Article Text

Abstract
Background Despite growing interest in engaging patients and families (P/F) in patient safety education, little is known about how P/F can best contribute. We assessed the feasibility and acceptability of a patient–teacher medical error disclosure and prevention training model.
Methods We developed an educational intervention bringing together interprofessional clinicians with P/F from hospital advisory councils to discuss error disclosure and prevention. Patient focus groups and orientation sessions informed curriculum and assessment design. A pre-post survey with qualitative and quantitative questions was used to assess P/F and clinician experiences and attitudes about collaborative safety education including participant hopes, fears, perceived value of learning experience and challenges. Responses to open-ended questions were coded according to principles of content analysis.
Results P/F and clinicians hoped to learn about each other's perspectives, communication skills and patient empowerment strategies. Before the intervention, both groups worried about power dynamics dampening effective interaction. Clinicians worried that P/F would learn about their fallibility, while P/F were concerned about clinicians’ jargon and defensive posturing. Following workshops, clinicians valued patients’ direct feedback, communication strategies for error disclosure and a ‘real’ learning experience. P/F appreciated clinicians’ accountability, and insights into how medical errors affect clinicians. Half of participants found nothing challenging, the remainder clinicians cited emotions and enormity of ‘culture change’, while P/F commented on medical jargon and desire for more time. Patients and clinicians found the experience valuable. Recommendations about how to develop a patient–teacher programme in patient safety are provided.
Conclusions An educational paradigm that includes patients as teachers and collaborative learners with clinicians in patient safety is feasible, valued by clinicians and P/F and promising for P/F-centred medical error disclosure and prevention training.
- Safety culture
- Health professions education
- Patient-centred care
- Patient education
- Simulation
Statistics from Altmetric.com
Introduction
It wasn’t just the workshop, it was the whole process. The focus groups and prep meetings, we were asked questions we’ve never been asked before.—A patient participant
Patient and family engagement (PFE) is commanding increased attention in safety efforts.1–5 Leading organisations encourage patients to participate in safety6–8 and some patients are stepping forward to engage actively with clinicians as safety partners.9–11 While P/F members increasingly serve as advisors in quality improvement committees12 and patient experience is routinely surveyed after hospitalisations,13 ,14 such interventions may lack the reach to tangibly bring patients' and families' (P/F) voices to the frontlines of care.
PFE may be particularly critical in the context of medical error disclosure training, as patients rate lower satisfaction with such conversations than physicians after harmful events.15 Ensuring that P/F voices are heard in disclosure training can help better prepare clinicians to meet P/F needs in such a vulnerable time.16 ,17 Healthcare organisations can learn from patient input about adverse events to gain a fuller perspective of the event,18–23 and better understand P/F experiences and expectations after harmful events.4 ,24 ,25 Effective integration of P/F into safety efforts may also empower them to speak up about care concerns.26 ,27 To achieve meaningful PFE, some experts advocate inviting P/F as teachers and codesigners of educational initiatives.28
Medical error disclosure training programmes are rapidly disseminating in the USA29–31 and other countries.32 Yet opportunities for patients and providers to come together, reflect and engage in collaborative learning about patient safety communication are still lacking.33 ,34 Little is known about the potential role for patients as teachers to help clinicians develop the relational and communication skills when things go wrong, and what risks PFE in patient safety education with clinicians may raise.18 ,20 ,21 ,26 Similarly, training patients as safety advocates if they observe a problem in care is rare, and patients seldom have opportunities to develop and practice the skills that enable them to speak up for themselves or their loved ones in the healthcare setting.27
To address these gaps, we developed a new programme ‘Patient-Teachers in Patient Safety’ (Patient TIPS), bringing interprofessional clinicians together with P/F members in a collaborative learning experience. The intervention focused primarily on developing more patient-centred medical error disclosure communication skills for clinicians. It also addressed partnering more effectively with patients to prevent errors by supporting P/F to speak up about concerns.
The aim of this study was to evaluate the feasibility and acceptability of the Patient TIPS collaborative learning model to P/F and clinicians. Because we anticipated that clinicians, patients and organisations may have reservations about bringing P/F and clinicians together to talk about medical errors, we focused on understanding potential benefits and risks of such an educational intervention. We anticipated that understanding these factors could inform strategies to enhance the educational benefits, mitigate any possible concerns and thereby facilitate broader programme implementation. We address the following research questions:
Is it feasible to engage P/F and interprofessional clinicians in a collaborative learning programme on medical error disclosure and prevention? Specifically:
Would P/F and clinicians be willing to participate?
