Article Text

Abstract
Background In the hospital setting, inadequate engagement between healthcare professionals and seriously ill patients and their families regarding end-of-life decisions is common. This problem may lead to medical orders for life-sustaining treatments that are inconsistent with patient preferences. The prevalence of this patient safety problem has not been previously described.
Methods Using data from a multi-institutional audit, we quantified the mismatch between patients’ and family members’ expressed preferences for care and orders for life-sustaining treatments. We recruited seriously ill, elderly medical patients and/or their family members to participate in this audit. We considered it a medical error if a patient preferred not to be resuscitated and there were orders to undergo resuscitation (overtreatment), or if a patient preferred resuscitation (cardiopulmonary resuscitation, CPR) and there were orders not to be resuscitated (undertreatment).
Results From 16 hospitals in Canada, 808 patients and 631 family members were included in this study. When comparing expressed preferences and documented orders for use of CPR, 37% of patients experienced a medical error. Very few patients (8, 2%) expressed a preference for CPR and had CPR withheld in their documented medical orders (Undertreatment). Of patients who preferred not to have CPR, 174 (35%) had orders to receive it (Overtreatment). There was considerable variability in overtreatment rates across sites (range: 14–82%). Patients who were frail were less likely to be overtreated; patients who did not have a participating family member were more likely to be overtreated.
Conclusions Medical errors related to the use of life-sustaining treatments are very common in internal medicine wards. Many patients are at risk of receiving inappropriate end-of-life care.
- Adverse events, epidemiology and detection
- Chronic disease management
- Communication
- Decision making
- Medical error, measurement/epidemiology
Statistics from Altmetric.com
- Adverse events, epidemiology and detection
- Chronic disease management
- Communication
- Decision making
- Medical error, measurement/epidemiology
Introduction
From the perspective of seriously ill, hospitalised elderly patients and their family members, effective communication and decision-making and open relationships with their healthcare providers are central to their construct of quality of end-of-life (EOL) care.1 There are great opportunities for the improvement of these practices.2 In a multicentre audit of communication practices in 12 hospitals in Canada, we used a validated questionnaire to interview patients and family members shortly after hospital admission to determine their perspectives about whether healthcare professionals engaged them in key processes of communication and assessed concordance between preferences for EOL care as stated by the patient and/or family member and medical orders for the use of life-sustaining treatments as documented by the physicians.3 We found that there was very little effective communication between the patient/family and members of the healthcare team about goals of care. This occurred despite the fact that most patients and family members had discussed among themselves options about life support near the EOL before admission to hospital and could clearly express their preferences for EOL care. In nearly 30% of cases in which patients and family members had reported a preference for the use (or non-use) of life-sustaining treatments, there was no documentation of a preference in the medical record. Even when preferences were documented, written orders for resuscitation (cardiopulmonary resuscitation, CPR) were discordant with the patients’ or family members’ expressed preferences in more than two-thirds of cases. Most of the discordance was related to the patient wishing for some limitation of life-sustaining technologies at the EOL, whereas documentation in the chart stated that the patient was to receive full resuscitation if necessary (‘full code’). We posit that these discordances are medical errors.
The term, ‘medical error’ has been defined as “the failure to complete a planned action as it was intended, or when an incorrect plan is used in an attempt to achieve a given aim”.4 In the case of EOL communication, the ‘intended action’, or the ‘given aim’ is to provide life-sustaining treatments to seriously ill hospitalised patients in a manner that is concordant with their preferences. To achieve this goal, these preferences must be known to healthcare providers before the time that care is provided. Therefore, to provide patient-centred care, preferences must be elicited accurately from the patient or substitute decision maker (often a family member) and be clearly documented in the patient's medical record. Two types of errors may occur in this context. First, equivalent to not having a plan at all, is a complete lack of communication and documentation. By default, aggressive life support would likely be offered in such cases, occasionally against a patient's preferences. Second, corresponding to using an incorrect plan, the documented goals of care may not reflect the patient's actual preferences, either because communication was ineffective or it was absent. These errors may result in opposite situations, each with possible serious implications: (1) Undertreatment—a patient who is interested in receiving CPR and is not ordered to receive it and suffers cardiac arrest and dies with no resuscitative attempts and (2) Overtreatment—a patient who desires ‘comfort management only’ but is ordered to be resuscitated and has a cardiac arrest and is resuscitated and transferred to the Intensive Care Unit (ICU). Although generally a small fraction of medical errors result in adverse events,5 in this case, the implications of errors in EOL communication can be serious. Specifically, errors stemming from poor EOL communication and documentation may potentially lead to inappropriate delivery, or withholding of care, unnecessary increase in healthcare costs, and patient and family dissatisfaction at the EOL. Thus, the purpose of this paper is to determine the prevalence and nature of errors related to EOL communication and documentation of preferences.
