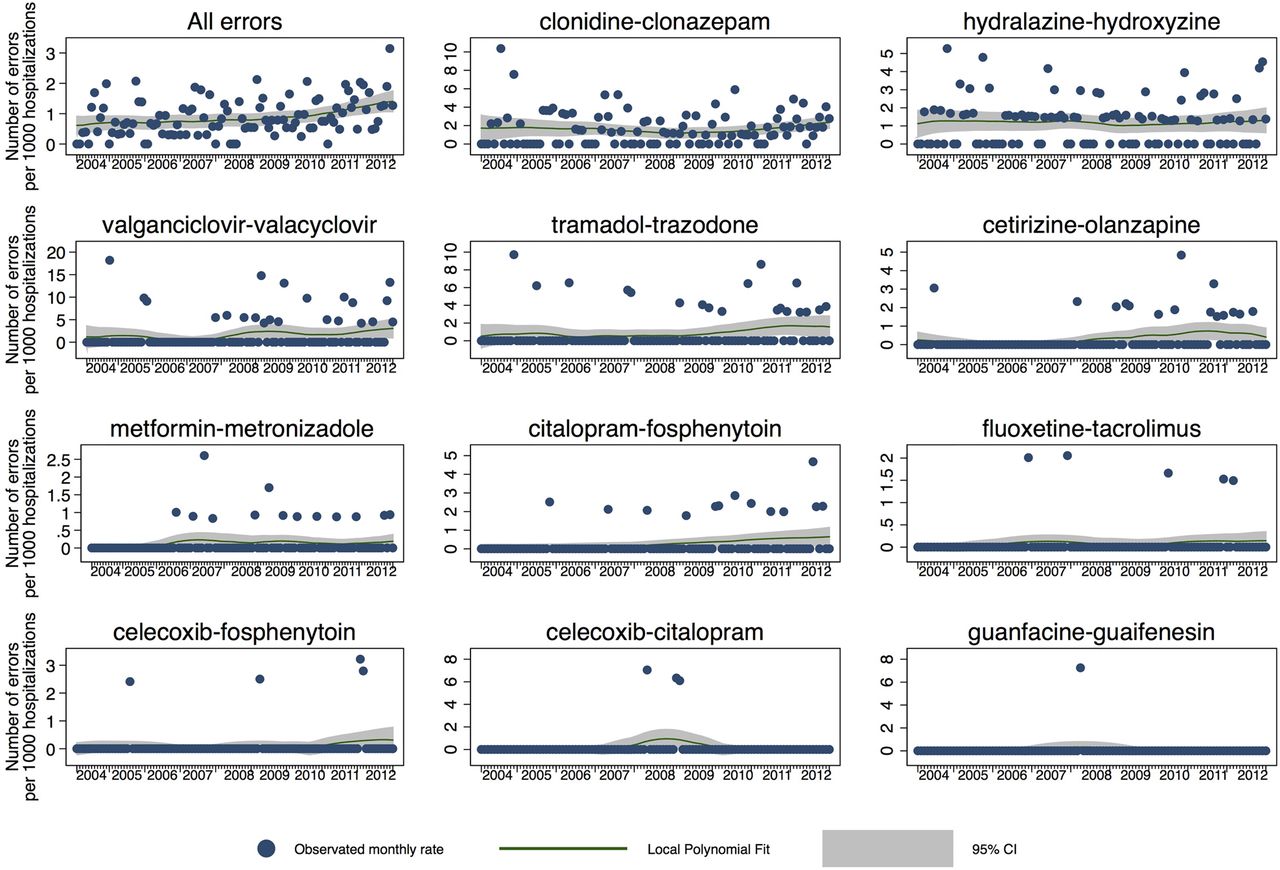
In the secondary sensitivity analysis, we plotted the time trends to assess the trends across all of the study years to account for the possibility that Tall Man lettering implementation began earlier or later than 2007 (figure 3). The fitted curves did not identify any abrupt change around year 2007 for these LA-SA drug potential error rates.