Would each group feel comfortable discussing communication about medical errors with the other?
What are the programmatic characteristics necessary to create a safe space for collaborative discussions between clinicians and P/F about medical error communication?
What are the benefits and risks of such an intervention?
What do clinicians find valuable about learning with P/F? What are their concerns?
What do P/F find valuable about learning with clinicians? What are their concerns?
Methods
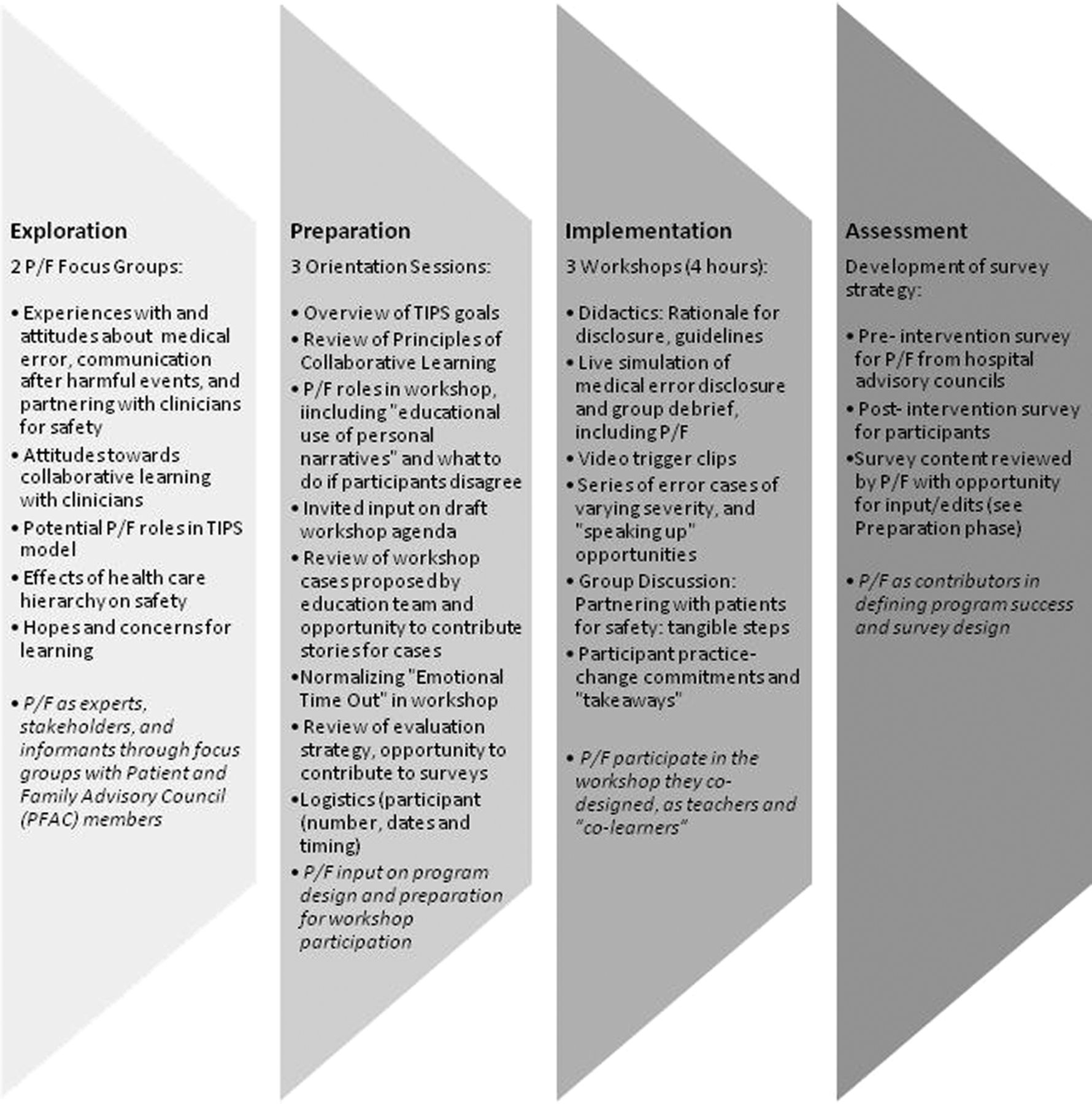
The study was designed as a mixed methods study using qualitative and quantitative data to explore participants’ experiences and perspectives on the educational intervention in four phases, each directly involving P/F (figure 1). During the exploration phase, we held discussions with P/F at Patient and Family Advisory Council (PFAC) meetings to describe the programme and receive feedback. These guided discussions served as focus groups (FG) to gain P/F insights into programme design including curricular content and facilitation strategies. The preparation phase included orientation sessions (OS) with volunteering P/F, preparing them for workshops. During the implementation phase, we carried out the actual educational intervention in which P/F participated. The evaluation phase included a preintervention and postintervention survey for P/F and clinicians, and workshop debriefings. Further details of the curriculum design, and the characteristics of the exploration, preparation and implementation phases can be found in the online supplementary appendix.