Methods
Given the importance of communication and decision-making at the EOL, we developed an audit tool to measure communication, decision-making and documentation practices in acute care settings (The Audit of Communication, CarE Planning, and documenTation or The ACCEPT Study, see http://www.thecarenet.ca for more information). Beginning in September 2011, we conducted three separate and sequential cross-sectional surveys or audits in acute care hospitals in Canada that ended in March 2015. The details of these audits have been previously published.3 We included a convenience sample of large hospitals in British Columbia, Alberta, Ontario and Quebec. Hospitalised patients were enrolled if they were 55–79 years old and had advanced pulmonary, cardiac or liver disease, metastatic cancer (see online supplementary appendix 1 for details), or if they were 80 years of age or older and admitted to hospital from the community for an acute medical or surgical condition. If none of the above criteria were met, any patient whose death within the next 6 months would not surprise any member of their care team was also included.6 For the purposes of this analysis, data sets from all three audits were combined.
In all audits, we administered a questionnaire7 during face-to-face interviews with patients and family members to assess the quantity and quality of EOL communication and decision-making. Potentially eligible patients were approached after day 2 of hospitalisation to allow for abatement of acute symptoms that were present at the time of admission. Patients were identified by the attending physician, medical residents, other healthcare team members and/or by a research coordinator. Patients unable to communicate due to language (unable to speak English or French) or cognitive reasons were excluded. However, if their family member was available, this person was approached independent of the patient. Otherwise, enrolled study patients were asked to identify an adult family member who knew them the best (inclusive of partners, significant others and/or close friends) and who had visited the patient in hospital at least once.
After enrolment, the research coordinator conducted separate face-to-face interviews with patients and their family members. The details of development and validation of the questionnaire used during this interview are described elsewhere.7 Questions assessed the extent to which patients had thought about the kinds of life-sustaining treatments they would or would not want in the context of a life-threatening or serious illness, what their preferences regarding life-sustaining treatments were, if they had shared those preferences with anyone, if so, with whom, and whether a doctor had discussed their prognosis with them. To elicit preferences for use of life-sustaining treatments, we used a taxonomy that varied slightly across the three audit cycles (see online supplementary appendix 2). In the last audit cycle, respondents were asked to pick the one that best represented their wishes: (1) Use machines and all possible measures including CPR with a focus on keeping me (or my family member) alive at all costs; (2) Use machines and all possible measures with a focus on keeping me (or my family member) alive but if my heart stops, no CPR; (3) Use machines only in the short term to see if I (or my family member) will get better but if my illness is prolonged, change focus to comfort measures only. If the heart stops, no CPR; (4) Use full medical care to prolong my life (or life of my family member) but if my heart or breathing stops, no CPR or breathing machines; (5) Use comfort measures only, with a focus on improving quality of life and comfort. Allow natural death and no artificial prolongation of life and no CPR; or (6) Unsure. In the first two audit cycles, participants could select a preference that contained a ‘mix’ of the above goals but did not explicitly state whether CPR was to be used or not. Because of this ambiguity, respondents who selected this preference were not used in this analysis.
We also sought to determine if the patients had formally documented these wishes in a written advance care plan or directive, whether they had formally documented their choice of substitute decision maker, and whether they were asked about these prior discussions or written documents upon admission to hospital. We asked family members about their wishes for the patient, not a proxy assessment of the patient's wishes.
After completion of the interview, on the same day, the research coordinator reviewed the medical record to determine documented orders regarding life-sustaining treatments including CPR using the same taxonomy/categories as for patient preferences. Demographic characteristics of the patients and family members were determined from direct interview of the patient and/or family or chart abstraction. We used the Clinical Frailty Scale, a well validated 8-point assessment tool, to define frailty.8 At the end of hospital stay, the chart was reviewed to determine use of CPR and palliative care consultations.