{kind=link}
{kind=link}
{kind=link}
Local polynomial smoothing (95% CI) of the error rates trends. The fitted curves were from local polynomial smoothing, no abrupt change around year 2007 for these look-alike sound-alike drug potential error rates was identified. The denominators are the hospitalisations that involved any of the 19 drugs (for all errors), or involved either drugs (for specific drug pairs). Total number of errors was combined from 11 drug pairs.
Discussion
Although there has been considerable interest regarding the degree of impact of Tall Man lettering reducing LA-SA drug confusion errors, previous studies were mostly theoretical or experiments conducted in laboratories to test whether Tall Man lettering decreases the visual perceptual confusability of drug names among volunteers.14–17 ,23–26 To our knowledge, our study is the first to compare potential LA-SA error rate before and after the wide implementation of Tall Man lettering among US children's hospitals using clinically detailed hospital pharmacy billing data. We did not find a significant change in potential LA-SA error rates in paediatric hospitalisations for the 11 drug pairs before and after year 2007. Furthermore, the temporal trend of potential LA-SA error rates across the entire study period, if anything, suggests an increase rather than a decrease over time.
Studies on LA-SA error rates in clinical practice have been limited, and the statistics on LA-SA drugs errors are rare in the existing literature.27 One study using Idaho Medicaid outpatient claims data defined potential errors as adjacent claims generated by dispensing of one drug followed by dispensing of the other drug with a similar name. They reported that of 300 LA-SA drug pairs studied, 35% were involved with at least one potential error, and a total of 1138 dispensing episodes involved potential errors during the 1993–2000 study period.28 Another study29 of LA-SA error rates used South Carolina Medicaid outpatient-dispensed drugs, and reported potential error (screening alerts) rate of 0.28 per thousand prescriptions (for 22 selected drugs) on screening, and the true error rate was about 0.03 per thousand prescriptions.
Our study design differed from the Basco et al's study in several important ways: First, we used as our indicator of a potential error patterns of use of the LA-SA pair during any continuous 4 days in a hospitalisation (inpatient), whereas Basco et al's study used a much larger time window—6 months—for outpatient data. Second, Basco et al's ‘alarm’ outcome was based on a broader and less restrictive set of patterns, because they were trying to see if their patterns could be used ‘real time’ to alert pharmacists that an error may be present. When Basco et al added a component of the pattern that we employed (namely, stopping the erroneous drug and providing only one dispensing of the drug), the 395 ‘alarms’ were reduced to 95. Of these 95 errors that are of a similar pattern as our potential errors, 43 were deemed to be ‘true’ errors based on their review of the patients’ diagnoses. Finally, Basco et al included only drug pairs wherein one drug is commonly prescribed for children but the other drug is rarely prescribed for children. This selection of drugs rarely prescribed for children may have inadvertently further lowered their observed ‘true’ error rate, in that prescribing a rare drug may be a more intentional act and less on erroneous slip. We selected paired drugs that are both plausible to be intended for paediatrics, and thus can slip by (in the mind of the prescriber or when being reviewed by others in the drug therapy management process) because either drug would be plausible for hospitalised paediatric patients.
While our study has the strengths of a large sample size and the use of segmented regression analysis of interrupted time series data (which allows control for prior trends in the outcome and to study the dynamics of change in response to an intervention), our study also has limitations that warrant close consideration. First, we only identified potential errors based on patterns of medication dispensing data. While we expect that the true error rates would be lower than potential errors, medical chart audit might conversely reveal additional true LA-SA errors that could not be detected by our pattern-matching approach. The types of potential errors that could be identified with this methodology include two scenarios: (1) a provider incorrectly prescribes an LA-SA medication which is subsequently dispensed by pharmacy or (2) a provider prescribes the intended medicine of the LA-SA pair but the pharmacy incorrectly dispenses the other medicine due to a transcription error. Even if drug information is transcribed correctly, the pharmacy could still pick the wrong drug off the shelf, but this information can't be detected by PHIS because the billed drug information is still for the correct drug.