{kind=link}
Roadmap of Patient TIPS phases and P/F participation in each step. P/F, patients and families; Patient TIPS, Patient-Teachers in Patient Safety.
Supplementary appendices
Educational intervention
Because conversations about medical errors are interpersonally and emotionally challenging and involve taking risks between stakeholders across the medical hierarchy, we used two conceptual frameworks to design our educational model: (1) relational learning34 ,35 (online supplementary appendix 1) and (2) psychological safety40 ,42 The Program to Enhance Relational and Communication Skills (PERCS) has been used since 2002 and was developed to help clinicians from different professions improve their relational and communicative competence to meet the challenges of difficult conversations in a variety of healthcare settings.35–40 Psychological safety promotes a safe space for interpersonal risk taking,41–43 and organisational learning.44–46 In order to further create an educational setting in which P/F feel safe to speak up and take on a teaching role, we engaged P/F as stakeholders from the very beginning and throughout the curricular design, implementation and evaluation process.
Three workshops were consecutively held between 2012 and 2013 in two academic medical centres. We planned to conduct 3 workshops, each accommodating 20–25 learners. We set a goal of recruiting 15 P/F members (aiming for 20%–25% participation by P/F) based on precedent of proportions in a paediatric palliative care educational intervention involving bereaved parents.47 ,48 The 4 hour workshops featured an in-depth simulation of a medical error disclosure based on a case developed by the education team with invited input from P/F. Professional actors portrayed the role of P/F members, and clinicians played their own role.49 Each enactment was immediately followed by debriefing including the actors, clinicians, P/F and facilitators.35 ,36 Throughout the workshop, P/F also shared their own experiences at will. The workshops included several other interactive components involving P/F and clinicians (figure 1 and online supplementary appendix). Facilitators included physician, psychosocial and family faculty who are practicing professionals and educators.
Participants
We recruited a purposive sample of P/F and clinicians interested in patient safety to participate in the workshop. P/F from two hospital PFACs volunteered to participate after introduction to the Patient TIPS programme at a PFAC meeting. In order to expose clinicians to a wide variety of P/F experiences in discussion of error disclosure and prevention, we did not restrict our sample to P/F who self-reported an error. P/F who participated in the workshops attended a preceding orientation session that focused on principles of collaborative learning (figure 1 and online supplementary appendix). In addition to workshop participants, all P/F from one PFAC were invited to complete baseline surveys to provide a broader understanding of patient attitudes related to collaborative learning about medical error. Physicians, nurses, nurse managers, social workers, medical interpreters and other healthcare personnel were invited to participate in workshops by hospital safety and professionalism leaders from two academic hospitals via email, which briefly described the programme. To ensure that clinicians and P/F did not have an existing relationship prior to the workshop, participant lists were shared before the training.
Survey design
Baseline and postintervention surveys were designed with input from P/F participants. We included P/F in this phase as part of our commitment to integrate P/F throughout the programme, and so that our measures of the programme's impact would also reflect P/F values and priorities. Questionnaires were based on previously published PERCS surveys,35 ,36 and adapted for the Patient TIPS format and research goals. The pilot version of the survey was developed by physician-researchers with expertise in patient safety, patient engagement and ethics, with input from a social worker and P/F representative. It was reviewed by P/F and clinician representatives for content and understandability, and subsequently finalised after P/F feedback in the first orientation session.