Statistical analysis
Demographics of patients and their family members are described as means, SDs and ranges for continuous variables and as counts and percentages for categorical variables. Concordance between stated preferences and documented goals of care was calculated for subjects who had both of these items available; patients who had missing data or who were ‘unsure’ of their preferences were excluded from these analyses. If the patient preferred CPR and if there were no documented goals of care on the chart, the case was considered concordant because the default in all participating institutions was to resuscitate these patients. If patients preferred not to be resuscitated and there was no documentation, such cases were considered to be discordant and consistent with a medical error. Given that not all levels of disagreement could be considered of equal severity, we analysed the disagreement between expressed preferences and documented orders for the use of life-sustaining treatments, focusing on the use (or not) of CPR. For example, if the patient/family member preferred CPR but the documented orders indicated withholding of CPR, this situation was called potential undertreatment. If expressed preferences were for no CPR but the documented orders indicated that CPR would be provided (if needed) or there were no documented goals of care (default to receive CPR), this situation was called potential overtreatment. We also examined an extreme subset of potential overtreatment in which the patient/family member preferred comfort measures only but the documented order indicated that they would receive CPR. To evaluate the effect of using family members who were not substitute decision-makers as informants in this study, we conducted a sensitivity analysis where we excluded those family members who were not substitute decision-makers and evaluated the impact on concordance and medical error rates.
Variations in concordance and medical error rates across participating sites were also assessed by reporting average, maximum and minimum site medical error rates for patients and family members. Sites contributing responses from 5 or patients or family members were excluded from this analysis given the paucity of site data.