Second, we identified potential errors only during the designated 4-day window when the first of the drug pair was initiated; consequently, we would have missed any errors that were first detected and corrected beyond the 4-day window. Third, we identified potential drug errors at the stage when medications were dispensed; we do not know what proportion of these medications were administered to patients or were, instead, detected as erroneous prior to being administered. Fourth, we did not examine all available LA-SA drug pairs in our data source, which included over 250 pairs, but instead (for reasons we noted above) selected those pairs that are both most clinically important and relevant to paediatric inpatients and least likely to be ordered in quick succession. Finally, there are variants of Tall Man lettering,11 and we could not account for this variation in our study because we do not have access to data regarding which form of Tall Man letter different hospitals might have used.
While our findings suggest that Tall Man lettering has not reduced potential LA-SA errors, we should consider six possible explanations for this null finding. First, as we stated previously, the FDA and other safety regulatory bodies had recommended Tall Man lettering before the JCAHO's 2007 NPSGs, so effort to reduce LA-SA might have been implemented in this sample of hospitals prior to 2007, hampering our ability to detect an effect of implementation in 2007. Our sensitivity analysis, however, does not support this explanation, as there does not appear to have been any significant decline in the rate of potential LA-SA errors extending back to 2004. Second, our method of identifying potential LA-SA errors required hospitalisation of four or more days, and potentially shorter hospitalisations have different rates of LA-SA errors (but we know of no data to support this hypothesis). Third, the 11 drug pairs analysed in our study are not representative of all LA-SA drug pairs. Whether the overall rate of error for all other LA-SA drug pairs would be higher, lower, or the same as the pairs included in this study remains to be determined. Fourth, as the LA-SA drugs are constantly identified and added to lists by regulatory agencies, the drug pairs we studied might appear in different lists in different time points during the study period, thereby diluting any time-specific effect of Tall Man lettering implementation. Fifth, the period of this study overlaps with the era in which the widespread adoption of computerised physician order entry (CPOE) occurred. Since CPOE can intercept drug name confusion errors by generating indication alerts during ordering,30 and has been shown to reduce medication errors,31 the concurrent adoption of CPOE might have lowered the observed rates of potential LA-SA errors independent of any effect of Tall Man lettering. This potential confounding effect of CPOE would not explain, however, why our results suggest (but not to a statistically significant degree) an increasing rate of errors over time. Finally, generalised increased awareness of the LA-SA problem among staff could also have reduced errors, above and beyond a specific effect of Tall Man lettering implementation (although, as noted previously, the overall trend of potential LA-SA errors was, if any, rising over time).
One of our findings warrants particular discussion, namely that the relationship between generic and brand names may be related to rates of LA-SA errors. The drug pairs that had over 20 errors were either generic-generic name or generic-brand name (clonidine-clonazepam, hydralazine-hydroxyzine, valganciclovir-valacyclovir and tramadol-trazodone). Because the use of generic names is the current standard in children's hospitals and our data found that most potential errors involved generic-generic pairs and not brand-brand pairs, any subsequent studies and interventions must pay special attention to generic pairs.
Finally and importantly, our study suggests very low rates of LA-SA confusion errors for the 12 LA-SA drug pairs studied in 42 children's hospitals during 2004–2012. The overall potential LA-SA error rate was less than 1/1000, and we expect the true LA-SA error rates may be even lower.
Conclusion
Although Tall Man lettering has been widely adopted by US hospitals since 2007, this study of 42 children's hospitals from 2004 to 2012 did not detect a significant change in potential LA-SA errors during drug prescribing or dispensing after 2007. The rates of potential LA-SA errors for our selected LA-SA drug pairs remained extremely low during the entire study period.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online table 1
- Data supplement 2 - Online table 2
Footnotes
Contributors All authors participated in the design of the study and interpretation of the data; WZ, DD, and CF performed the data analysis; WZ, JAF, NSP and CF drafted the manuscript; all authors revised the manuscript for key intellectual content. All authors read and approved the final manuscript.
Funding Agency for Healthcare Research and Quality (grant no. 1RO1HS018425).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.