To address research question 1 (feasibility), we included items about collaborative learning attitudes and queried participants’ comfort participating in the workshop. For research question 2, we addressed perceived benefits and risks of participation. Presurvey questions included: “What are you hoping to learn from (P/F or clinicians)?” and “What concerns do you have about learning with (P/F or clinicians)?” Postsurvey questions included: “What, if anything, was valuable about learning with (patients/families or clinicians)?” and “What was the most difficult thing about learning with (P/F or clinicians)?” Quantitative items included yes/no and a 5-point Likert-scale questions.
P/F and clinicians received separate but parallel surveys. Surveys were administered on paper before the workshop or online through Survey Monkey. Postquestionnaires were administered at the end of each workshop.
Analysis
We used descriptive statistics to analyse quantitative data. For the four open-ended questions, we created a database of all responses resulting in a total of 282 utterances, which were typically one sentence or shorter (Preintervention quotes A1-180, postintervention quotes B1-B102). Responses were coded according to the standard principles of content analysis.50 Data from P/F and clinicians were coded separately and grouped into thematic domains for each open-ended question. After reviewing all the data, two study team members developed coding categories and discussed them iteratively to reach consensus. Coding was first performed by a physician-researcher and educator familiar with the Patient TIPS pedagogy, but not present at the workshops and second by a physician-researcher who was present at all of the workshops. Areas of disagreement were discussed until consensus was reached.
Ethics
The study was exempt by the Institutional Review Board at our hospital.
Results
Feasibility and acceptability of the Patient TIPS collaborative learning model
Baseline data were collected from 53/55 (96%) of participating clinicians and 71/88 (81%) of P/F (including both PFAC members who went on to participate in the workshops, and those who did not volunteer for the programme). Clinicians’ years of experience ranged from <1 to 42 years. Of all P/F members, 36% reported they had experienced a medical error in the past. Of those, 48% stated that the medical error had been disclosed to them.
A total of 18 PFAC members, and 55 clinicians stepped forward as volunteers for the programme. All 55 clinicians and 9 P/F completed the workshop, with roughly 15%–20% of learners comprised by P/F at each session, approximating our goal. We ultimately had fewer patients participate in workshops than expected because of scheduling conflicts or illness; a couple of patients cancelled just before the workshop. Characteristics of clinicians and P/F who participated in the baseline and the postworkshop survey are shown in table 1.
Characteristics of clinicians and P/F who participated in the baseline and the postworkshop survey
At baseline, nearly all responding clinicians (98%, 52/53) and P/F (94%, 61/65) thought the collaborative learning model was a good idea. After the workshop, 84% (42/50) of responding clinicians reported they felt comfortable discussing errors with patients. Likewise, 100% (9/9) P/F completing the training reported comfort discussing errors with clinicians.
Programme characteristics needed to create a safe space for collaborative learning
Key insights from FG and OS were used in programme design, including curricular content and facilitation strategies (table 2). For example, based on discussions in FG and OS, P/F prioritised understanding why clinicians wanted to come to the workshops, leading us to include discussion and survey assessment of what individuals hoped to learn. They also highlighted attention to seating arrangements and power dynamics, concepts echoed in the qualitative thematic analysis of survey data.
Insights from focus groups and effects on curricular adaptation
Risks and benefits of the collaborative learning model
Potential risks: participant concerns and challenges
Asked about their concerns related to the educational model prior to the workshop, about half of clinicians held no worries. Those who reported concerns most commonly cited two issues. They were worried that power dynamics may limit effective interaction with P/F: “People aren’t going to say what they truly feel based on who is in the room or [it] is going to get very tense in the opposite direction with a lot of conflict.” (A87) They also worried that patients would learn about physicians’ fallibility and that P/F “will lose confidence in [their] provider [or] other care givers.” (A92) While clinicians generally focused on potential harms to P/F by learning about medical system imperfections, some also pointed out their own vulnerability to “hearing ways we have harmed and/or disappointed them when giving care.” (A69)
Among P/F, about half reported no concerns. Some P/F articulated an understanding of medical hierarchy and feared defensive posturing by clinicians as a barrier to open exchange and the opportunity to learn from P/F.I worry that the healthcare providers wouldn’t have the freedom to speak openly with their colleagues due to patient participation, as if they were on display and had to “perform”. While the idea of having patient input is good in theory, it may be challenging to create a judgment-free zone in reality. It would require very specific, flexible, honest, confident individuals who are clear communicators and really strong in their roles. (A148)
Some worried about untoward effects of power dynamics, such as P/F gaps in medical knowledge that could leave P/F to feel excluded or disrespected: “I would hope that they would neither use too much medical jargon nor talk down to the non-medically trained participants.” (A154)
After the training session, half of clinicians reported ‘nothing’ was difficult about discussing communication related to errors with patients. Other clinicians found it challenging to deal with emotions arising from P/F experiences, such as “their hurt and potential mistrust of the medical profession,” (B52) and “anger and distrust—that may be deserved.” (B70) Several clinicians were taken by insights into the shortcomings of the healthcare system, and the enormity of the task to induce change, that there are “no easy fixes and lots of culture-change required in family-centered care.” (B84) Clinicians also acknowledged that meaningful change regarding collaboration with P/F will require levelling the playing field to some degree, given, “the lack of power or the great power differential perceived by P/F with respect to clinicians.” (B72) Still, asked what was most surprising about the shared learning experience, clinicians most commonly expressed, “That it can be done.” (B85)
Like clinicians, about half of P/F reported ‘nothing’ was difficult about learning with clinicians about medical errors. A few commented on the challenge of medical jargon and that they would benefit from longer workshops. P/F reported few surprises about the shared learning experience, but were pleased to see how receptive clinicians were to working together with P/F. They noted that while patients may be nervous to participate, the experience can be transformative.