Finally, we used regression modelling to determine, when controlling for site, which patient characteristics are associated with potential overtreatment. We included all patient characteristics reported in table 1 as covariates. In addition, we added a variable to denote whether only the patient participated in the study or patient and his/her family member participated. This study was approved by the Research Ethics Boards of all participating institutions and all participants provided written informed consent.
Patient demographics
Results
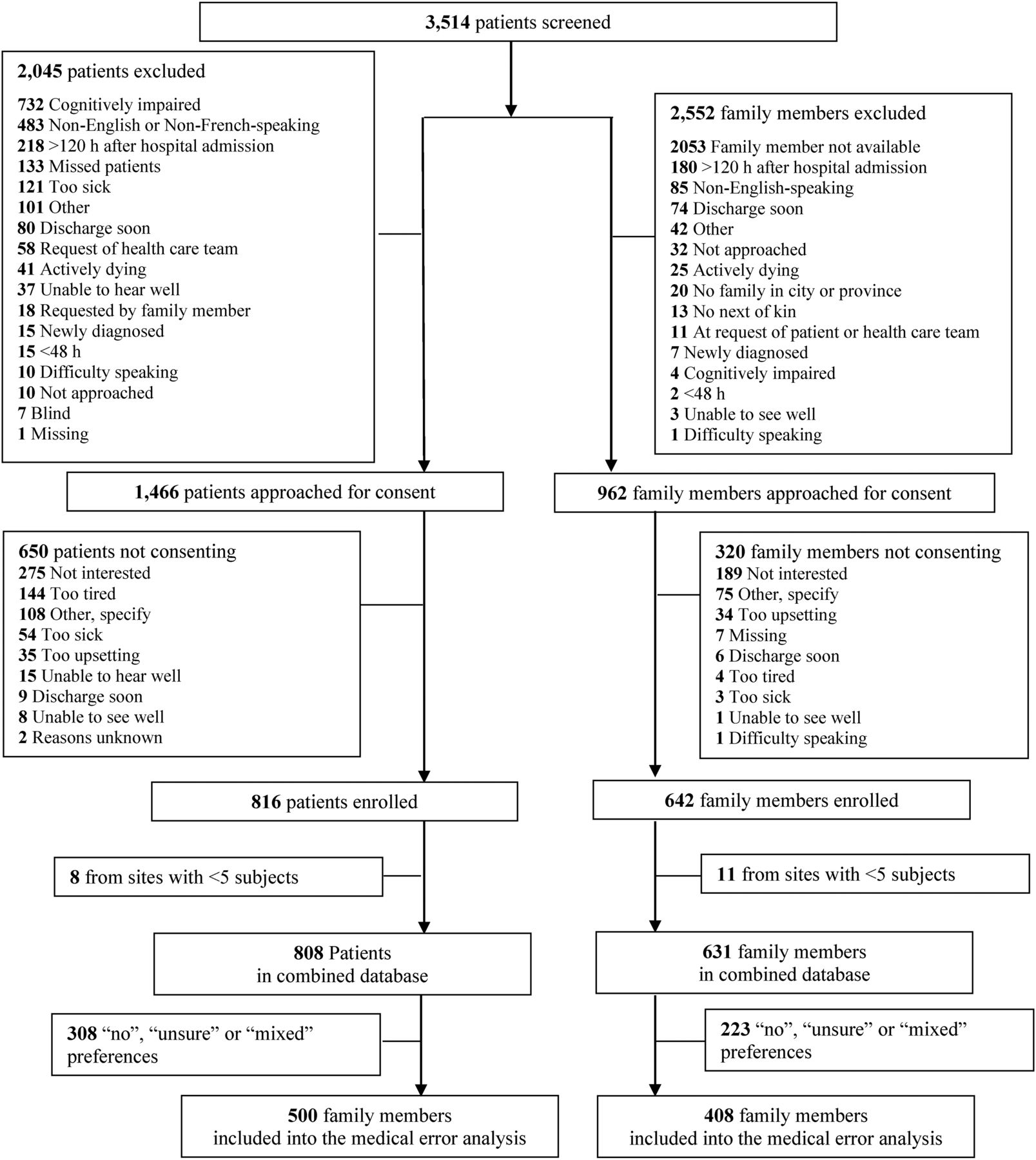
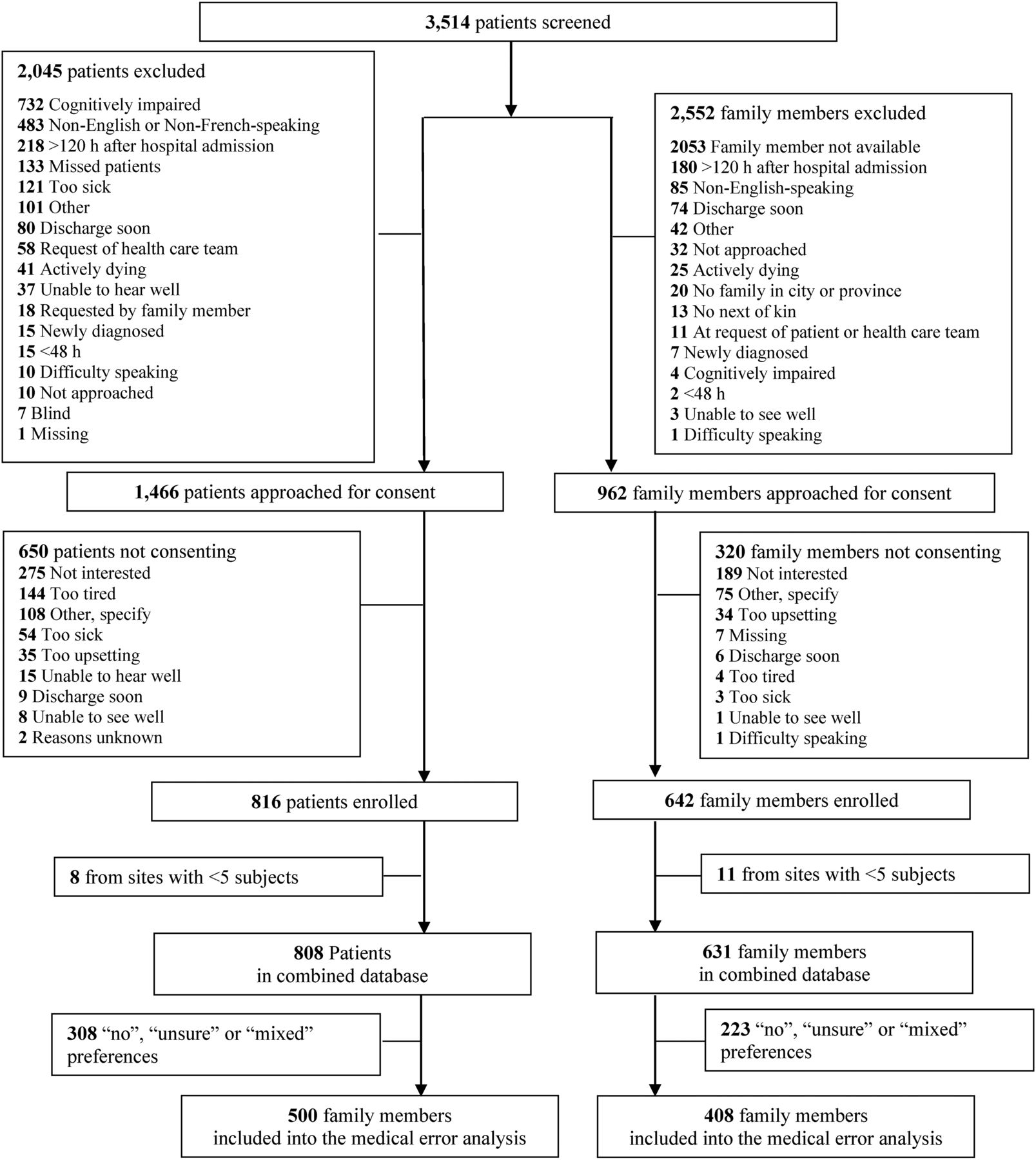
At 16 hospitals, we approached a total of 1466 eligible patients and 962 potentially eligible family members; 816 patients and 642 family members consented, yielding an enrolment rate of 56% and 67%, respectively (figure 1). Of the 642 participating family members, in 295 cases (46%), the corresponding patient participated as well; for the remaining 347 family members (54%), the patient did not participate, usually because they were too unwell. The average age of the participating patients was 80 years (table 1). The average age of the participating family members was 61 years and most were children of the patient (58%; table 2). Most patients and family members were Caucasians. In 397 out of the 500 patients (80%), a standardised folder or any other strategy to easily localise Advance Care Planning (ACP)/advance directives (AD) tools in the medical record was supposed to be used according to local hospital policies. However, only in 238 patients (60%) could research staff find the specialised folder.
Family member demographics
{kind=link}
Flow diagram of patients and families involved in this study.
As shown in table 3, most patients preferred either comfort care (29%) or some limitation of medical care that does not include CPR (50%) whereas only 12% preferred life support including resuscitation (table 3). Similarly, family members more commonly preferred comfort care (33%) or some limitation of medical care that does