Potential benefits: the value of collaborative learning
Asked specifically what they hoped to learn from patients prior to the training, clinicians’ responses revealed three themes. First, they aimed to better understand patients’ perspectives, expressing interest in learning “what it might be like on the receiving end” (A61) of an error disclosure, and “how [patients] perceive us medical professionals.” (A33) Clinicians wanted to learn about patient concerns, “to hear their feedback,” (A55) and “their worries and assumptions—which may remain unverbalized in a typical encounter in the office.” (A18)
Second, clinicians were interested in learning how to best communicate after harmful events. “[I hope to be] hearing from patients and families about what they consider effective and compassionate communication.” (A59)
Finally, clinicians prioritised understanding patient empowerment strategies: “[I hope to learn about] what issues exist that prevent or limit their active involvement in their care and decision making,” (A32) and “what providers can do…[to] create a positive experience [for patients].” (A62)
Regarding what P/F hoped to learn from clinicians, P/F frequently voiced an interest in “how the provider thinks.” (A108) They were interested in how clinicians deal with medical error on an individual and organisational level, citing, for example, “what clinicians experience in a medical error” (A4) and what policies are in place in such an instance. They queried “how safety protocols are followed to prevent error, and when an error does occur, what is the procedure for disclosure to patients and families.” (A120) P/F thought a better understanding of the clinicians’ perspective could help better prepare P/F, if things go wrong.
Second, P/F were interested in concrete advice about strategies for communicating with clinicians and how they could better partner with clinicians for safety:[I would like to learn] questions to ask healthcare professionals in order to prevent/minimize medical errors, [and] my role as a patient in minimizing errors. (A115)
Finally, they hoped for openness from clinicians to hear P/F input, and wondered how to get clinicians engaged in learning from patients:[I hope clinicians] recognize the power of a partnership with patients. That they are willing to be seen as fallible human beings. That they believe an honest relationship with a patient for whom they are caring is essential to a good outcome of the patient’'s illness. (A105)
Following the workshop, nearly all (96%, 48/50) clinicians reported P/F participation was valuable to their learning, independent of profession or years of clinical experience (data not shown). All (100%, 9/9) patients agreed that the participation of clinicians was valuable to their learning. Asked specifically what was valuable, clinicians commonly underscored three areas. First, they reported new insights into patient perspectives. They highly valued the opportunity to receive feedback from patients, and a new space to hear from P/F members in ways that are much harder to come by in routine clinical encounters. By learning alongside patients, some clinicians noted increased awareness of their own roles as patients.Somehow, even though we are all patients at some point, as health care workers we often lose the capacity to see things as a patient in theoretical situations and even real situations. Having them there reminded us of their perspective. (B26)
Second, clinicians stated that the patients’ participation helped them to better understand effective communication strategies during challenging conversations. “The importance of trust and honesty” (B7) was highlighted. Some clinicians noted that P/F “need time to process—we go too fast.” (B75) Similarly, clinicians valued the opportunity to understand “what [patients’] take-aways from the conversation [were]” (B12) in order to gauge how well they were communicating with P/F, and to understand that what they think they are saying is not necessarily what patients are hearing.
Finally, clinicians underscored the value of a ‘real’ learning experience through the authentic emotions triggered by discussing medical errors with P/F, and “discuss[ing] areas of mutual vulnerability.” (B45) Amplifying the power of simulation by adding the moral urgency of learning with patients, they noted that the workshop had “the air of real transparency,” (B32) allowing them to imagine and practice how they would respond in the actual clinical environment.
P/F responses after the workshop similarly highlighted three themes. First, P/F valued experiencing clinicians’ sense of accountability following medical mistakes: “How they see their own responsibility and how they may look at stakeholdership differently.” (B87) Second, they highlighted new insight into the clinician experience with medical error, and particularly the emotional impact of medical error; “How [clinicians] feel when a medical error happened to one of their patients, I had never heard medical people acknowledge feeling before.” (B90) Lastly, patients and families welcomed the candour, the opportunity to see“[the clinicians’] honesty and self-reflection, and their sharing of both.” (B88)
A summary of themes from P/F and clinician perspectives on potential risks and benefits are summarised in table 3.
Potential risks and benefits of collaborative learning: clinician and P/F themes (shaded areas present exploratory data)
Discussion
We found that bringing P/F and interprofessional clinicians together to learn about medical error disclosure and prevention is feasible and acceptable to participants. Nearly all P/F and clinicians felt comfortable discussing errors with each other, and found the learning experience valuable, independent of profession or years of clinical experience. Involving P/F early and comprehensively in programme design and evaluation strategies can help shape the envisioned role of patients as teachers, and engage P/F as stakeholders in the programme.
Among potential benefits, we were struck by the similarity between learning agendas ‘hoped for’ by P/F and clinicians. Prior to their participation, both groups independently prioritised better understanding of each other's perspective, learning about specific communication strategies to improve safety and error disclosure and empowering patients as safety advocates—highlighting a curricular alignment in the shared learning experience.
While clinicians were concerned about exposing their own fallibility, patients literally hoped that clinicians would be willing to be seen as ‘fallible human beings’, underscoring the power of the programme to challenge assumptions. Clinicians particularly valued direct patient feedback, finding such opportunities scarce in routine practice. In our workshops, these P/F comments were among the most powerful ‘teaching moments’. At the same time, P/F discovered a window into the clinician's world, better understanding how to engage with the healthcare system and its professionals. Clinicians and P/F were most surprised that ‘it can be done’, challenging educators to more deeply integrate P/F in medical error disclosure and prevention education. Creating opportunities for P/F and clinicians to better understand one another may prove critical to improving patient safety.
Our study highlights activation of both P/F and clinicians, and suggest that P/F-centred education, as advocated by experts,28 can have powerful effects on learners (see online supplementary video 1). The Patient TIPS model provides a tangible way to involve P/F in safety education design and delivery. It may be a particularly useful strategy as communication and resolution programmes disseminate across the USA and globally,30–32 and leaders seek ways to clearly demonstrate partnership with P/F. Dedicated studies to examine the link between collaborative learning strategies and outcomes, including changes in P/F and clinician communication behaviours and institutional safety culture or safety outcomes51 are a research priority.
Supplementary video
Our findings expand on previous work exploring the role of patient-educators,52–55 by examining qualitatively in depth what both P/F and clinicians experience in a collaborative learning model. In a prior controlled intervention study, use of patient narratives to train doctors in patient safety55 did not demonstrate clear benefit in terms of patient safety attitudes, and generated both positive and negative reactions from doctors. Although data on P/F are limited, prior studies of Standardized Patients (SP) also indicate some potential concerns and stressors for SPs.56 While clinicians in our study commented on possible negative emotions related to fallibility, we were surprised to find that patients in our study reported few concerns about negative emotions triggered by the training, and both groups reported benefits. This may be due to extensive preparation of P/F or their relative experience as PFAC members, or the voluntary nature of participation. We chose to develop didactic workshop cases and share them with P/F before the session in the event that any of the scenarios were too close to their own experience and too emotionally jarring. While the additional safeguards for P/F are important since they enter the sessions in a traditionally more vulnerable role, our findings and others suggest that clinicians may struggle with emotions,45 ,47 ,55 and may also benefit from advanced preparation and support.
PFE in safety education: what can be learned from the Patient TIPS experience?