not include CPR (48%) whereas only 13% preferred life support including resuscitation for their loved ones (table 3). Less than 10% of patients and families were unsure of their preferences (table 3). We were unable to elicit preferences in seven (1%) patients and four (1%) family members. During this index hospitalisation, only one patient actually received CPR. Palliative care consultations were used in 44 (9%) of patients and rates did not defer between patients with and without a medical error.
Expressed preferences for end-of-life care
Medical error rates
From the calculation of medical error rates, we excluded 308 patients and 223 family members because of no preference information available, ‘unsure’ preferences, or it was unclear if they wanted CPR or not (figure 1). Documentation of medical orders for life-sustaining treatment was not found for 122 (15%) of patients; across sites, this omission ranged from 0% to 50%. Raw concordance between patients’ and family members’ expressed preferences, and documentation of orders for life-sustaining treatment in the medical record was 35% and 33%, respectively (table 4). As judged by comparing expressed preferences and documented orders for use of CPR, 37% of patients experienced a medical error. Very few patients (8, 2%) expressed a preference for CPR and had CPR withheld in their documented medical orders (potential undertreatment, table 4). Of patients who preferred not to have CPR, 80 (16%) had orders to receive it and 94 (19%) had no documented goal of care orders and thus, by default, would receive CPR in the event of a crisis/life-threatening event (Total potential overtreatment error rate: 174 (35%)). A subset of this last group, 34 (7%) preferred comfort measures only and had documented orders to receive CPR. Similar findings were observed based on family members’ preferences and documented orders for life-sustaining treatments in the patient's chart (table 4). Results did not change appreciably when family members who were not substitute decision-makers were excluded from the analysis (concordance remained the same at 33.1% and medical error rates went from 46.8% to 49.6%).