As we reflect on our experience, the success of the programme stemmed from in-depth preparation, conscientious facilitation during workshops and strong institutional support for patient engagement, medical error disclosure and novel approaches to enhance patient safety. Integrating insights and lessons learned, we propose recommendations for educators and innovators who are considering a Patient TIPS model (table 4). Engaging with the institutional PFAC is a good way to identify volunteer patients who have already been through the PFAC selection process. Despite high motivation by P/F, we experienced more cancellations than anticipated prior the workshops due to scheduling conflicts or illness. Planning with back-up P/F candidates may help to counterbalance such events. Facilitators with strong skills in levelling traditional hierarchies—notably perceived by clinicians and patients alike in our study as a potential barrier—are needed to create a safe learning environment. While each group cited power dynamics as a concern, neither described it as a learning challenge after the curricular intervention, suggesting that establishing ground rules for shared learning play an important role.47 Facilitators should also acknowledge potential emotions triggered for both P/F and clinicians during training sessions. Finally, institutional support is critical, and tailoring educational content to reflect local disclosure practices and policies is a sine qua non to clinician buy-in and effective outcomes. At the same time, participation may accelerate providers’ motivation for culture change, as we saw in our study, and institutional leaders may seek ways to best harness this potential by supporting these advocates and new approaches to patient engagement in safety.
Recommendations for educators and innovators to support Patient TIPS programme development
Study limitations include voluntary participation. A selection bias towards individuals with awareness for patient safety, engagement and error disclosure is therefore likely. Similarly, PFAC members likely represent more activated patients than the general public; however, PFACs have become a common practical source for P/F engagement for clinicians developing quality improvement projects and educators designing patient-centred curricula. Participants were recruited from two academic centres, and may represent views that do not reflect those of other organisations. The study is also limited by a small sample size for P/F completing the training. However, we share these qualitative data as exploratory, and note that patient and family perspectives often echoed clinician themes about the collaborative learning and were also consistent with results from the baseline survey among the larger group of P/F.
Conclusion
P/F-centred communication after harmful events requires understanding P/F perspectives. Patient and family engagement needs to be more strongly reflected in medical education to support clinicians that are equipped to deliver care in the era of transparency. Patient–teachers can help frontline clinicians to learn ‘first-hand’ from their experiences, and patients can also learn from clinicians how to better partner for safety in ways that are not otherwise accessible to them in routine healthcare settings. Shared learning between P/F and clinicians can empower P/F in safety, provide clinicians with deeper sensitivity and insights into P/F perspectives and enhance safety collaboration between P/F and clinicians.
Acknowledgments
The authors thank the patients, families, and clinicians who participated in the Patient TIPS program for sharing their insights (see online supplementary video 1). They also thank the Patient and Family Advisory Councils at Beth Israel Deaconess Medical Center and Cambridge Health Alliance, the Massachusetts Alliance for Communication and Resolution after Medical Injury, Pat Folcarelli RN, PhD, Erica Dente, Elana Premack-Sandler, and Liz Gaufberg MD for their support of this work. They are grateful to Betsy Lowe, Shane P. McBride, Sandy Novack, Melinda Van Niel, MBA, and Alison Rapoport MD for their dedication to the program and participation in the video; and to Kelly Lawman for editing and producing the video. Finally, the authors gratefully acknowledge Elaine C. Meyer, PhD, RN and their colleagues at the Institute for Professionalism and Ethical Practice for their shared insights and continued collaboration in innovative curricula to improve communication with patients and families; Donna Luff, PhD for her contributions to the manuscript; and Elana Premack Sandler, LCSW, MPH, former Patient and Family Engagement Project Leader, Beth Israel Deaconess Medical Center. SKB thanks The Schwartz Center for Compassionate Healthcare for their generous support of this work and of compassionate care.
References
Footnotes
Twitter Follow William Martinez at @DrWillMartinez
Contributors WM, DMB, PV, BS and SKB conceptualised and designed the programme and the study. SKB and WM managed the data collection. TL and SKB analysed and interpreted the data. TL and SKB drafted the first manuscript. All authors read and approved the final manuscript.
Funding Deutsche Forschungsgemeinschaft (LA-2344/2-1), Institutional National Research Service Award (T32HP10251), Institute for Professionalism and Ethical Practice at Boston Children’s Hospital, Schwartz Center for Compassionate Healthcare.
Competing interests None declared.
Ethics approval Institutional Review Board at Beth Israel Medical Center and Boston Children’s Hospital, Boston, MA.
Provenance and peer review Not commissioned; externally peer reviewed.