Concordance between expressed preferences and documented goals
There was wide variation in concordance and medical error rates across sites (table 5). From a patient's perspective, medical error rates varied from a minimum of 25% to a maximum of 67% across 16 sites. From a family member's perspective, medical error ranged from 19% to 82% across 14 sites. The majority of the errors related to potential overtreatment, which ranged from 14% to 82% (table 5). Potential overtreatment in the ‘comfort only’ subgroup ranged from 0% to 23%.
Medical error rates by site
Patients who were frail were less likely to be potentially overtreated (OR 0.7, 95% CI 0.5 to 0.9, p=0.004). There was a tendency for patients who had end-stage disease to be less likely to be potentially overtreated (OR 0.5, 95% CI 0.3 to 1.1, p=0.09). Patients whose family members did not participate in this study tended to be more likely to be potentially overtreated (95% CI 0.8 to 1.5, p=0.15) (eTable 1).
Discussion
In this multicentre observational study, we elicited patients’ and family members’ preferences for the use of life-sustaining measures and compared these preferences to documented orders. The majority of these older, hospitalised patients and their participating family members expressed a preference for comfort care only. It is noteworthy that 15% of patients did not have any documentation regarding the use of life-sustaining treatment but for those who did, we found poor agreement between these expressed preferences and documented orders for these life-sustaining treatments. Crude agreement was less than 30%. There is a range of discordance between preferences and orders, not all situations are equally as harmful (or potentially harmful). We focus on the situation when a patient requests CPR and there are orders not to receive it, or more commonly, when a patient prefers not to be resuscitated and there are orders to receive it. These medical errors occurred in approximately a third to a half of cases from a patient's perspective and from a family member's perspective, respectively. Moreover, these error rates varied widely across all participating sites (from 14% to 82%). Frailty and the presence of significant end-stage disease were associated with a lower risk of potential overtreatment whereas the absence of a participating family member was associated with a greater risk of potential overtreatment. It is notable that low health literacy was not associated with potential overtreatment, suggesting that these patients can meaningfully participate in EOL conversations without increased risk of potential overtreatment (or undertreatment).
The results of this larger, multi-institutional audit using a combined data set are consistent with our previously reported findings from our first audit that also highlight poor concordance between expressed preferences and documented orders but further elaborate the nature of the disagreement.3 The most common form of disagreement, potential overtreatment, is when the patient expresses a desire not to be resuscitated but CPR is ordered (or assumed to be ordered) in the medical record. These findings are consistent with other reports in the literature in other clinical settings that document significant overtreatment at the EOL due principally to poor communication.9 ,10 This discordance has significant potential for harming patients (and their families) and is inconsistent with patient-centred care.
There are also significant economic implications of these medical errors. Inadequate (or absent) EOL conversations are associated with increased intensification of care leading to increased costs of care.11 Millions of dollars per year of wasted healthcare resources could be recovered if we could solve this problem and stop providing unwanted treatments to seriously ill hospitalised patients.9 Moreover, there is an opportunity cost because resources for healthcare are finite. There is considerable demand for critical care services and those demands are likely to increase as society ages and more people live with advanced, serious illnesses. If ICU beds are full and occupied by patients who receive unwanted treatment, then beds will not be available to other patients who might benefit from critical care. Delays in accessing ICU care have been shown to increase patient morbidity and mortality.12
What are the possible sources of error in the EOL communication and decision-making process that may explain our findings? The placement of medical orders for life-sustaining treatments in a patient's chart is the final step in a complex process, which includes reflection, discussion, education and advice-giving, decision-making, and finally documentation. Each of these steps can be affected by various human and system-related factors, barriers and challenges, including time and space, skills and expertise, the availability of established processes, and the need to provide social and emotional support to patients and their families. Examining this situation using a system-based analysis can identify multiple contributing factors, including patient, provider, team, training, task and environment-related factors.13 Although many patients have considered their preferences regarding EOL care before the hospital admission, a considerable proportion have not.3 Furthermore, due to physical and cognitive dysfunction surrounding an acute illness, or simply to avoid emotional distress, many clinicians have not initiated a conversation about EOL with their patients. Furthermore, the task of discussing and documenting patients’ goals of care may not be supported by well established procedures and protocols in many organisations. Consequently, EOL communication may not be routinely integrated into providers’ workflow. In a prior publication,14 we explicated the key communication steps related to establishing goals of care. Patients and family members identified the following elements as most important to discuss: (1) preferences for care in the event of life-threatening illness, (2) values, (3) prognosis, (4) fears or concerns, and (5) questions about goals of care; but also reported that clinicians infrequently discussed/broached these issues with them. However, addressing more elements of goals of care discussions was associated with greater concordance between patients’ preferences and prescribed goals of care and with greater patient satisfaction. If healthcare providers engaged more frequently in these five communication processes, the incidence of medical errors related to communication at the EOL (and its attendant consequences) could be reduced.
Even if conversations happen and are documented, the misinterpretation of documented orders may lead to errors.15 In a survey of emergency room physicians, there was wide variation in the application of life-sustaining treatments to patients with document physician orders for the use of life-sustaining treatments suggesting the training and/or safeguards need to be in place to ensure patients are receiving the treatments that are ordered.
Finally, the clinical environment poses various barriers and challenges, including time constraints, various distractions and competing objectives, so that EOL communication may lose priority, and providers may lose situational awareness regarding this task. For example, the Study to Understand Prognoses and Preferences for Outcomes and Risks of Treatments demonstrated that over half of attending physicians were unaware of their patients’ treatment preferences.16 The relevance of any of these factors to different healthcare organisations, and specific units, may vary as does the safety climate.17 This is illustrated by the fact that medical error and concordance rates varied considerably across our sites. Therefore, the measures necessary to address this problem need to be specifically designed for different organisations and clinical areas. Nevertheless, perhaps something can be learned from top performing sites that can be disseminated to other sites.
Strengths of this study include the ‘real time’ assessment of preferences and objective measures of concordance between these preferences and documented orders for life-sustaining treatments. The multiyear, multicentre nature of the study increases the generalisability of the findings. However, our study population is limited to mostly Protestant Caucasians who speak English. We are uncertain if these estimated event rates apply to other religious or minority groups in Canada and hypothesise, given the communication and EOL decision-making difficulties with such groups, that medical error rates might even be higher or at least, the nature of the medical error may be different. Another potential limitation is that the patient's preference when stated to the research nurse during our research interview may not be an accurate reflection of what their ‘true’ preference would be if the attending physician could help to put the decision into the context of what is actually going on with the patient during the hospital admission.
Conclusions
Medical errors related to communication about EOL treatments are very common in internal medicine wards across Canada, and many older patients in these wards are at risk of receiving inappropriate EOL care. There is a striking variability in medical error rates across hospitals. Patients who are frail and have significant advanced medical disease have a lower risk of potential overtreatment whereas older patients who do not have attendant family members have a higher risk of potential overtreatment. A system-based approach, geared to the relevant needs of individual clinical areas is required to address the communication and documentation failings highlighted in this analysis.
Acknowledgments
The authors thank the research coordinators at the following sites for their support conducting the study: Carol Mantle (Hamilton General Hospital); Christine Welsh (Ottawa Civic and General Hospitals); Lauren Ogilvie, Gail Gonyea, Lisa Sinclair, Tess Topor (Calgary Zone Hospitals, Alberta Health Services); LeeAnn Esau, Sarah Borland, (Chinook Regional Hospital) Pat Porterfield, Sandy MacDonaldis (Vancouver General Hospital); Reihbar Hans (Burnaby and Royal Columbian Hospitals, British Columbia); Betty Jean Ashley, Janice Palmer, Lucia Milosavljevic (St. Paul's Hospital, Vancouver). The authors also thank the staff at the Clinical Evaluation Research Unit at the Kingston General Hospital for their support with coordinating the study (Jennifer Korol) and analysing the results (Xuran Jiang and Andrew Day). In addition, the authors also thank the other members of the ACCEPT study team for their contributions to the development of the study protocol or support with data collection: Bert Enns, Jim Kustogiannis, James Downar, Nora Cummins and Ana Johnson.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Collaborators The ACCEPT Study Team and the Canadian Researchers at the End of Life Network (CARENET).
Contributors All coauthors participated in all stages of the manuscript; including the planning, conduct, reporting, drafting and finalisation of the manuscript.
Funding Alberta Innovates—Health Solutions; Michael Smith Foundation for Health Research (PJ HSP 00001 (10-1)); Canadian Institutes of Health Research (114117).
Competing interests None declared.
Ethics approval Queen's University Research Ethics Board.
Provenance and peer review Not commissioned; externally peer reviewed.